

Cervical cancer develops in the cervix (the lower part of the uterus). Most cervical cancers are caused by human papillomavirus (HPV) infection.
Cervical cancer usually results from infection with the human papillomavirus (HPV), which is transmitted during sexual contact.
The first symptom is usually irregular vaginal bleeding, usually after sexual activity, but symptoms may not occur until the cancer has enlarged or spread.
Cervical cancer screening tests (Papanicolaou [Pap] tests and/or HPV testing) can usually detect abnormalities, which are then biopsied.
Treatment usually involves surgery to remove the cancer and often the surrounding tissue and often, if tumors are large or have spread, radiation therapy and chemotherapy.
(See also Overview of Female Reproductive System Cancers.)
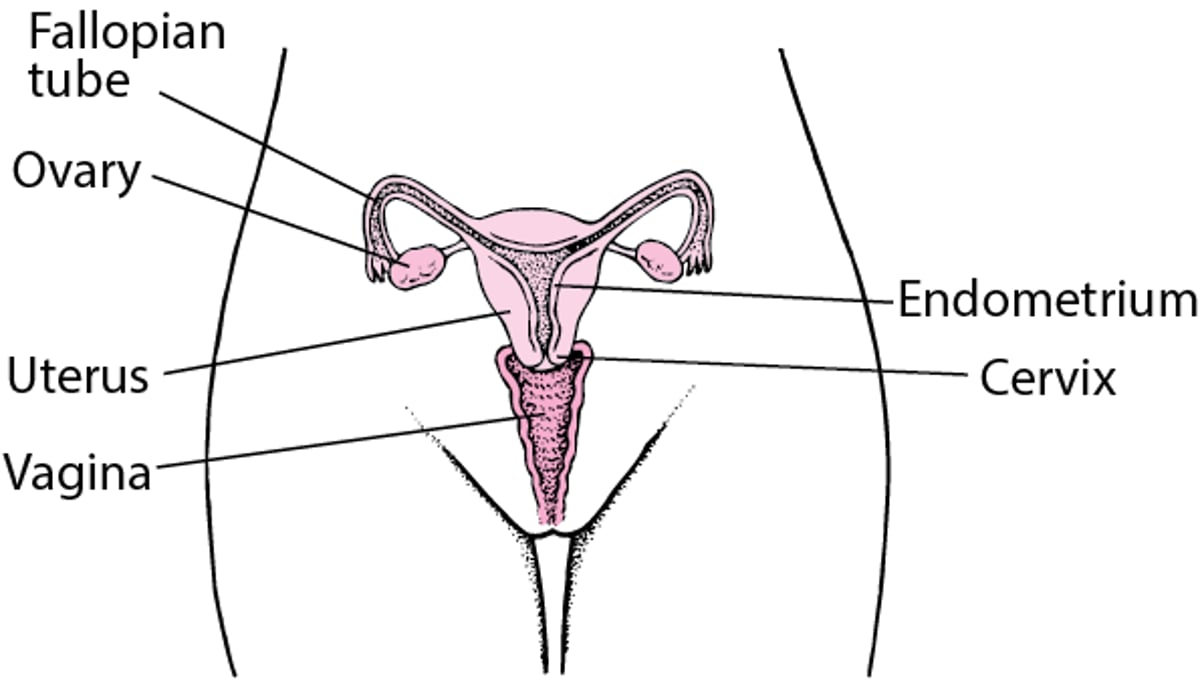
The cervix is the lower part of the uterus. It extends into the vagina.
In the United States, cervical cancer (cervical carcinoma) is the third most common gynecologic cancer among all women and is common among younger women. The average age at diagnosis is about 50 years, but it is most often diagnosed in women aged 35 to 44 years.
Worldwide, most cervical cancer cases (almost 85%) and deaths due to cervical cancer (almost 90%) occur in low- and middle-resource countries. Cervical cancer is the most common cancer among females in 23 countries and the leading cause of cancer death in 36 countries.
Internal Female Reproductive Anatomy

Approximately 80 to 85% of cervical cancers are squamous cell carcinomas, which develop in the flat, skinlike cells that line the cervix. Most other cervical cancers are adenocarcinomas, which develop from gland cells.
Cervical cancer begins with slow, progressive changes in cells on the surface of the cervix. These changes, called dysplasia or cervical intraepithelial neoplasia (CIN), are considered precancerous. That means that if untreated, they may progress to cancer; sometimes this takes several years. CIN is classified as mild (CIN 1), moderate (CIN 2), or severe (CIN 3).
Cervical cancer begins on the surface of the cervix and can penetrate deep beneath the surface. Cervical cancer can spread in the following ways:
By spreading directly to nearby tissues, including the vagina
By entering the rich network of lymphatic vessels inside the cervix, then spreading to other parts of the body
Rarely, by spreading through the bloodstream
Causes of Cervical Cancer
Precancerous changes in cervical cells (cervical intraepithelial neoplasia) and cervical cancer are almost always caused by the human papillomavirus (HPV), which is transmitted through sexual contact. The HPV virus can also cause genital warts or cancer of the vagina, vulva, or anus. Rates of cervical cancer have decreased steadily over the past several decades in countries that have access to HPV vaccines, cervical cancer screening, and treatment of cervical intraepithelial neoplasia.
Risk factors for developing cervical cancer include the following:
Having an increased chance of exposure to sexually transmitted infections (for example, having sexual intercourse for the first time at a young age, having more than one sex partner, or having sex partners who have risk factors for sexually transmitted infections)
Using oral contraceptives (birth control pills)
Smoking cigarettes
Having had precancerous changes or cancer in the vulva, vagina, or anus
Having a weakened immune system (due to a disorder such as cancer or AIDS or to medications such as chemotherapy drugs or corticosteroids)
HPV can be transmitted through any kind of sexual activity, including oral, genital, or anal contact. HPV infection is very common, and approximately 80% of sexually active people are exposed to HPV infection at least once during their lifetime. Many HPV infections last only a short time, but some people can be infected with HPV more than one time, and some HPV infections last for years.
Symptoms of Cervical Cancer
Precancerous changes and early cervical cancer often do not cause symptoms.
The first symptom of cervical cancer is usually abnormal bleeding from the vagina, most often after sexual activity. Spotting or heavier bleeding may occur between periods, or periods may be unusually heavy. Large cancers are more likely to bleed and may cause a foul-smelling discharge from the vagina and pain in the pelvic area.
If the cancer is widespread, it can cause lower back pain and swelling of the legs. The urinary tract may be blocked, and without treatment, kidney failure can result.
Diagnosis of Cervical Cancer
Papanicolaou (Pap) tests
Biopsy
Routine Pap tests can detect abnormal, precancerous cells (dysplasia) on the surface of the cervix. Doctors check women with precancerous cells at regular intervals. Dysplasia can be treated, thus helping prevent cancer.
Biopsy
If a growth or another abnormal area is seen on the cervix during a pelvic examination or if a Pap test detects precancerous or cancerous cells, a biopsy is done. Usually, doctors do a procedure called colposcopy using an instrument with a binocular magnifying lens (colposcope), inserted through the vagina, to examine the cervix and to choose the best biopsy site.
Two different types of test are done:
Cervical biopsy: A tiny piece of the cervix, selected using the colposcope, is removed.
Endocervical curettage: Tissue is scraped from inside the cervix.
These tests are similar to having a Pap test. They usually cause only mild pain and a small amount of bleeding.
If the diagnosis is not clear, a cone biopsy is done to remove a larger cone-shaped piece of tissue. Usually, a thin wire loop with an electrical current running through it is used. This procedure is called the loop electrosurgical excision procedure (LEEP). It requires only a local anesthetic. Alternative techniques are to use a scalpel (cold knife) or a laser (a highly focused beam of light). These procedures require an operating room and usually a general anesthetic.
Staging of cervical cancer
If cervical cancer is diagnosed, its exact size and locations (its stage) are determined. Staging begins with a physical examination of the pelvis and a chest x-ray. Usually, computed tomography (CT), magnetic resonance imaging (MRI), or a combination of CT and positron emission tomography (PET) is done to determine whether the cancer has spread to nearby tissues or to distant parts of the body. If these procedures are not available, doctors may do other imaging procedures to check specific organs, such as cystoscopy (bladder), sigmoidoscopy (colon), or IV urography (urinary tract).
Doctors usually also check for spread to the lymph nodes by doing imaging tests or a biopsy. Knowing whether cancer has spread to the lymph nodes and how many lymph nodes are involved helps doctors predict the person's outcome and plan treatment.
Stages of cervical cancer range from I (the earliest) to IV (advanced). Staging is based on how far the cancer has spread:
Stage I: The cancer is confined to the cervix.
Stage II: The cancer has spread outside the uterus, to the upper two thirds of the vagina or to tissues outside the uterus, but is still within the pelvis (which contains the internal reproductive organs, bladder, and rectum).
Stage III: The cancer has spread throughout the pelvis and/or the lower third of the vagina and/or blocks the ureters and/or causes a kidney to malfunction and/or spreads to the lymph nodes near the aorta (the largest artery in the body).
Stage IV: The cancer has spread outside the pelvis and/or to the bladder or rectum or to distant organs.
Treatment of Cervical Cancer
Surgery, radiation therapy, and/or chemotherapy
Treatment of cervical cancer depends on the stage of the cancer. It may include surgery, radiation therapy, and chemotherapy.
Precancerous changes and early stage I cervical cancer
Precancerous cervical cells (cervical intraepithelial neoplasia) and cervical cancer that involves only the surface of the cervix (early stage I) are treated the same way. Doctors can often completely remove the cancer by removing part of the cervix with a cone biopsy procedure. They may use the loop electrosurgical excision procedure (LEEP), a laser, or a scalpel. These treatments preserve a woman’s ability to have children.
Removal of the uterus (hysterectomy) may be done if women are not interested in preserving their ability to have children. If some cancer remains after the cone biopsy, hysterectomy or another cone biopsy may be done.
If early-stage cancer has spread deeply into the cervix or into blood vessels or lymphatic vessels, a modified radical hysterectomy is done, and nearby lymph nodes are removed. A modified radical hysterectomy involves removing the cervix and some of the tissue next to it (called the parametrium). But unlike a standard radical hysterectomy, the modified radical hysterectomy involves removing only half of the parametrium.
Lymph nodes may be checked for spread of cancer cells with a procedure called sentinel lymph node mapping.
Another treatment option is external radiation therapy plus radioactive implants placed in the cervix to destroy the cancer (a type of internal radiation called brachytherapy).
Radiation therapy may irritate the bladder or rectum. Later, as a result, the intestine may become blocked, and the bladder and rectum may be damaged. Also, the ovaries usually stop functioning, and the vagina may narrow.
Late stage I and early stage II cervical cancer
If cervical cancer involves more than the surface of the cervix but the cancer is still relatively small, treatment is typically
Radical hysterectomy (a hysterectomy plus removal of surrounding tissues including the upper part of the vagina and ligaments) and evaluation of lymph nodes
Hysterectomy is done by making a large incision in the abdomen (open surgery) or by using a thin viewing tube (laparoscope) and specialized surgical instruments inserted through small incisions just below the navel. Research suggests that when open surgery is done, the cancer is less likely to return and women are more likely to live longer than when laparoscopic surgery is done.
If the cancer has grown or has begun to spread within the pelvis, treatment is typically
Radiation therapy plus chemotherapy
The ovaries are usually left in place because cervical cancer is unlikely to spread (metastasize) to the ovaries.
If during surgery, doctors discover that cancer has spread outside the cervix, hysterectomy is not done, and radiation therapy plus chemotherapy is recommended.
Late stage II through early stage IV cervical cancer
When cervical cancer has spread further within the pelvis or has spread to other organs, the following treatment is preferred:
Radiation therapy plus chemotherapy
Doctors may use positive emission tomography with computed tomography (PET-CT) to determine whether lymph nodes are involved and thus determine where radiation should be directed. External radiation (directed at the pelvis from outside the body) is used to shrink the cancer and treat cancer that may have spread to nearby lymph nodes. Then radioactive implants are placed in the cervix to destroy the cancer (a type of internal radiation called brachytherapy).
Chemotherapy is usually given with radiation therapy, often to make the tumor more likely to be damaged by radiation therapy.
Extensive spread or recurrence of cervical cancer
The main treatment for extensive spread or recurrence of cervical cancer is
Chemotherapy
However, chemotherapy reduces the cancer’s size and controls its spread in almost half of women treated, and the beneficial effect is usually only temporary. Adding another medication (such as monoclonal antibodies used to treat several types of cancer; this is called immunotherapy) may extend survival by a few months.
If the cancer remains in the pelvis after radiation therapy, doctors may recommend surgery to remove some or all pelvic organs (called pelvic exenteration). These organs include the reproductive organs (vagina, uterus, fallopian tubes, and ovaries), bladder, urethra, rectum, and anus. Which organs are removed and whether all are removed depends on many factors, such as the cancer's location, the woman's anatomy, and her goals after surgery. Permanent openings—for urine (urostomy) and for stool (colostomy)—are made in the abdomen so that these waste products can leave the body and be collected in bags.
Sentinel lymph node mapping and dissection
A sentinel lymph node is the first lymph node that cancer cells are likely to spread to. There may be more than one sentinel lymph node. These nodes are called sentinel lymph nodes because they are the first to warn that cancer has spread.
A sentinel lymph node dissection involves
Identifying the sentinel lymph node (called mapping)
Removing it
Examining it to determine whether cancer cells are present
To identify sentinel lymph nodes, doctors inject a blue or green dye and/or a radioactive substance into the cervix near the tumor. These substances map the pathway from the cervix to the first lymph node (or nodes) in the pelvis. During surgery, doctors then check for lymph nodes that look blue or green or that give off a radioactive signal (detected by a handheld device). Doctors remove this node (or nodes) and send it to a laboratory to be checked for cancer. If the sentinel lymph node or nodes do not contain cancer cells, no other lymph nodes are removed (unless they look abnormal).
For women with early-stage cervical cancer, sentinel lymph node dissection is an alternative to removing lymph nodes in the pelvis. Cervical cancer spreads to the lymph nodes in only 15 to 20% of women with early-stage cancer. Sentinel lymph node dissection may help doctors limit the number of lymph nodes that need to be removed, sometimes to only one. Removing lymph nodes often causes problems such as accumulation of fluids in tissues, which can cause persistent swelling (lymphedema), and nerve damage.
Fertility and menopause after cervical cancer
Treatment with radical hysterectomy, chemotherapy, and/or radiation therapy usually makes it impossible for women to become pregnant or to carry a pregnancy to term. However, if being able to have children is important, a woman should talk to her doctor and get as much information as possible about how treatment affects fertility and whether they are eligible for treatments that do not make future pregnancy impossible.
A cone biopsy (conization) may be an option for women who have low-risk, early-stage cervical cancer and who wish to preserve their ability to have children. Before this procedure, doctors check to see whether the cancer has spread to lymph nodes in the pelvis. If the cancer has not spread, doctors may completely remove the cancer by removing part of the cervix during a cone biopsy.
If women with early-stage cervical cancer wish to preserve their ability to have children, a different cancer treatment called radical trachelectomy (a fertility-preserving treatment) may be possible. Doctors remove the cervix, the tissue next to the cervix, the upper part of the vagina, and the lymph nodes in the pelvis. To remove these tissues, doctors may do one of the following:
Do open surgery
Use a laparoscope inserted through a small incision just below the navel, then thread instruments through the laparoscope, sometimes with robotic assistance (laparoscopic surgery)
Remove the tissues through the vagina (vaginal surgery)
Then the uterus is re-attached to the lower part of vagina. Thus, women still can become pregnant. However, babies must be delivered by cesarean.
Trachelectomy appears to be as effective as radical hysterectomy for many women with early-stage cervical cancer.
If premenopausal women are having radiation therapy, doctors discuss options for protecting the ovaries to avoid causing premature menopause. Before radiation therapy of the pelvis, ovaries may be moved outside the radiation field (oophoropexy) to avoid exposing them to radiation.
Prognosis for Cervical Cancer
Prognosis depends on the stage of the cervical cancer. The percentages of women who are alive 5 years after diagnosis and treatment are
Stage I: 80 to 90% of women
Stage II: 60 to 75%
Stage III: 30 to 40%
Stage IV: 15% or fewer
If the cancer is recurs, it usually does so within 2 years.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
National Cancer Institute: Cervical Cancer: This web site provides links to general information about cervical cancer, as well as links to information about causes, prevention, screening, treatment, and research and about coping with cancer.





