




Hip dislocations occur when the ball-shaped head of the thighbone (femur) pops out of the rounded socket of the hip bone (pelvis).
Usually, hips are dislocated when a great force hits a bent knee and pushes the head of the thighbone backward—for example, when a knee hits the dashboard in a car accident.
People with a hip dislocation often have other injuries.
The hip is very painful, and usually people cannot move their leg.
Doctors diagnose these dislocations by examining the hip and taking x-rays.
Doctors can usually put the hip back in place without surgery, typically after giving the person drugs to make the procedure more tolerable.
(See also Overview of Dislocations.)
In most hip dislocations, the head of the thighbone is pushed backward—called a posterior hip dislocation. These dislocations usually occur when the knee and hip are flexed (as when sitting down) and a great force hits the knee. A common cause is hitting the knee against the dashboard of a car in a crash. Hip dislocations can also occur when people fall from a high place (such as a ladder) or play a contact sport (such as football and rugby). In older people, much less force is needed to dislocate a hip.
The force that causes the hip dislocation often also causes other injuries. For example, when a hip dislocation results from a fall or an athletic injury, the pelvis, knee, or legs may be fractured, and the back or head may be injured.
When the hip is dislocated, bones may be broken, and nerves, including the sciatic nerve (see Sciatica), may be injured. The blood supply to the head of the thighbone may be disrupted, causing bone tissue to die (called osteonecrosis).
An artificial hip joint may also be dislocated. It is sometimes dislocated after an injury but can occur while people are doing their usual daily activities, even when crossing their legs.
Symptoms of a Dislocated Hip
Hip dislocations are very painful. People usually cannot move their leg.
When the thighbone is pushed backward, the affected leg looks shorter and turns inward.
When the thighbone is pushed forward, the leg turns outward. It looks shorter but not as obviously as when the thighbone is pushed backward.
If nerves are damaged, parts of the foot and ankle may feel numb.
Diagnosis of a Dislocated Hip
X-rays
If people think that their hip is dislocated, they should not be moved. They should be taken to an emergency department, usually by ambulance.
Doctors can usually identify a dislocated hip when they examine the area. X-rays are taken to confirm the diagnosis and check for fractures.
Treatment of a Dislocated Hip
Maneuvers to put the hip back in place
Possibly bed rest or immobilization for a short time
Physical therapy
If hip dislocation is the only injury or the most serious injury, doctors put the hip back in place (called reduction) as soon as possible. Any delay increases the risk that bone tissue will die. Surgery is not necessarily required.
Before hip reduction, people are given a sedative (usually by vein), pain reliever, and muscle relaxant, but they may remain conscious. Or they may require a general anesthetic (making them unconscious) or an anesthetic injected around the spinal cord to make them numb from the waist down.
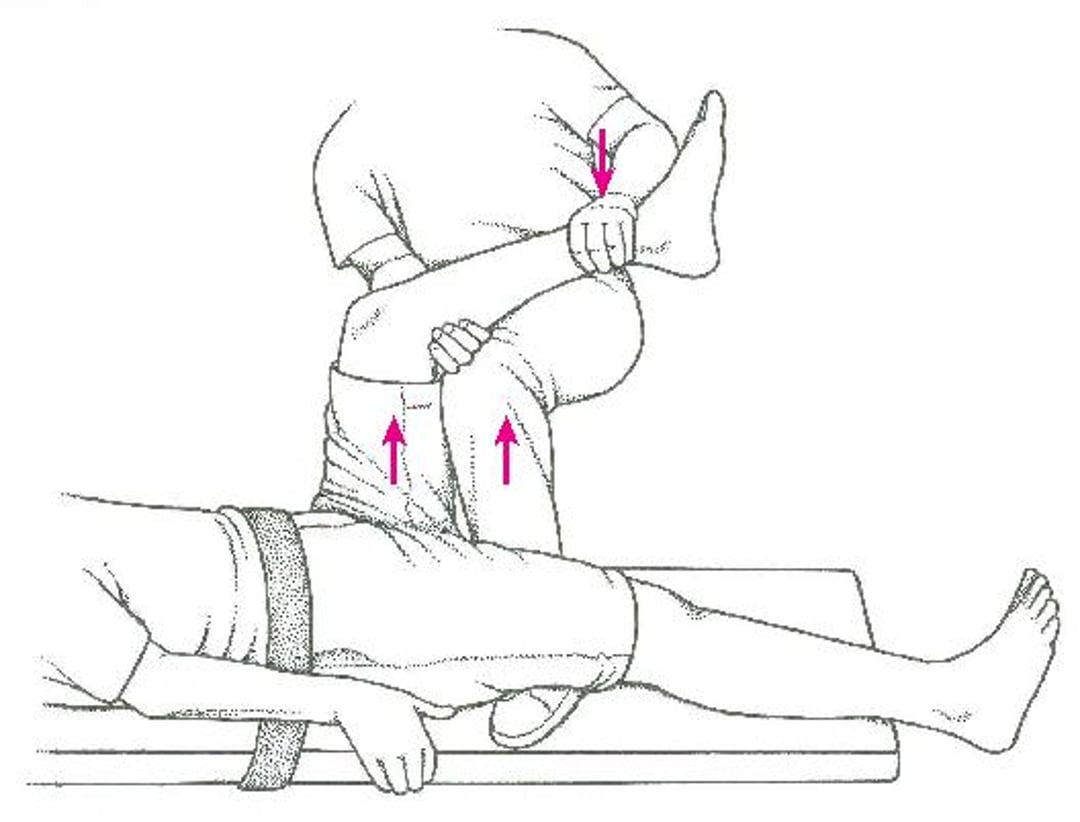
One of several maneuvers can be used to put the hip back in place. In one maneuver (Captain Morgan technique), a person lies face up, usually on a rigid board on the floor. The person's hips are held down by a sheet or belt, and a practitioner gently bends the person's knee and moves it so that it is over the hip joint. Practitioners then place their knee under the person's knee and lift up under the knee while pushing down on the ankle.
Reducing a Hip Dislocation: Captain Morgan Technique
For this technique, the person lies face up, usually on a rigid board on the floor. The person's hips are held down by a sheet or belt, and a practitioner gently bends the person's knee and moves it so that it is over the hip joint. Practitioners then place their knee under the person's knee and lift up under the knee while pushing down on the ankle. |

After reduction, computed tomography (CT) is done to check for fractures and for any debris or fragments of bone or cartilage in the joint. If any are found, doctors consult an orthopedic surgeon about whether surgery is needed.
If no fractures, debris, or fragments are found, most people with a posterior hip dislocation are sent home with crutches. They are instructed that their foot on the injured side may touch the floor—for example, to help with balance—but they should not put any weight on it.
Follow-up visits with an orthopedist are needed. People should not put weight on their foot until their orthopedist says they can.
Most people can walk without crutches in about 1 week. People who have certain types of dislocations may need crutches longer or, rarely, permanently.
Bed rest is not recommended because it increases the risk of complications such as blood clots.
If there are other injuries, surgery may be needed to repair them.
Right after a person has surgery for a dislocated hip, a physical therapist usually gently exercises the person's joint (called passive exercise), sometimes using a continuous passive motion machine.






