


Achalasia is a disorder in which the rhythmic contractions of the esophagus (called peristalsis) are missing or impaired, the lower esophageal sphincter does not relax normally, and the resting pressure of the lower esophageal sphincter is increased.
This cause of this disorder usually is not known, but it may occur after exposure to some viruses.
The main symptoms of achalasia are trouble swallowing, spitting up of liquid and food, chest pain, and weight loss.
The diagnosis is based on results of manometry and barium swallow x-rays.
Treatment is aimed at relieving symptoms by dilating the lower esophageal sphincter with a balloon or cutting the muscle fibers of the sphincter, and sometimes by injecting botulinum toxin.
The esophagus is the hollow tube that leads from the throat (pharynx) to the stomach. (See also Overview of the Esophagus.) The lower esophageal sphincter is the ring of muscle that holds the bottom of the esophagus closed so that food and stomach acid do not flow back up the esophagus. When people swallow, this sphincter normally relaxes to allow food into the stomach.
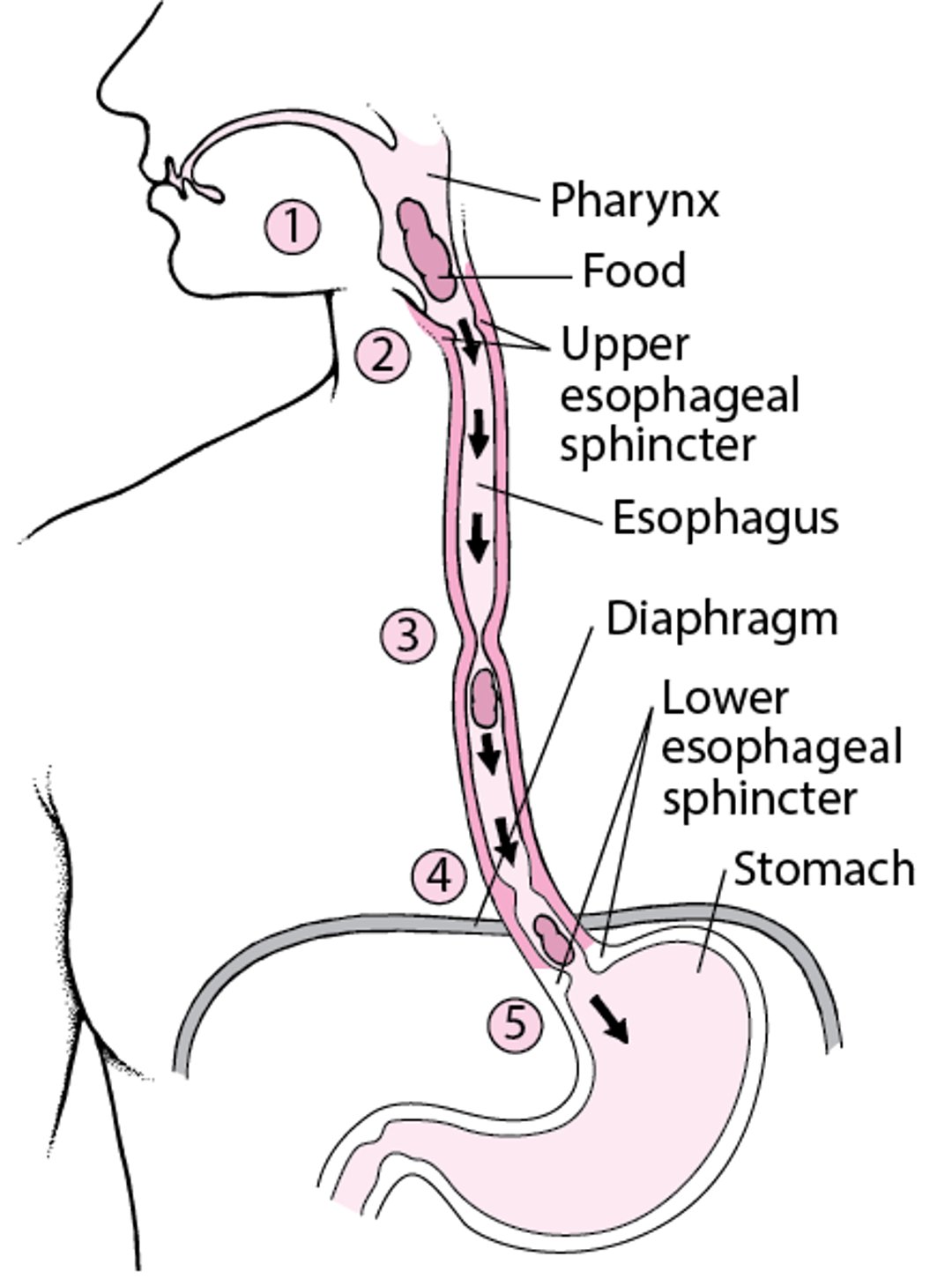
How the Esophagus Works
As a person swallows, food moves from the mouth to the throat, also called the pharynx (1). The upper esophageal sphincter opens (2) so that food can enter the esophagus, where waves of muscular contractions, called peristalsis, propel the food downward (3). The food then passes through the diaphragm (4) and lower esophageal sphincter (5) and moves into the stomach. |

Achalasia may occur at any age but usually begins, almost unnoticed, between the ages of 20 and 60 and then progresses gradually over many months or years.
Causes of Achalasia
Achalasia results from a malfunction of the nerves (called denervation) controlling the rhythmic contractions of the esophagus. The cause of the denervation is not usually known, but viral and autoimmune causes are suspected. Certain tumors may cause an achalasia–like disorder either by directly narrowing (constricting) the lower esophageal sphincter or by infiltrating the nerves of the esophagus. Chagas disease, an infection that causes the destruction of clusters of nerve cells (autonomic ganglia), may also result in achalasia.
Symptoms of Achalasia
The tight lower esophageal sphincter causes the part of the esophagus above it to enlarge greatly. This enlargement contributes to many of the symptoms. Difficulty swallowing (dysphagia) of both solids and liquids is the main symptom. Although less common, chest pain may occur during swallowing or for no apparent reason. About one third of people who have achalasia spit up (regurgitate) liquids and undigested food. If spitting up occurs when people are sleeping, they may inhale food into their lungs, which can cause coughing, infection of the airways, bronchiectasis, or aspiration pneumonia.
Mild to moderate weight loss also occurs. When people have significant weight loss, especially older adults whose symptoms of dysphagia developed rapidly, doctors consider and usually look for a tumor at the gastroesophageal junction (the place where the esophagus connects to the stomach).
Diagnosis of Achalasia
Manometry
Barium swallow x-rays
Doctors usually insert a small tube into the esophagus to take pressure measurements of the esophagus and lower esophageal sphincter (esophageal manometry). Often, doctors examine the esophagus through a flexible viewing tube (esophagoscopy). During an esophagoscopy, the doctor may do a biopsy (removal of tissue samples for examination under a microscope) to make sure the symptoms are not caused by cancer at the lower end of the esophagus.
X-rays of the esophagus taken while the person is swallowing barium (a barium swallow) show the normal rhythmic contractions of the esophagus are missing. The esophagus is widened, usually only moderately but occasionally to enormous proportions, but is narrow at the lower esophageal sphincter.
Impedance planimetry is a type of esophageal test. In this test, a balloon filled with salt water (saline solution) is used to measure the area across the inside of the esophagus (called the lumen) and the pressure inside of the esophagus at the same time. A functional lumen imaging probe (FLIP) is another esophageal test that uses impedance planimetry to evaluate how the esophagus functions. These measurements help doctors further evaluate people who are having trouble swallowing.
Some disorders, such as cancer at the gastroesophageal junction, can cause symptoms similar to achalasia (called pseudoachalasia), so doctors may do additional tests to rule them out. Cancer at the gastroesophageal junction can be diagnosed by esophagoscopy, computed tomography (CT) of the chest and abdomen, or by endoscopic ultrasonography (an ultrasound probe on the tip of an endoscope is passed through the mouth into the stomach).
Treatment of Achalasia
Balloon dilation
Myotomy
Sometimes botulinum toxin injections
No treatment restores peristalsis of the esophagus. The aim of treatment is to relieve symptoms by decreasing pressure in the lower esophageal sphincter.
There are two main treatment options for relieving the symptoms of achalasia that are equally effective and have similar outcomes.
Balloon dilation involves dilating the sphincter mechanically by inflating a large balloon inside it. This procedure is often successful, but repeated dilations may be needed. There is a small risk of the esophagus rupturing during the dilation procedure. Esophageal rupture leads to severe inflammation in the chest outside the esophagus (mediastinitis) and, in rare cases, is fatal if not treated appropriately. Immediate surgery is needed to close the rupture in the wall of the esophagus.
Myotomy involves surgery to cut the muscle fibers in the lower esophageal sphincter. The procedure is usually done with a laparoscope or, less commonly, with a thoracoscope. It can also be done with an endoscope inserted down the esophagus. Myotomy has a similar success rate as balloon dilation. As with balloon dilation, there is a small risk of the esophagus perforating during the myotomy procedure.
After myotomy, some people have an increased risk of developing a backflow of acid into the esophagus (gastroesophageal reflux disease). A procedure to prevent backflow of acid from the stomach (called a fundoplication) is usually done at the same time as myotomy.
Botulinum toxin can temporarily paralyze muscles, thus doctors sometimes inject botulinum toxin into the lower esophageal sphincter to relax it. This injection is an alternative to balloon dilation or myotomy and is almost as effective. However, the results typically last for only 6 months to 1 year, which is shorter than other treatments last.
Certain medications, such as nitrates or calcium channel blockers, have been studied but have not proved to be effective.






