


Intravenous feeding is used when the digestive tract cannot adequately absorb nutrients, as occurs in severe malabsorption disorders. It is also used when the digestive tract must be temporarily kept free of food, as is needed during certain stages of ulcerative colitis.
Food given intravenously can provide part of a person's nutritional requirements (partial parenteral nutrition), supplementing the food eaten by mouth. Or it may provide all of a person's nutritional requirements (total parenteral nutrition).
Parenteral nutrition requires a large intravenous tube. The tube (called a central venous catheter) must be inserted into a large vein, such as the subclavian vein, which is located under the collarbone. Parenteral nutrition may be used at home or in the hospital.
Total parenteral nutrition may be required in people with the following:
A digestive tract that is not functioning
Severe pancreatitis or certain stages of ulcerative colitis
In children, diarrhea that has lasted a long time, regardless of its cause
Short bowel syndrome due to surgical removal of a large part of the small intestine
Compared with tube feeding, intravenous feeding causes more complications, does not preserve the structure and function of the digestive tract as well, and is more expensive. Intravenous feeding is usually not the first choice for nutritional support when the digestive tract is functioning.
Procedure for Intravenous Feeding
Because the central venous catheter must remain in place for a long time, infections are a risk. To reduce the risk, health care practitioners use strict sterile techniques when inserting and maintaining the catheter. For example, they do the following:
Clean the skin at the insertion point before inserting the catheter
Change the tubing connecting the catheter to the bag of formula every day
Change the dressings that hold the catheter in place every other day
Using the catheter only for intravenous feeding also helps reduce the risk of infection.
To place the catheter, doctors insert a needle through the skin into the vein, then thread a guide wire through the needle. The needle is removed, and the catheter is passed over the guide wire, which is then removed. A small ultrasound device may be used to guide the placement of the catheter, and an x-ray may be taken afterward to confirm that the placement is correct. Often, the catheter is placed in the subclavian vein, under the collarbone. The catheter may be inserted into a vein in the neck if it is to be used only during a hospital stay.
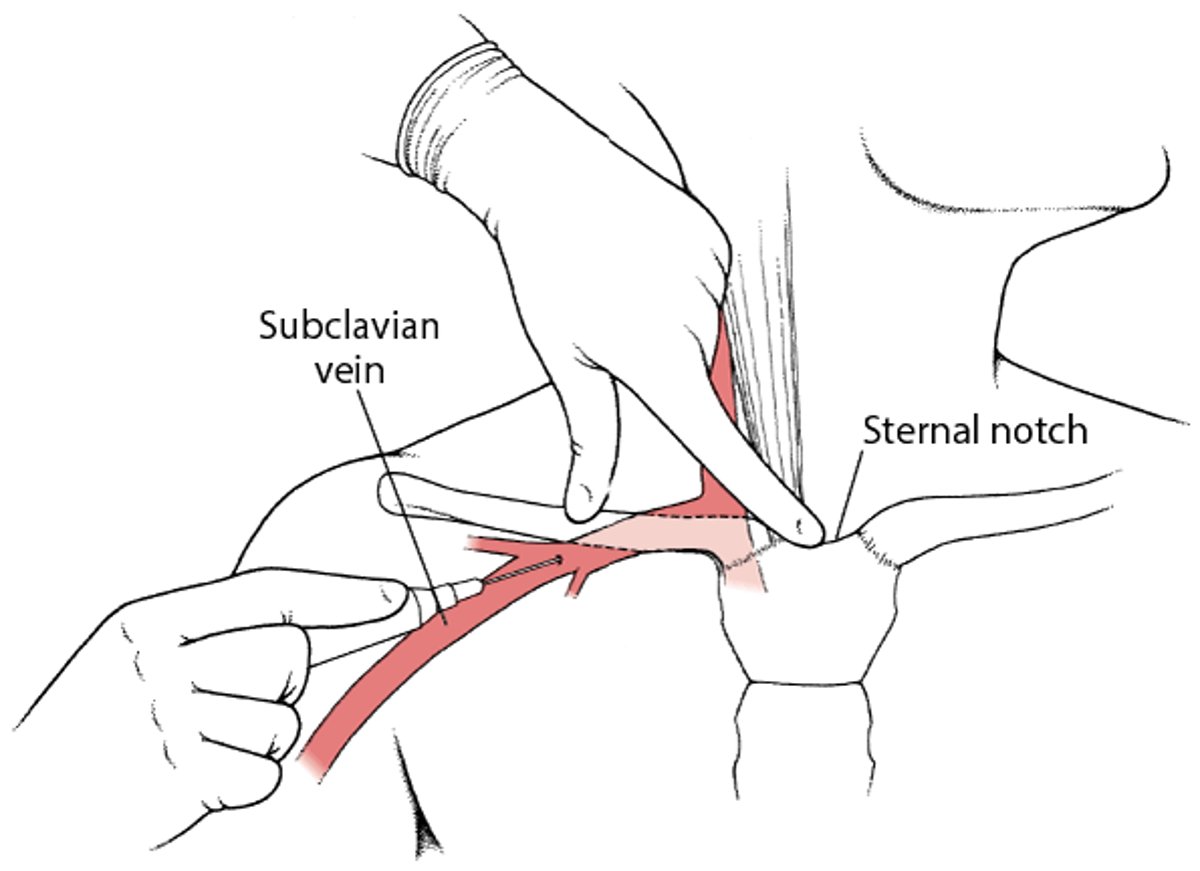
Catheter in a Chest Vein for Feeding
This figure shows the blood vessel (subclavian vein) in the chest that can be used for intravenous feeding. |

An interdisciplinary nutrition team (including a doctor, dietitian, pharmacist, and nurse), if available, should monitor the person's progress. They regularly measure body weight, the number of blood cells in blood (complete blood count), and levels of electrolytesliver tests) and keep track of how much fluid the person is getting and how much urine is excreted. A complete nutritional assessment, including calculating body mass index (BMI) and analyzing body composition, is done every 2 weeks.
If total parenteral nutrition is given outside the hospital, the person is taught to recognize the symptoms of infection, and home nurses visit regularly to check for problems.
Formulas
In the standard formula for intravenous feeding, carbohydrates provide most of the calories. Formulas may also contain water, protein, fats, vitamins, and minerals. Essential amino acids (components of protein) and essential fatty acids (components of fat) are also included. These nutrients are called essential because the body cannot make them from other nutrients. Thus, they must be consumed in the diet.
However, different formulas can be used based on test results, other disorders present, the person's age, and other factors, as for the following:
For people with kidney failure when dialysis is not being used or for people with liver failure: A formula with less protein but a high percentage of essential amino acids
For people with heart or kidney failure: A formula with less fluid
For people with respiratory failure: A formula with less carbohydrate and more fat, which is added to provide the needed amount of calories (processing fat is less work for the lungs than processing carbohydrates)
For newborns: A formula with less sugar
For obese people: A formula with less fat
Complications of Intravenous Feeding
Intravenous feeding can cause problems related to the central venous catheter or to the formula, as well as other problems. Why some problems occur is unknown.
Injury during insertion of the catheter may occur. For example, a blood vessel, nerve, or lung may be injured.
Infections are more likely when an incision is made in the skin, as is needed to insert a catheter, especially when it is left in place a long time. (Normally, the skin helps prevent organisms that cause infection from entering the body.) Infections may spread to the bloodstream, and bloodstream infections can lead to a serious condition called sepsis. Using sterile techniques can help prevent infections.
A blood clot sometimes forms in the vein that the catheter is in.
Nutritional imbalances and deficiencies can occur during intravenous feeding. Blood sugar (glucose) levels that are too high (hyperglycemia) or too low (hypoglycemia) are relatively common. Rarely, deficiencies of certain vitamins and minerals occur. To identify these problems, doctors do blood tests to measure levels of sugar and minerals (electrolytes). They adjust the formula as needed and periodically recheck sugar and electrolyte levels.
Too much water (volume overload) or too little water may be given. Too much water (overhydration) can cause fluid to collect in the lungs, making breathing difficult. Too little water results in dehydration
Problems due to formulas that contain more fat and fewer carbohydrates (called lipid emulsions) occasionally occur. These problems include difficulty breathing, allergic reactions, nausea, headache, back pain, sweating, and dizziness. Fat (lipid) levels in the blood may increase temporarily, especially in people with kidney or liver failure. Later, the liver and/or spleen may enlarge, and people may tend to bleed and bruise more easily or develop infections more often. Premature infants with respiratory distress syndrome or other lung disorders are particularly at risk of these problems. To try to prevent or minimize these problems, doctors may temporarily or permanently slow or stop the formula.
Liver problems
Bone density may decrease if intravenous feeding lasts more than 3 months. Osteoporosis or osteomalacia (due to a ) may result. If advanced, these disorders can cause severe pain in the joints, legs, and back.
Gallbladder problems may develop or worsen when the gallbladder is inactive, as may occur during intravenous feeding. Substances (such as cholesterol) that are normally processed and moved through the gallbladder may accumulate, forming gallstones or sludge. Stones may block a duct, causing inflammation (cholecystitis






