





Except in emergencies (eg, cardiac tamponade), pericardiocentesis, a potentially lethal procedure, should be done using echocardiographic guidance in a cardiac catheterization laboratory and should be supervised by a cardiologist or thoracic surgeon if possible. Resuscitation equipment must be at hand. IV sedation (eg, morphine 0.1 mg/kg or fentanyl 25 to 50 μg plus midazolam 3 to 5 mg) is desirable. The patient should be recumbent, with the head elevated 30° from the horizontal.
Under aseptic conditions, the skin and subcutaneous tissues are infiltrated with lidocaine.
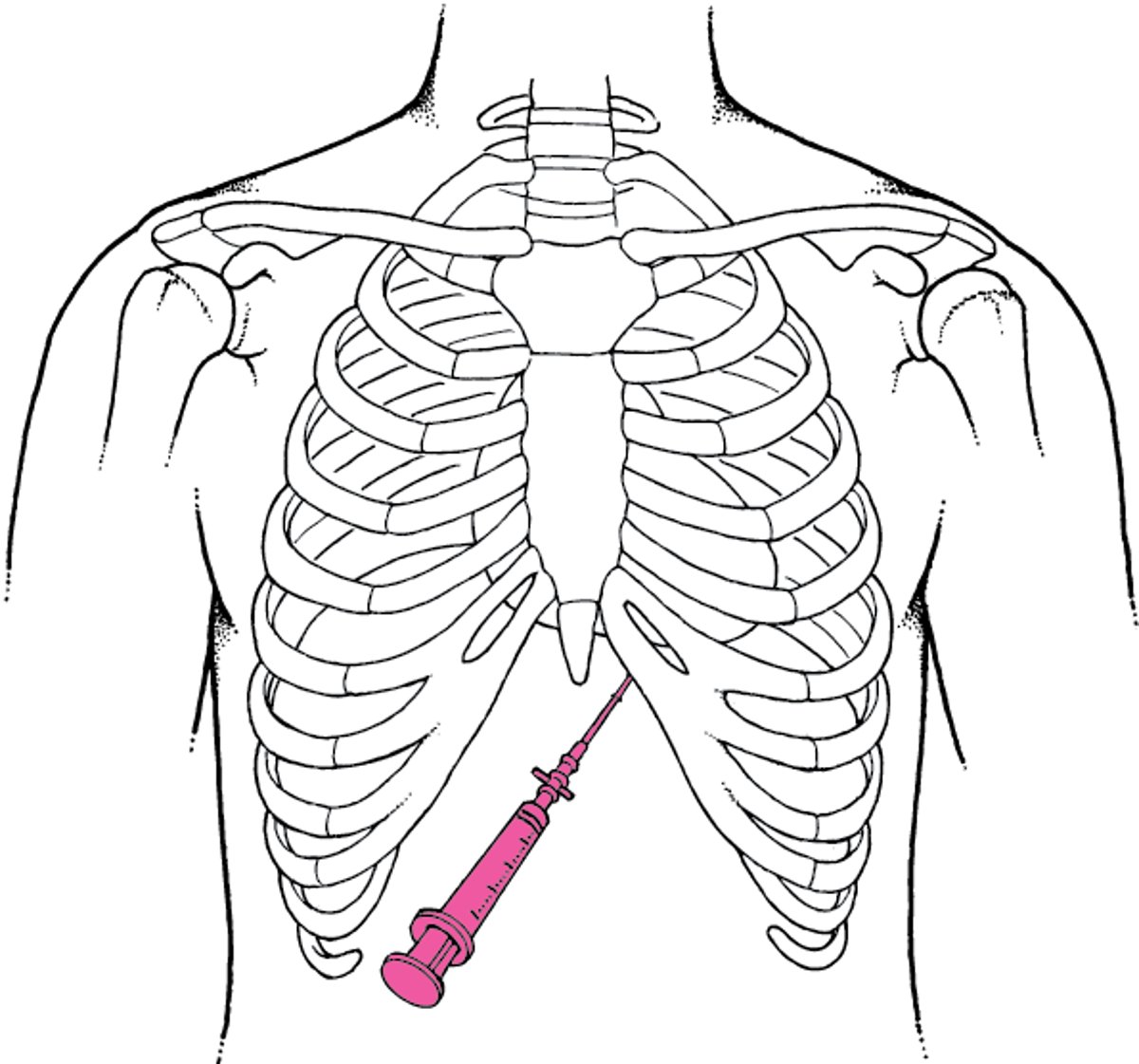
A 75-mm short-beveled, 16-gauge needle is attached via a 3-way stopcock to a 30- or 50-mL syringe. The pericardium may be entered via the right or left xiphocostal angle or from the tip of the xiphoid process with the needle directed inward, upward, and close to the chest wall. The needle is advanced with constant suction applied to the syringe.
Echocardiography may be used to guide the needle as agitated saline is injected through it. Echocardiography is also increasingly used to identify the optimal puncture site and the needle trajectory.
Once in place, the needle should be clamped next to the skin to prevent it from entering further than necessary and possibly puncturing the heart or injuring a coronary vessel. ECG monitoring is essential for detecting arrhythmias produced when the myocardium is touched or punctured. As a rule, right atrial pressure and pulmonary artery occlusion pressure (pulmonary capillary wedge pressure) are monitored.
Fluid is withdrawn until intrapericardial pressure falls below right atrial pressure, usually to subatmospheric levels. If continued drainage is needed, a plastic catheter may be passed through the needle into the pericardium and the needle withdrawn. The catheter may be left in place for 2 to 4 days.