




Acute otitis media is a bacterial or viral infection of the middle ear, usually accompanying an upper respiratory infection. Symptoms include otalgia, often with systemic symptoms (eg, fever, nausea, vomiting, diarrhea), especially in the very young. Diagnosis is based on otoscopy. Treatment is with analgesics and sometimes antibiotics.
Although acute otitis media can occur at any age, it is most common between ages 3 months and 3 years. At this age, the eustachian tube is structurally and functionally immature—the angle of the eustachian tube is more horizontal, and the angle of the tensor veli palatini muscle and the cartilaginous eustachian tube makes the opening mechanism less efficient.
The etiology of acute otitis media may be viral or bacterial. Viral infections are often complicated by secondary bacterial infection. In neonates, gram-negative enteric bacilli, particularly Escherichia coli, and Staphylococcus aureus cause acute otitis media. In older infants and children < 14 years, the most common organisms are Streptococcus pneumoniae, Moraxella (Branhamella) catarrhalis, and nontypeable Haemophilus influenzae; less common causes are group A beta-hemolytic streptococci and S. aureus. In patients > 14 years, S. pneumoniae, group A beta-hemolytic streptococci, and S. aureus are most common, followed by H. influenzae.
Risk factors
The presence of smoking in the household is a significant risk factor for acute otitis media. Other risk factors include having a strong family history of otitis media, living in a low-resource or high air-pollution region, being bottle fed (instead of breastfed), and attending a day care center.
Complications
Complications of acute otitis media are uncommon. In rare cases, bacterial middle ear infection spreads locally, resulting in acute mastoiditis, petrositis, or labyrinthitis. Intracranial spread is extremely rare; it usually causes meningitis. Brain abscess, subdural empyema, epidural abscess, lateral sinus thrombosis, or otitic hydrocephalus may occur. Even with antibiotic treatment, intracranial complications are slow to resolve, especially in immunocompromised patients.
Symptoms and Signs of Acute Otitis Media
The usual initial symptom is an earache, often with hearing loss. Infants may simply be cranky or have difficulty sleeping. Fever, nausea, vomiting, and diarrhea often occur in young children. Otoscopic examination can show a bulging, erythematous tympanic membrane with indistinct landmarks and displacement of the light reflex. Air insufflation (pneumatic otoscopy) shows poor mobility of the tympanic membrane. Spontaneous perforation of the tympanic membrane causes serosanguineous or purulent otorrhea, typically rapidly, relieving the pain.

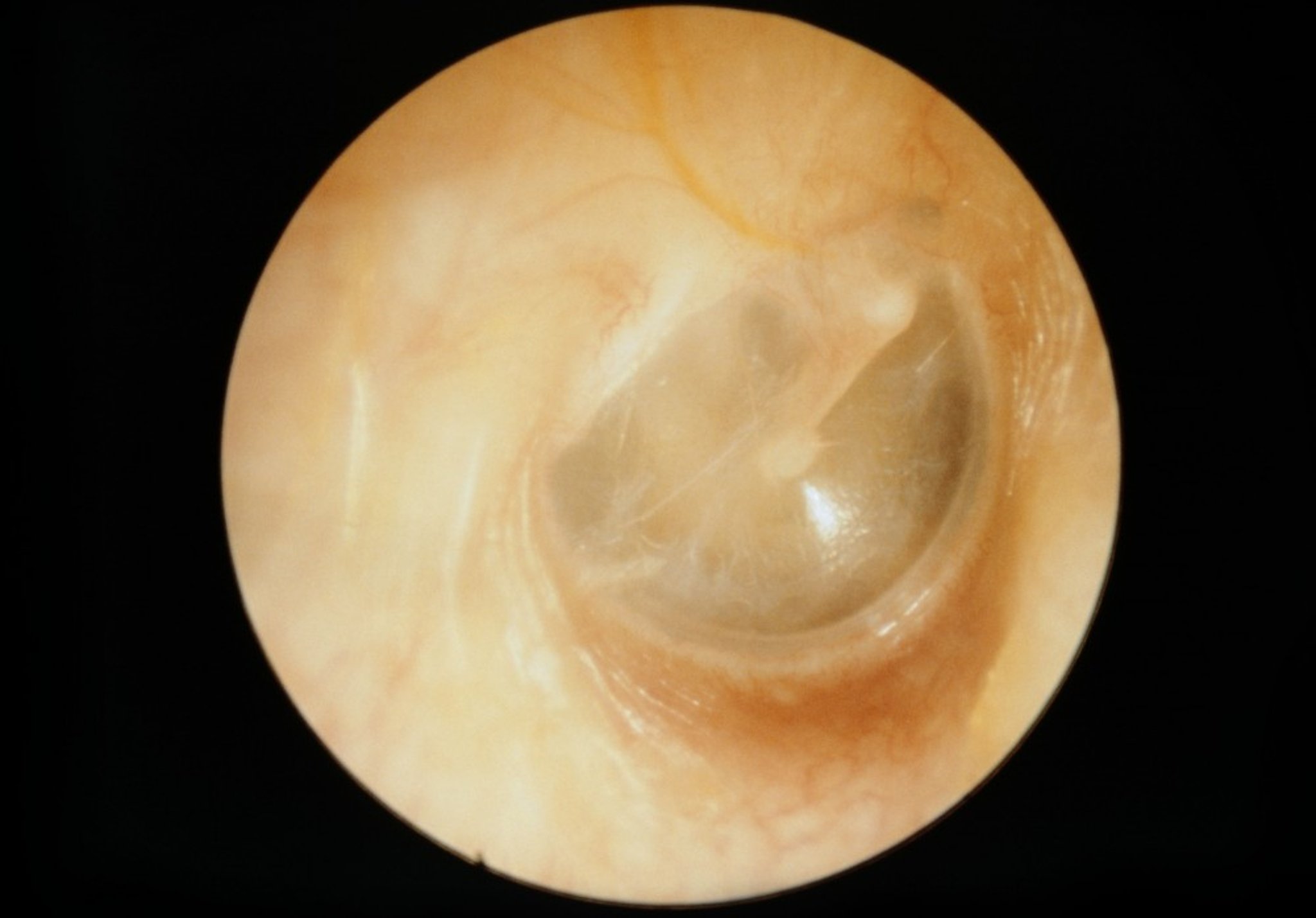
CLINICA CLAROS/SCIENCE PHOTO LIBRARY

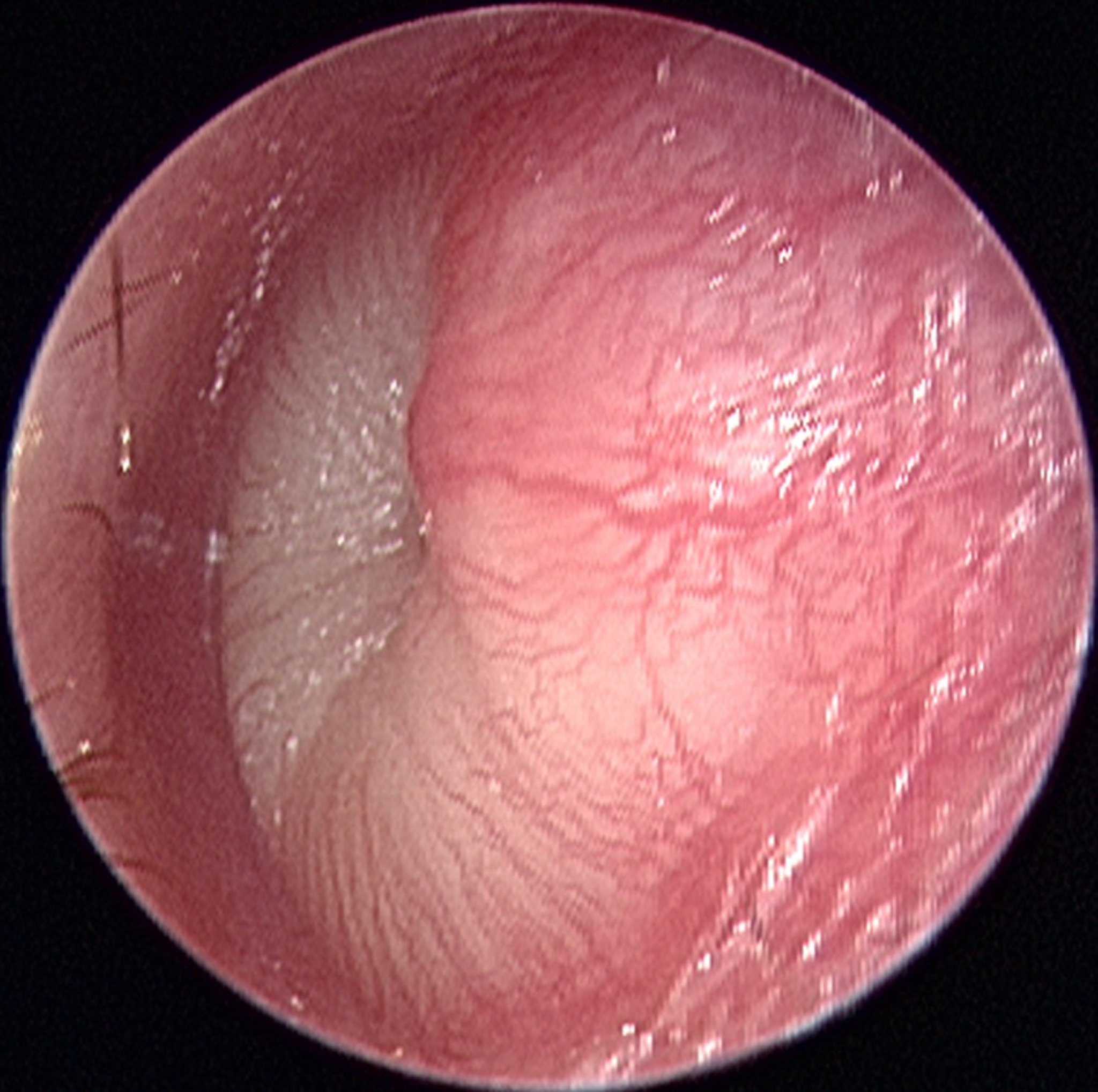
© Springer Science+Business Media
Severe headache, confusion, or focal neurologic signs may occur with intracranial spread of infection. Facial paralysis or vertigo suggests local extension to the fallopian canal or labyrinth.
Diagnosis of Acute Otitis Media
Clinical evaluation
Diagnosis of acute otitis media usually is clinical, based on the presence of acute (within 48 hours) onset of pain, bulging of the tympanic membrane and, particularly in children, signs of middle ear effusion detected by pneumatic otoscopy. Unless fluid is obtained during myringotomy, cultures are usually not done.
Treatment of Acute Otitis Media
Analgesics
Sometimes antibiotics
Rarely myringotomy
Most (80%) cases resolve spontaneously; however, in the United States, antibiotics are often given ([1]; see table Antibiotics for Otitis Media). Antibiotics relieve symptoms more quickly (although results after 1 to 2 weeks are similar) and may reduce the chance of residual hearing loss and labyrinthine or intracranial sequelae. However, with the recent emergence of resistant organisms, pediatric organizations have strongly recommended initial antibiotics only for certain children, such as the following:
Those who are younger or more severely ill—see table Guidelines for Using Antibiotics in Children With Acute Otitis Media)
Those with recurrent acute otitis media (eg, ≥ 4 episodes in 6 months)
Others, provided there is good follow-up, can safely be observed for 48 to 72 hours and given antibiotics only if no improvement is seen; if follow-up by phone is planned, a prescription can be given at the initial visit to save time and expense. Decision to observe should be discussed with the caregiver.
>
For children, neither vasoconstrictors nor antihistamines are of benefit.
Myringotomy may be done by a specialist for a bulging tympanic membrane, particularly if severe or persistent pain, fever, vomiting, or diarrhea is present. Tympanometry is used to monitor tympanic membrane movement; the patient's hearing and tympanic membrane appearance and movement are monitored until normal. If facial nerve palsy or weakness occurs in patients with acute otitis media, patients must be urgently referred to a specialist for possible myringotomy and placement of a tympanostomy tube.
Treatment reference
1. Lieberthal AS, Carroll AE, Chonmaitree T, et al: The diagnosis and management of acute otitis media. Pediatrics e964–99, 2013.
Prevention of Acute Otitis Media
Routine childhood vaccination against pneumococci (with pneumococcal conjugate vaccine), H. influenzae type B, and influenza decreases the incidence of acute otitis media. Infants should not sleep with a bottle, and elimination of household smoking may decrease incidence. Prophylactic antibiotics are not recommended for children who have recurrent episodes of acute otitis media.
Recurrent acute otitis media and recurrent serous otitis media may be prevented by the insertion of tympanostomy tubes.
Key Points
Give analgesics to all patients.
Use antibiotics selectively, based on patient age, severity of illness, and availability of follow-up.
Antihistamines and decongestants are not recommended for children; oral or nasal decongestants may help adults, but antihistamines are reserved for adults with an allergic etiology.






