




Persistent truncus arteriosus is a birth defect in which a single, large blood vessel (a truncus) exits the heart, instead of a separate pulmonary artery and aorta. The pulmonary artery comes off the truncus directly and a ventricular septal defect is always present. Deoxygenated blood from the right side of the heart and oxygenated blood from the left side of the heart both enter this single large vessel (the truncus arteriosus), and a mixture of oxygenated and deoxygenated blood then flows to the body and lungs.
Symptoms include a bluish coloration of the skin (cyanosis) and symptoms of heart failure, including shortness of breath, poor feeding, sweating, and rapid breathing.
Diagnosis is by echocardiography.
Medical treatment for heart failure is typically followed by early surgical repair.
(See also Overview of Heart Defects.)
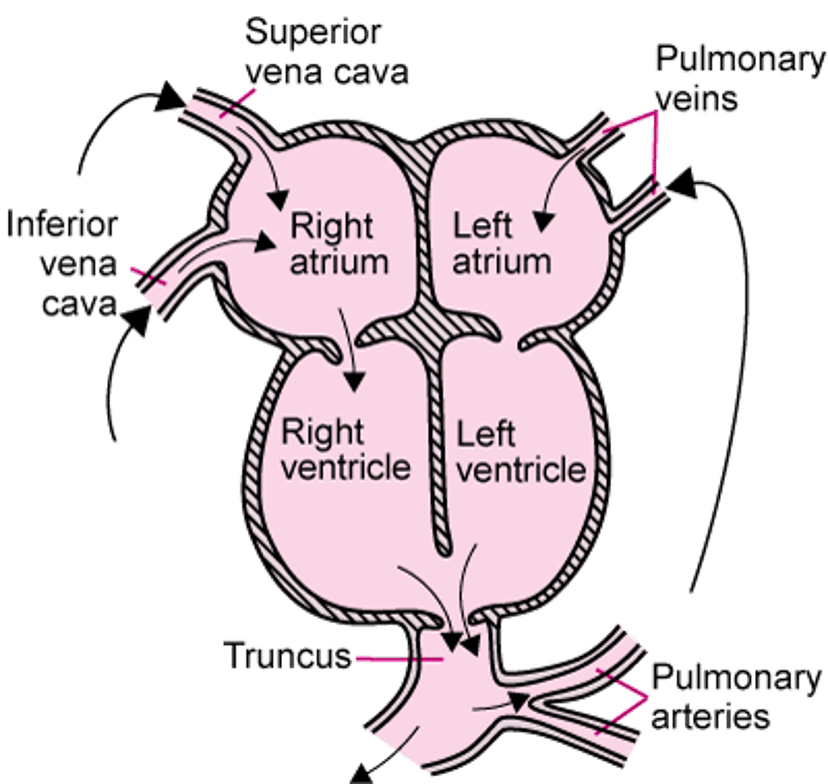
When the heart and blood vessels develop in the fetus, at first there is only one large tube, called the truncus, leaving the heart. Normally, the truncus divides into two blood vessels, the pulmonary artery and the aorta (see also Normal Fetal Circulation). Sometimes the truncus does not divide. There is one valve, the truncal valve, leading into this one artery, rather than separate aortic and pulmonic valves. A single artery arises from the heart, which then gives rise directly to the pulmonary arteries. Invariably, a ventricular septal defect is present, which allows both the right and left ventricles to pump blood across the truncal valve.
Persistent truncus arteriosus accounts for 1 to 2% of birth defects of the heart. Other abnormalities may be associated with persistent truncus arteriosus.
Persistent Truncus Arteriosus
Persistent truncus arteriosus occurs when, during fetal development, the developing truncus does not divide into the pulmonary artery and aorta, resulting in a single, large, blood vessel that exits the heart. As a result, blood that contains oxygen (oxygenated blood) and blood that does not contain oxygen (deoxygenated blood) mix together and enter the body and the lungs. |

Symptoms of Persistent Truncus Arteriosus
During the first few weeks of life, infants with persistent truncus arteriosus usually have mild cyanosis (bluish coloration of the skin) and symptoms and signs of heart failure (see figure Heart Failure: Pumping and Filling Problems), including shortness of breath, rapid breathing, poor feeding, and sweating.
Diagnosis of Persistent Truncus Arteriosus
Echocardiography
Occasionally cardiac catheterization, cardiac magnetic resonance imaging (MRI), or computed tomography (CT) angiography
Doctors suspect the diagnosis based on findings during their examination of the newborn, including characteristic heart murmurs and bounding (strong throbbing) pulses. A heart murmur is a sound created by turbulent blood flow through narrowed or leaking heart valves or through abnormal heart structures.
Findings from chest x-rays and ECG, done when doctors suspect a heart defect, usually provide further clues to the diagnosis. Echocardiography (ultrasonography of the heart) confirms the diagnosis.
Cardiac catheterization, MRI, or CT is occasionally used to identify other coexisting heart problems before surgery.
Treatment of Persistent Truncus Arteriosus
Surgical repair
Medication to treat heart failure before surgery
Heart failure is treated with medications to improve breathing and stabilize the infant until surgery can be done.
Surgery is usually done before the infant is 1 to 2 months old. The ventricular septal defect is repaired with a patch that directs all blood flow from the left ventricle to the truncal valve. Then doctors separate the pulmonary arteries from the truncus and attach them to the right ventricle using a tube (conduit). After this repair, the truncus functions as the aorta.
When a conduit is placed during early infancy, its size becomes inadequate as children grow, and additional surgery is needed to enlarge the conduit.
After surgical repair, affected children need to take antibiotics before visits to the dentist and before certain surgeries (such as on the respiratory tract). These antibiotics are used to prevent a serious heart infection called endocarditis.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides an overview of common birth defects of the heart for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing antibiotic use, for parents and caregivers






