


An abscess is a pocket of pus, usually caused by a bacterial infection.
Most people have constant abdominal pain and a fever.
Computed tomography or another imaging test can distinguish an abscess from other problems.
Treatment involves draining pus from the abscess and taking antibiotics.
(See also Acute Abdominal Pain.)
Abdominal abscesses may form below the diaphragm, in the middle of the abdomen, in the pelvis, or behind the abdominal cavity. Abscesses also may form in or around any abdominal organ, such as the kidneys, spleen, pancreas, or liver, or in the prostate gland. Untreated abscesses can grow and damage nearby blood vessels and organs.
Sometimes, bacteria enter the bloodstream (sepsis) and spread to distant organs and tissues. Such spread can be fatal.
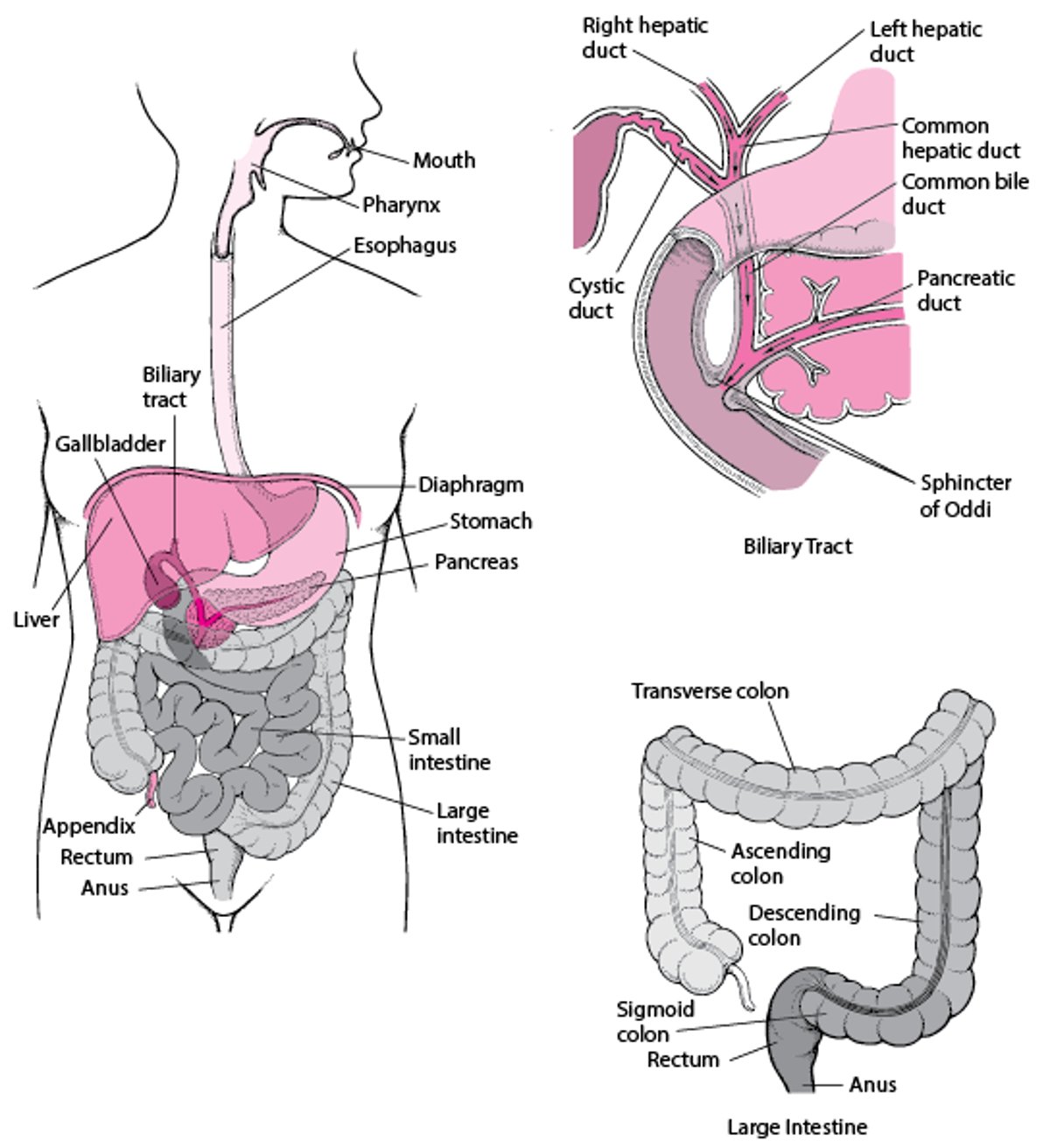
The Digestive System


Causes of Abdominal Abscesses
More common causes of abdominal abscesses involve spread of infection or inflammation caused by conditions such as appendicitis, diverticulitis, Crohn disease, pancreatitis, or pelvic inflammatory disease.
Sometimes, abdominal abscesses are caused by perforation of the intestine due to cancer, ulcer, or injury, and sometimes abscesses form after injury to the abdomen or after surgery on the abdomen.
Symptoms of Abdominal Abscesses
Specific symptoms of abdominal abscesses depend on the location of the abscess, but most people have constant discomfort or pain, feel generally sick (malaise), and often have a fever. Other symptoms include nausea, loss of appetite, and weight loss.
An abscess below the diaphragm may form when infected fluid, for example, from a ruptured appendix, is moved upward by the pressure of abdominal organs and by the suction created when the diaphragm moves during breathing. Symptoms may include a cough, painful breathing, chest pain, and pain in one shoulder. In this instance, the pain felt in one shoulder is an example of referred pain (pain felt in one area of the body that does not accurately represent where the problem is). Referred pain occurs because the shoulder and the diaphragm share the same nerves, and the brain incorrectly interprets the source of the pain (see figure What Is Referred Pain?).
Abscesses in the mid-abdomen may result from a ruptured appendix, a ruptured intestine, inflammatory bowel disease, diverticular disease, or an abdominal wound. The abdomen is usually painful in the area of the abscess.
An abscess in the lower abdomen may track down into the thigh or the area around the rectum (called the perirectal fossa).
Pelvic abscesses can result from the same disorders that cause abscesses in the mid-abdomen or from gynecologic infections. Symptoms may include abdominal pain, diarrhea caused by intestinal irritation, and an urgent or frequent need to urinate caused by bladder irritation.
Abscesses behind the abdominal cavity (called retroperitoneal abscesses) lie behind the peritoneum, the membrane that lines the abdominal cavity and organs. The causes, which are similar to those of abscesses in the abdomen, include inflammation and infection of the appendix (appendicitis), the pancreas (pancreatitis), and the kidneys (the kidneys are located behind the abdominal cavity). Pain, usually in the lower back, worsens when the person moves the leg at the hip.
Abscesses of the pancreas, although rare, typically form after an attack of acute pancreatitis. Symptoms such as fever, abdominal pain, nausea, and vomiting often begin a week or more after a person recovers from pancreatitis.
Liver abscesses may be caused by bacteria or by amebas (single-celled, microscopic parasites). Bacteria can reach the liver from an infected gallbladder, a penetrating or blunt wound, an infection in the abdomen (such as a nearby abscess), or an infection carried by the bloodstream from elsewhere in the body. Amebas from an intestinal infection reach the liver through the blood vessels. Symptoms of liver abscesses include loss of appetite, nausea, and a fever. A person may or may not have abdominal pain.
Abscesses in the spleen are caused by an infection traveling through the bloodstream to the spleen, by an injury to the spleen, or by the spread of an infection from a nearby abscess, such as one below the diaphragm. Pain may occur in the left side of the abdomen, the back, or the left shoulder.
Diagnosis of Abdominal Abscesses
Imaging tests
Needle aspiration
Doctors can easily misdiagnose an abscess because the first symptoms it causes are usually vague and mild and may be mistaken for less serious problems that are more common.
If doctors suspect a person has an abscess, they usually do computed tomography (CT) of the abdomen and pelvis or sometimes ultrasound scanning (ultrasonography), x-rays of the abdomen and chest, or magnetic resonance imaging (MRI). These tests can help distinguish an abscess from other problems, as well as determine the source, size, and position of an abscess.
To make a definitive diagnosis and treat the abscess, doctors sometimes insert a needle through the skin to draw a sample of pus from the abscess (needle aspiration) and place a drain. To guide the placement of the needle, doctors use CT or ultrasound scanning. The sample of fluid is then examined in a laboratory to identify the infecting organism so that the most effective antibiotic can be selected.
Occasionally, radionuclide scanning is done to help identify abscesses. For scanning, a radionuclide is used to label a substance that accumulates in a specific part of the body. Different substances are used depending on which part of the body is to be evaluated.
Treatment of Abdominal Abscesses
Drainage of pus
Antibiotics
Almost all abdominal abscesses need to be drained of pus, either by surgery or by a needle and a small flexible tube (catheter). To guide the placement of the needle and catheter, a doctor uses CT or ultrasound scanning. Once the doctor is sure the needle and catheter have reached the abscess, the needle is taken out but the catheter is left in place. The pus drains out through the catheter, usually over several days to weeks.
Antibiotics are usually used in addition to drainage to prevent the infection from spreading and to help completely eliminate the infection. Laboratory analysis of the pus identifies the infecting organism so that the most effective antibiotic can be selected. It is uncommon for antibiotics to cure an abscess without drainage.
If the abscess cannot be reached safely by the needle and catheter, surgical drainage may be necessary. Once the abscess has been drained, the source of the infection is also surgically treated. For example, if the abscess is caused by a perforation (hole) in the colon, doctors usually remove that part of the colon.
Maintaining proper nutrition is important. If people are unable to eat because of the abscess or because of the cause of the abscess, they may receive nutrition through a tube (called enteral tube nutrition) or a vein (called parenteral nutrition).
Prognosis for Abdominal Abscesses
Abdominal abscesses can cause death in about 10 to 40% of people. What caused the abscess and a person's general medical condition affect the prognosis more than the specific nature and location of the abscess. People who develop sepsis have a worse prognosis.






