




Epiglottitis is a rapidly progressive bacterial infection of the epiglottis and surrounding tissues that may lead to sudden respiratory obstruction and death. Symptoms include severe sore throat, dysphagia, high fever, drooling, and inspiratory stridor. Diagnosis requires direct visualization of the supraglottic structures; this procedure is not to be done until full respiratory support is available. Treatment includes airway protection and antibiotics.
Epiglottitis used to primarily affect children and usually was caused by Haemophilus influenzae type B. Now, because of widespread vaccination, it has been almost eradicated in children (more cases occur in adults). Causal organisms in children and adults include Streptococcus pneumoniae, Staphylococcus aureus, nontypeable H. influenzae, Haemophilus parainfluenzae, beta-hemolytic streptococci, Branhamella catarrhalis, and Klebsiella pneumoniae. H. influenzae type B is still a cause in adults and unvaccinated children.
Bacteria that have colonized the nasopharynx spread locally to cause supraglottic cellulitis with marked inflammation of the epiglottis, vallecula, aryepiglottic folds, arytenoids, and laryngeal ventricles. With H. influenzae type B, infection may spread hematogenously.
The inflamed supraglottic structures mechanically obstruct the airway, increasing the work of breathing, ultimately causing respiratory failure. Clearance of inflammatory secretions is also impaired.
Symptoms and Signs of Epiglottitis
In children with epiglottitis, sore throat, odynophagia, and dysphagia develop abruptly, often with no visible oropharyngeal inflammation. Fatal asphyxia may occur within a few hours of onset. Drooling is very common. Additionally, the child typically has signs of toxicity (poor or absent eye contact, cyanosis, irritability, inability to be consoled or distracted) and is febrile and anxious. Dyspnea, tachypnea, and inspiratory stridor may be present, often causing the child to sit upright, lean forward, and hyperextend the neck with the jaw thrust forward and mouth open in an effort to enhance air exchange (tripod position). Relinquishing this position may herald respiratory failure. Suprasternal, supraclavicular, and subcostal inspiratory retractions may be present.
In adults, symptoms are similar to those of children, including sore throat, fever, dysphagia, and drooling, but peak symptoms usually take > 24 hours to develop. Because of the larger diameter of the adult airway, obstruction is less common and less fulminant.
In many children and adults, oropharyngeal inflammation is not visible. However, severe throat pain with a normal-appearing pharynx raises suspicion of epiglottitis. A delay in diagnosis and treatment increases the risk of airway obstruction and death.
Diagnosis of Epiglottitis
Direct inspection (typically in operating room)
X-rays in milder cases with low suspicion
Epiglottitis is suspected in patients with severe sore throat and no pharyngitis and in patients with sore throat and inspiratory stridor. Stridor in children may also result from croup (viral laryngotracheal bronchitis—see table Differentiating Epiglottitis From Croup), bacterial tracheitis, and airway foreign body. The tripod position may also occur with peritonsillar abscess or retropharyngeal abscess.
The patient is hospitalized if epiglottitis is suspected. Diagnosis requires direct examination, usually with flexible fiberoptic laryngoscopy. (CAUTION: Examination of the pharynx and larynx may precipitate complete respiratory obstruction in children; only specifically trained personnel should directly examine the pharynx and larynx, and the examination should be done in an operating room, where the most advanced airway intervention is available.) Direct laryngoscopy that reveals a beefy-red, stiff, edematous epiglottis is diagnostic.
Although plain x-rays may be helpful, they are not highly accurate (1) and must be taken during inspiration, during neck extension, and with no rotation to avoid false-positive results. Also, a child with stridor should not be transported to the x-ray suite.
Cultures from the supraglottic tissues and blood can then be taken to search for the causative organism.
In some adult patients with epiglottis, flexible fiberoptic laryngoscopy can be done safely. However, flexible laryngoscopy is sometimes not done in adult patients,because it may cause airway collapse.

Image provided by Clarence T. Sasaki, MD.
Image provided by Clarence T. Sasaki, MD.
Image provided by Clarence T. Sasaki, MD.

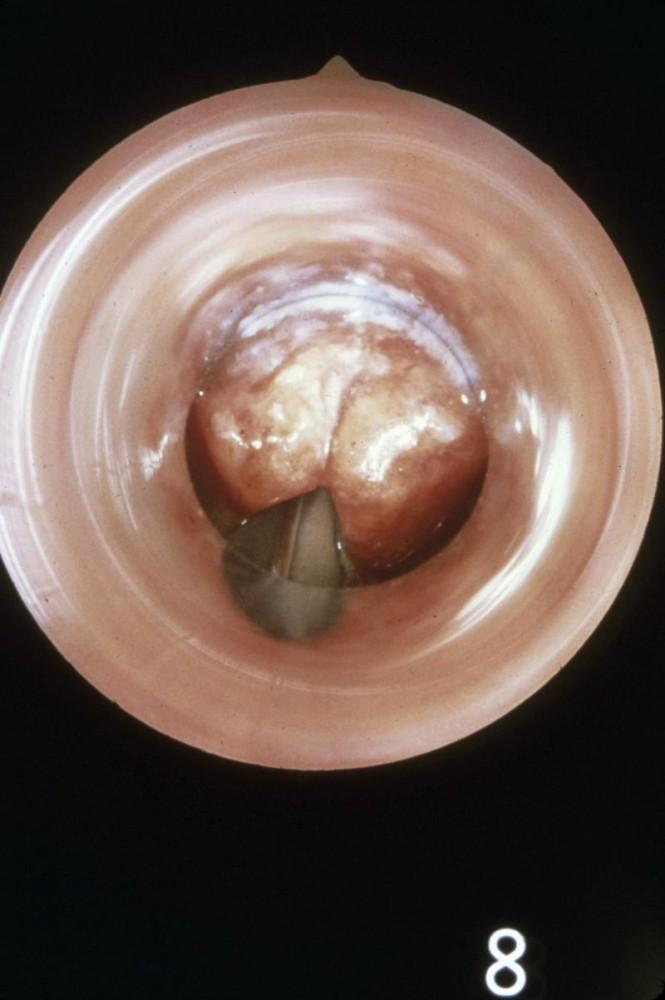
Image provided by Clarence T. Sasaki, MD.

Image provided by Clarence T. Sasaki, MD.

Image provided by Clarence T. Sasaki, MD.
Pearls & Pitfalls
|
Diagnosis reference
1. Fujiwara T, Miyata T, Tokumasu H, et al: Diagnostic accuracy of radiographs for detecting supraglottitis: A systematic review and meta-analysis. Acute Med Surg 4 (2):190–197, 2016. doi: 10.1002/ams2.256 eCollection 2017 Apr.
Treatment of Epiglottitis
Airway establishment
In children with stridor, any intervention that could be upsetting and thus could trigger airway obstruction should be avoided until an airway is established. In children with epiglottitis, the airway must be secured immediately. Securing the airway can be quite difficult and should, if possible, be done by experienced personnel in the operating room. An endotracheal tube is usually required until the patient has been stabilized for 24 to 48 hours (usual total intubation time is < 60 hours for both children and adults). Alternatively, a tracheotomy is done. If respiratory arrest occurs before an airway is established, bag-mask ventilation may be a life-saving temporary measure. For emergency care of children with epiglottitis, each institution should have a protocol that involves critical care, otolaryngology, anesthesia, and pediatrics.
Adults whose airway is severely obstructed can be endotracheally intubated during flexible fiberoptic laryngoscopy. Other adults may not require immediate intubation but should be observed for airway compromise in an intensive care unit with an intubation set and cricothyrotomy or tracheostomy tray at the bedside.
Epiglottitis caused by H. influenzae type B can be effectively prevented with the H. influenzae type B (HiB) conjugate vaccine.
Key Points
The incidence of epiglottitis has decreased significantly, particularly in children, because of widespread vaccination against the most common cause, Haemophilus influenzae type B.
Stridor, as well as sore throat with a normal-appearing pharynx, should raise suspicion of epiglottitis.
In children with stridor and suspected epiglottitis, examination of the pharynx or larynx may precipitate complete airway obstruction; only specifically trained personnel should directly examine the pharynx and larynx, and the examination should be done in an operating room.
If the diagnosis is suspected, do flexible fiberoptic laryngoscopy in the operating room; reserve imaging tests for cases with very low suspicion.
Children typically should have their airway secured by tracheal intubation; if airway obstruction is not severe, adults can often be observed for signs of airway compromise in an intensive care unit.






