


Cardiac imaging tests can delineate cardiac structure and function. Standard imaging tests include
Various radionuclide techniques
Standard CT and MRI have limited application because the heart constantly beats, but faster CT and magnetic resonance techniques can provide useful cardiac images if the rhythm is regular and the heart rate is controlled; sometimes patients are given a drug (eg, a beta-blocker) to slow the heart rate during imaging.
In ECG gating, the image recording (or reconstruction) is synchronized with the electrocardiogram (ECG), providing information from several cardiac cycles that can be used to create single images of selected points in the cardiac cycle.
CT gating uses the ECG to trigger the x-ray beam at the desired portion of the cardiac cycle, exposing the patient to less radiation than gating that reconstructs information from only the desired portion of the cardiac cycle (gated reconstruction) and does not interrupt the x-ray beam.
Chest X-Rays in Cardiac Diagnosis
Chest x-rays are often useful as a starting point in a cardiac diagnosis and should always be done when a diagnosis of heart failure is considered. Posteroanterior and lateral views provide a gross view of atrial and ventricular size and shape and pulmonary vasculature, but additional tests are almost always required for precise characterization of cardiac structure and function.

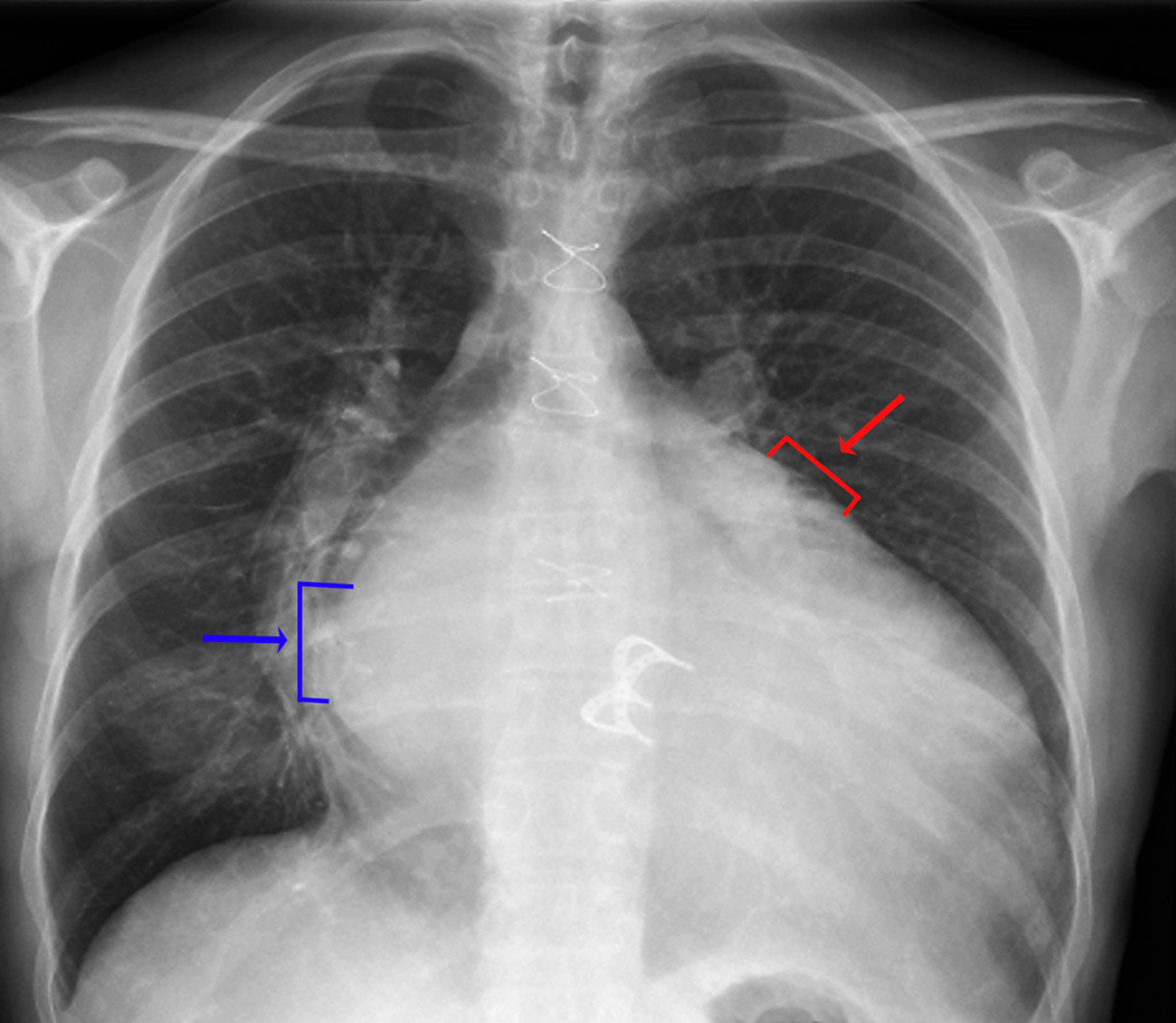
ZEPHYR/SCIENCE PHOTO LIBRARY
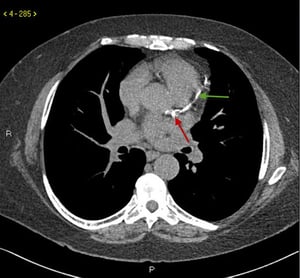
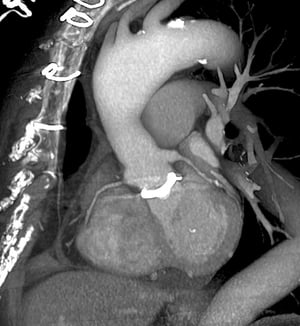
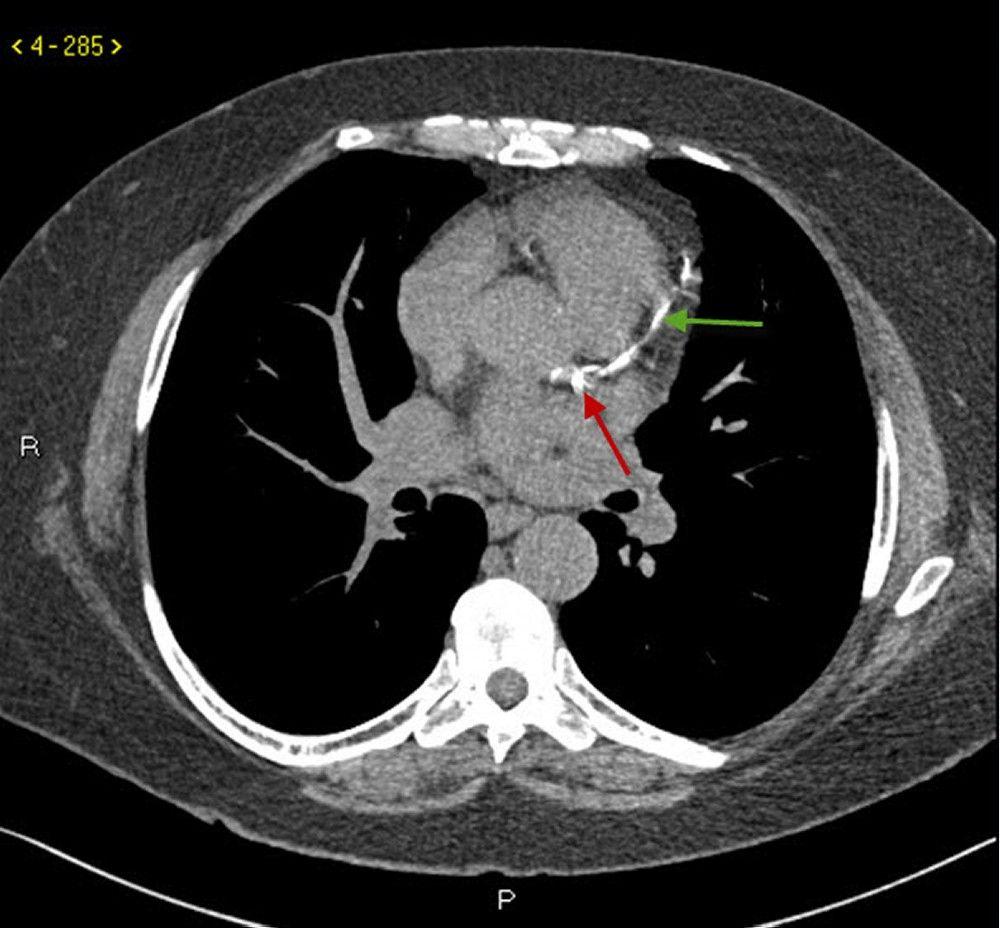
Computed Tomography (CT) in Cardiac Diagnosis
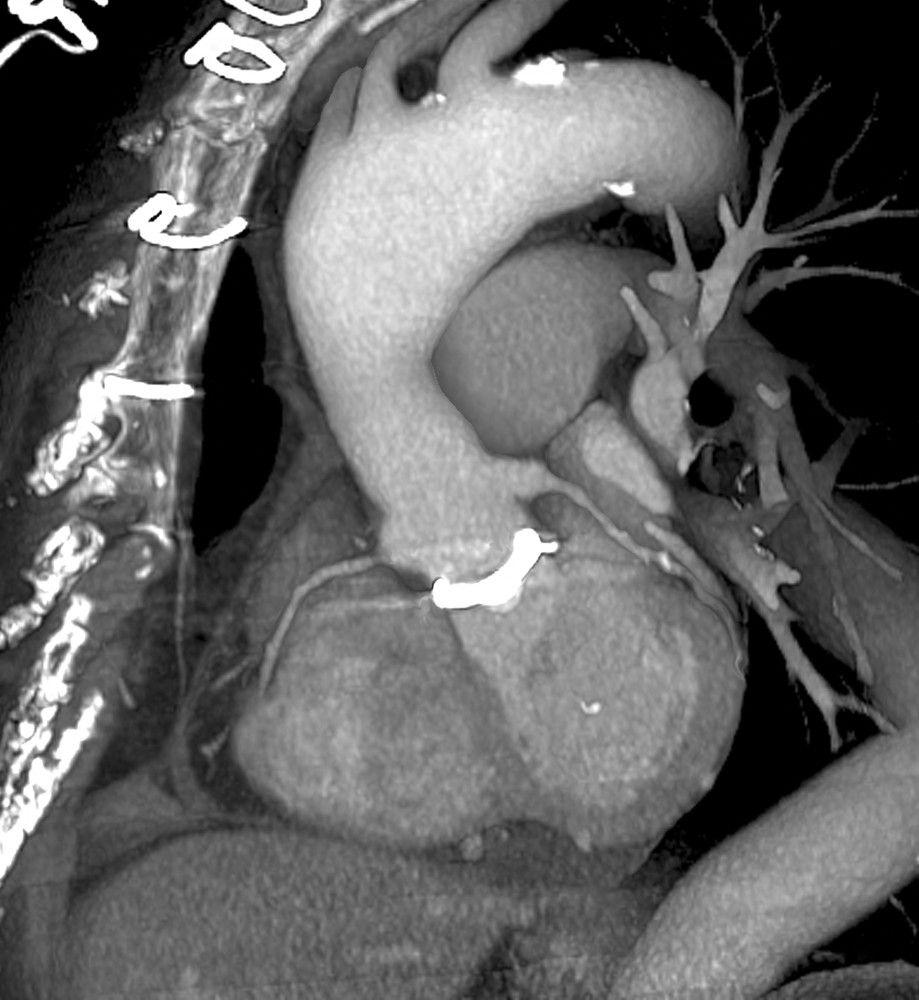
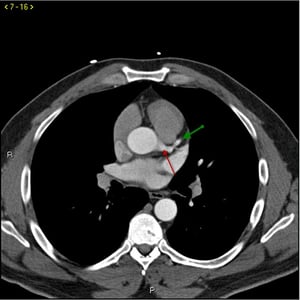
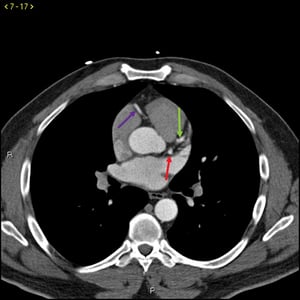
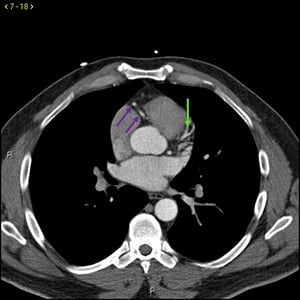
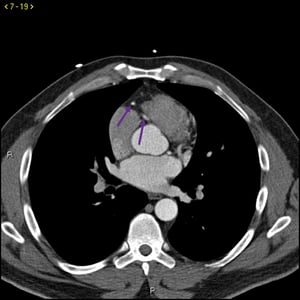
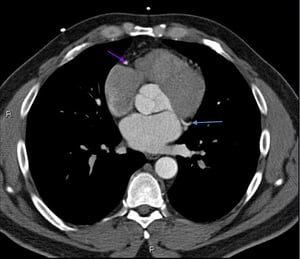
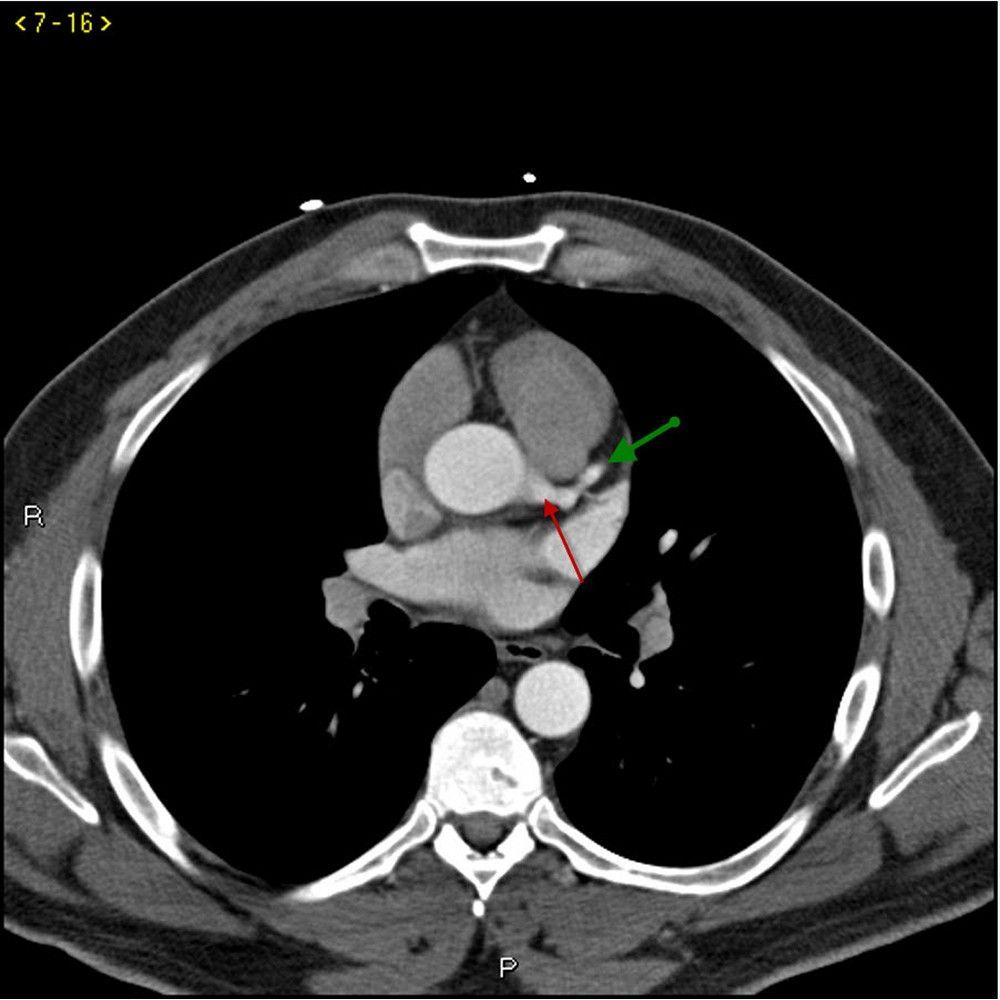
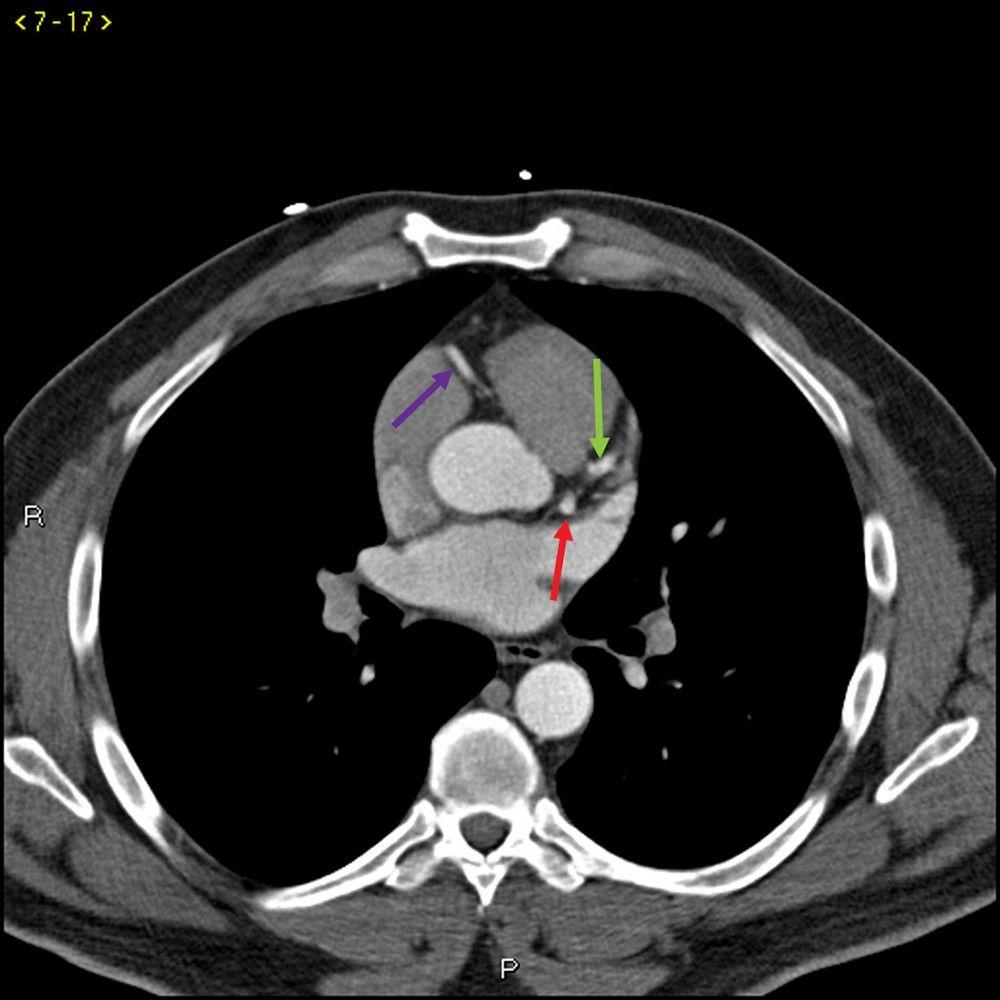
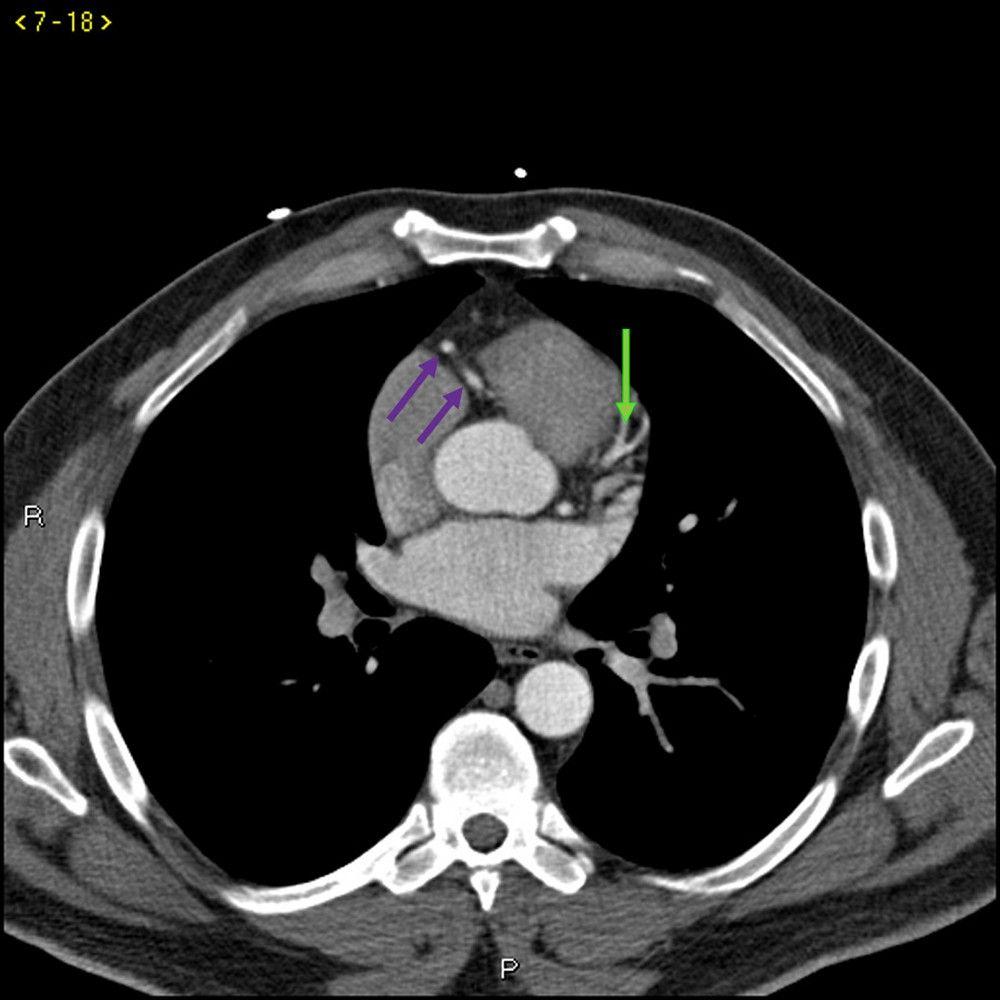
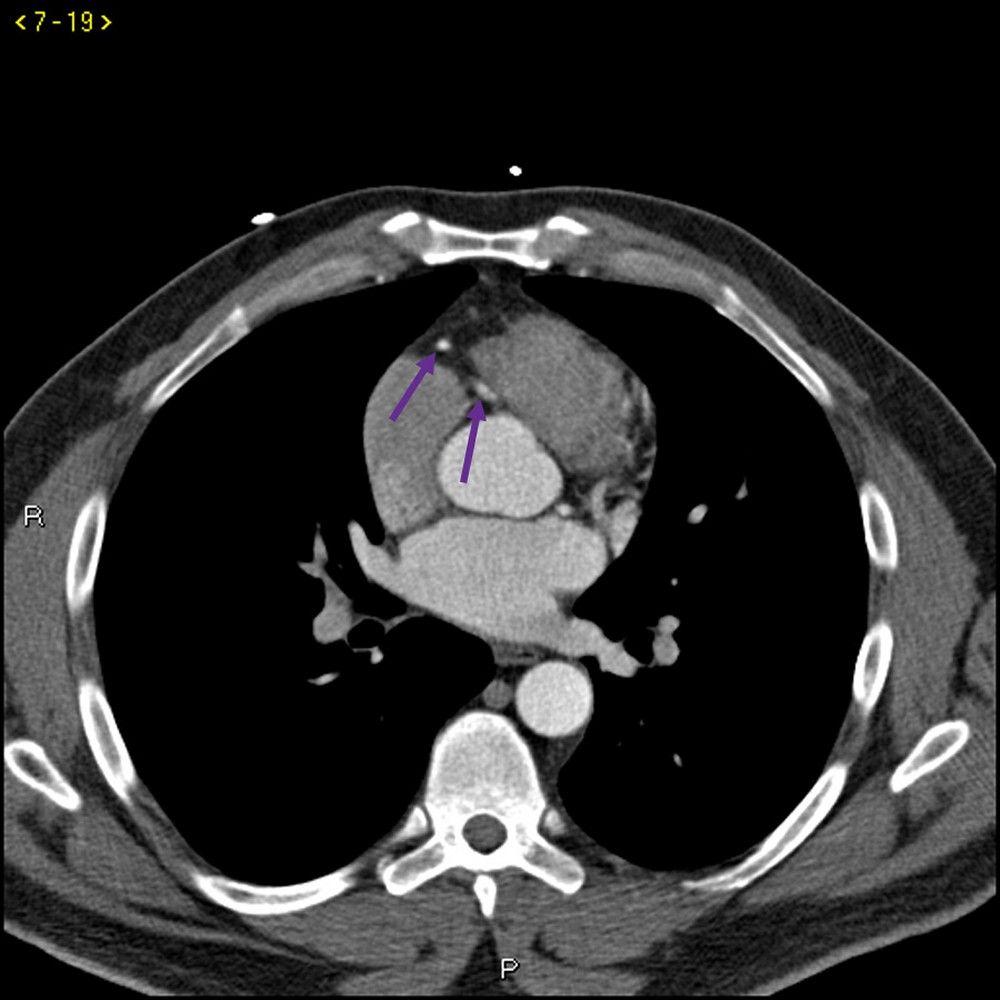
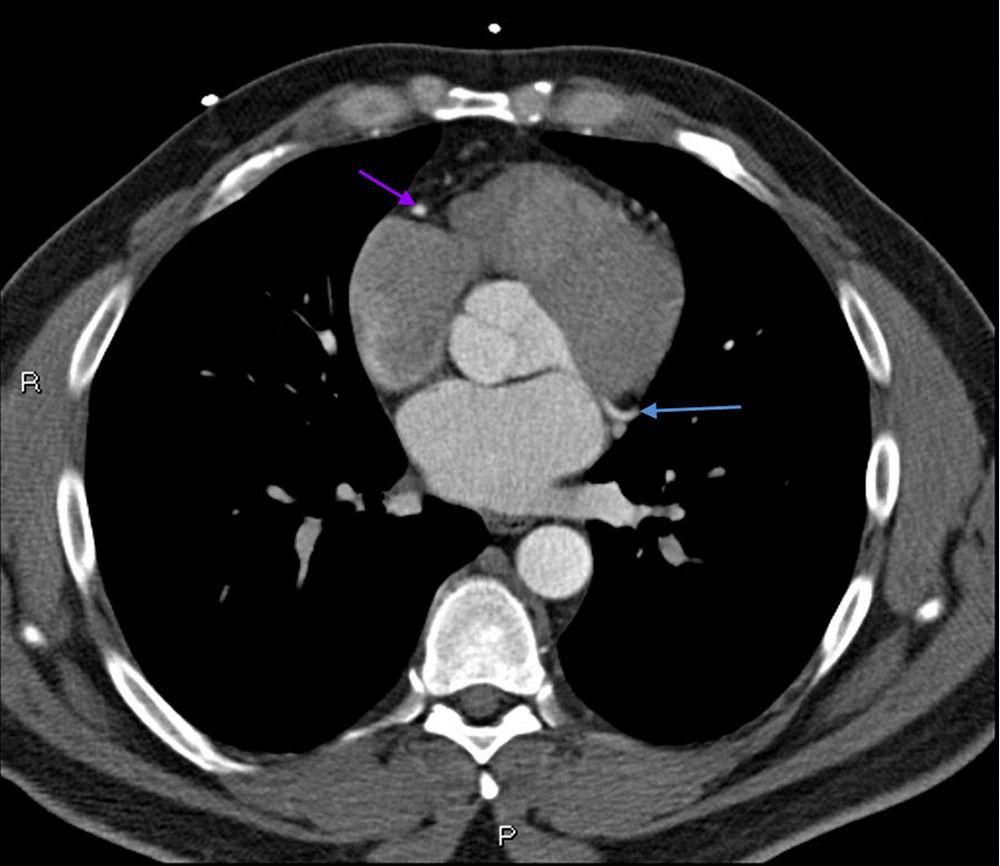
Spiral (helical) CT may be used to evaluate pericarditis, congenital cardiac disorders (especially abnormal arteriovenous connections), disorders of the great vessels (eg, aortic aneurysm, aortic dissection), cardiac tumors, acute pulmonary embolism, chronic pulmonary thromboembolic disease, and arrhythmogenic right ventricular dysplasia. Noncontrast CT can be used to look for coronary artery calcification; the calcium load is sometimes used to refine estimates of cardiac risk. The use of CT to evaluate most other cardiac conditions requires a radiopaque contrast agent, which may limit its use in patients with renal impairment.


LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY
© 2017 Elliot K. Fishman, MD.
ZEPHYR/SCIENCE PHOTO LIBRARY

© 2017 Elliot K. Fishman, MD.

ZEPHYR/SCIENCE PHOTO LIBRARY
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.

© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.

© 2017 Elliot K. Fishman, MD.

© 2017 Elliot K. Fishman, MD.
Electron beam CT, formerly called ultrafast CT or cine CT, unlike conventional CT, does not use a moving x-ray source and target. Instead, the direction of the x-ray beam is guided by a magnetic field and detected by an array of stationary detectors. Because mechanical motion is not required, images can be acquired in a fraction of a second (and recorded at a specific point in the cardiac cycle). Electron beam CT is used primarily to detect and quantify coronary artery calcification, an early sign of atherosclerosis. However, spatial resolution is poor and the equipment cannot be used for noncardiac disorders, so newer standard CT techniques are becoming preferred for cardiac use.
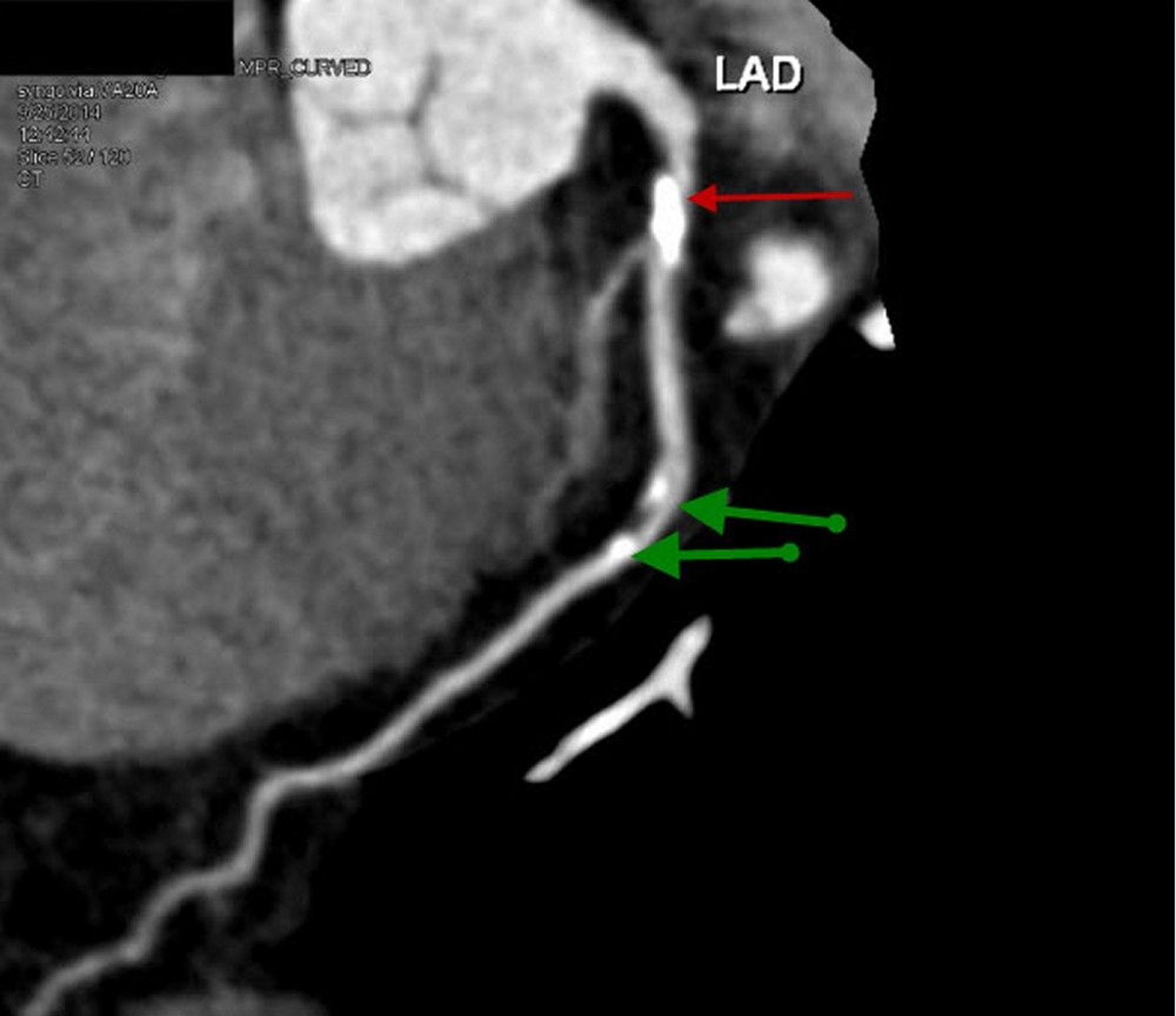
Multidetector CT (MDCT), with ≥ 64 detectors, has a very rapid scan time; some advanced machines may generate an image from a single heartbeat, although typical acquisition time is 30 seconds. Dual-source CT uses 2 x-ray sources and 2 multidetector arrays on a single gantry, which cuts scan time in half. Both of these modalities appear able to identify coronary calcifications and flow-limiting (ie, > 50% stenosis) coronary artery obstruction. Typically, an IV contrast agent is used, although nonenhanced scans can detect coronary artery calcification.
MDCT, a noninvasive alternative to coronary angiography, is used mainly for patients with stable angina to identify obstructive coronary artery disease or patients with chest pain and a low to intermediate probability of acute coronary syndrome. Although the radiation dose can be significant, about 15 mSv (vs 0.1 mSv for a chest x-ray and 7 mSv for coronary angiography), newer imaging protocols can reduce the exposure to 5 to 10 mSv. The presence of high-density calcified plaques creates imaging artifacts that interfere with interpretation. Nonenhanced scans to evaluate for coronary artery calcification can be done with even lower radiation exposure. The amount of coronary artery calcium present can be used to determine the 10-year risk of coronary artery disease (see The Multi-Ethnic Study of Atherosclerosis (MESA) risk calculator). The absence of coronary artery calcium portends a very favorable prognosis.
Magnetic Resonance Imaging (MRI) in Cardiac Diagnosis
Standard MRI is useful for evaluating areas around the heart, particularly the mediastinum and great vessels (eg, for studying aneurysms, dissections, congenital heart disease, and stenoses). With ECG-gated data acquisition, MRI can be used to image the heart itself, and image resolution can approach that of CT or echocardiography, clearly delineating myocardial wall thickness and motion, chamber volumes, intraluminal masses or clot, and valve planes.

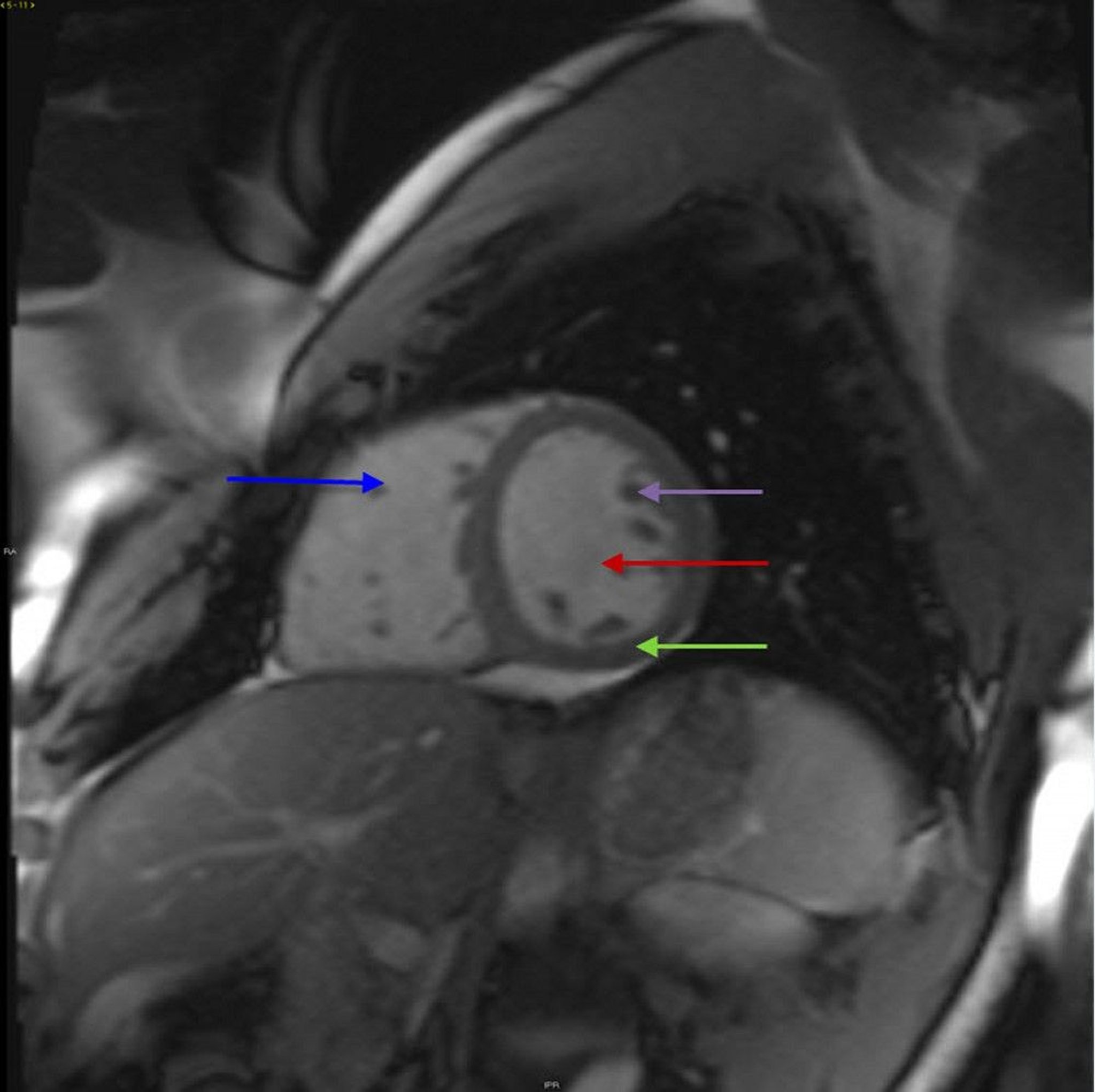
© 2017 Elliot K. Fishman, MD.
Sequential MRI after injecting a paramagnetic contrast agent (gadolinium-diethylenetriamine pentaacetic acid [Gd-DTPA]) produces higher resolution of myocardial perfusion patterns than does radionuclide imaging. MRI is generally considered the most accurate and reliable measure of ventricular volumes as well as ejection fraction. However, patients with impaired renal function can develop nephrogenic systemic fibrosis, a potentially life-threatening disorder, after use of gadolinium contrast. Contrast agents are being developed that are safe to use in patients with impaired renal function.
When MRI is done with contrast,Marfan syndrome, MRI measurements of ascending aorta dilation are more accurate than echocardiographic measurements. MRI is increasingly being used in the evaluation of nonischemic cardiomyopathies such as amyloidosis.
Magnetic resonance angiography (MRA), after injection of a gadolinium contrast agent, is used to assess blood volumes of interest (eg, blood vessels in the chest or abdomen); all blood flow can be assessed simultaneously. MRA can be used to detect aneurysms, stenosis, or occlusions in the carotid, coronary, renal, or peripheral arteries.
Magnetic resonance venography (MRV) can be used as an alternative to ultrasonography to detect deep venous thrombosis; however, MRV is less well studied and more expensive than ultrasonography.
Positron Emission Tomography (PET) in Cardiac Diagnosis
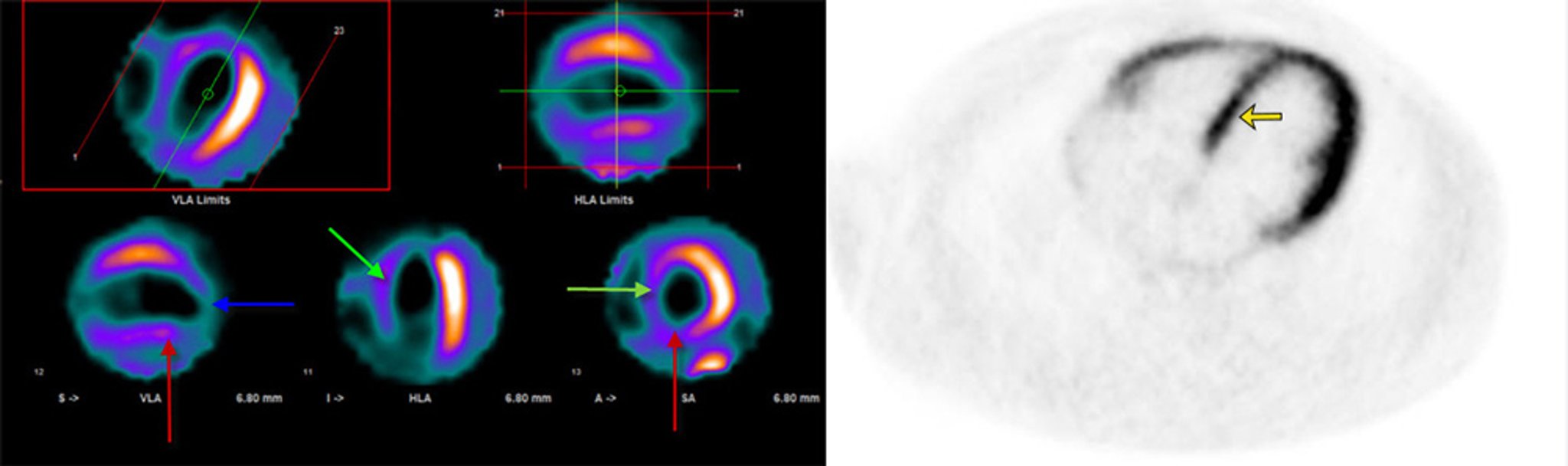
PET with CT (PET-CT) can demonstrate myocardial perfusion and metabolism and is increasingly being used to assess myocardial viability or to assess myocardial perfusion after an equivocal single-photon emission CT (SPECT) study or in patients with severe obesity.
Perfusion agents are radioactive nuclides that are used to trace the amount of blood flow entering a specific region and are therefore useful in unmasking myocardial perfusion deficits not evident at rest. They include carbon-11 (C-11) carbon dioxide, oxygen-15 (O-15) water, nitrogen-13 (N-13) ammonia, and rubidium-82 (Rb-82). Only Rb-82 does not require an on-site cyclotron.
Metabolic agents are radioactive analogs of normal biologic substances that are taken up and metabolized by cells. They include
Fluorine-18 (F-18)–labeled deoxyglucose (FDG)
C-11 acetate
FDG detects the enhancement of glucose metabolism under ischemic conditions, and can thus distinguish ischemic but still viable myocardium from scar tissue. Sensitivity is greater than with technetium-99m myocardial perfusion imaging, possibly making FDG imaging useful for selecting patients for revascularization and for avoiding such procedures when only scar tissue is present. This use may justify the greater expense of PET. Half-life of F-18 is long enough (110 min) that FDG can often be produced off-site. Techniques that enable FDG imaging to be used with conventional SPECT cameras may make this type of imaging widely available. FDG has also been used to detect inflammatory cardiovascular disorders (eg, infected pacemaker wires, aortic vasculitis, cardiac sarcoidosis).

© 2017 Elliot K. Fishman, MD.
Carbon-11 acetate uptake appears to reflect overall oxygen metabolism by myocytes. Uptake does not depend on such potentially variable factors as blood glucose levels, which can affect FDG distribution. C-11 acetate imaging may better predict postintervention recovery of myocardial function than FDG imaging. However, because of its 20-minute half-life, C-11 must be produced by an on-site cyclotron.






