


Echocardiography uses ultrasound waves to produce an image of the heart, the heart valves, and the great vessels. It helps assess heart wall thickness (eg, in hypertrophy or atrophy) and motion and provides information about ischemia and infarction. It can be used to assess systolic function as well as diastolic filling patterns of the left ventricle, which can help in the assessment of left ventricular hypertrophy, hypertrophic or restrictive cardiomyopathy, severe heart failure, and constrictive pericarditis. It also is used to assess the structure and function of the heart valves; detect valvular vegetations and intracardiac thrombus; and provide an estimate of pulmonary arterial pressure and central venous pressure.

Chris Gallagher/SCIENCE PHOTO LIBRARY
Techniques
There are 3 techniques for doing echocardiography:
Transthoracic
Transesophageal
Intracardiac
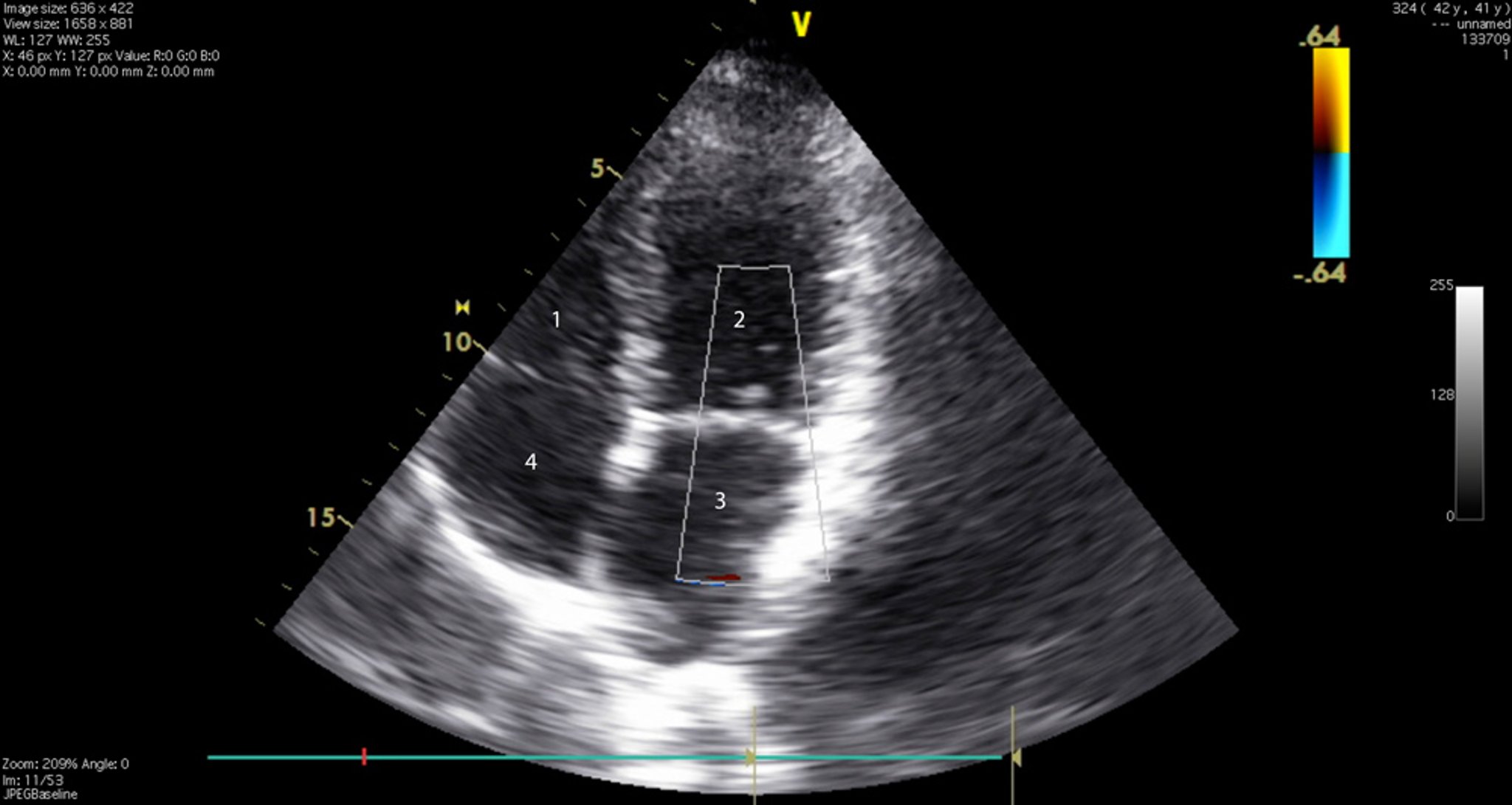
Transthoracic echocardiography (TTE) is the most common echocardiography technique. In TTE, a transducer is placed along the left or right sternal border, at the cardiac apex, at the suprasternal notch (to allow visualization of the aortic valve, left ventricular outflow tract, and descending aorta), or over the subxiphoid region. TTE provides 2- or 3-dimensional tomographic images of most major cardiac structures. TTE is a relatively inexpensive and non-invasive imaging technique for diagnosis of right and left ventricular function and wall motion, chamber size and anatomy, valvular structure function, aortic root structure and intracardiac pressures.
Point of care ultrasonography (POCUS) is a limited TTE (focused on detecting significant pericardial effusion and ventricular dysfunction) that is sometimes done at the bedside of critically ill patients in the intensive care unit (ICU) and emergency department (ED); many intensivists and emergency department physicians have training to do this procedure with portable hand-held machines when experienced radiologists or cardiologists are not available. Portable hand-held machines act as a good screening tool to determine which patients may require more detailed testing. With expanding use by less experienced clinicians, the major limitation is missed diagnoses. As a result, national societies are making recommendations for training in cardiovascular POCUS to facilitate the best use of the diagnostic test. Sites using cardiovascular POCUS should develop standards for use within their practice.
In transesophageal echocardiography (TEE), a transducer on the tip of an endoscope passed into the esophagus and stomach allows visualization of the heart. TEE is used to assess cardiac disorders when transthoracic study is technically difficult, as in patients with obesity or chronic obstructive pulmonary disease (COPD). It reveals better detail of small abnormal structures (eg, endocarditic vegetations or patent foramen ovale) and posterior cardiac structures (eg, left atrium, left atrial appendage, interatrial septum, pulmonary vein anatomy) because they are closer to the esophagus than to the anterior chest wall. TEE can also produce images of the ascending aorta, which arises behind the 3rd costal cartilage; of structures < 3 mm (eg, thrombi, vegetations); and of prosthetic valves.
In intracardiac echocardiography (ICE), a transducer on the tip of a catheter (inserted via the femoral vein and threaded to the heart) allows visualization of cardiac anatomy. ICE can be done during complex structural cardiac (eg, percutaneous closure of atrial septal defects or patent foramen ovale) or electrophysiologic procedures. ICE provides better image quality and decreased procedure time when compared with TEE during these procedures. However, ICE is generally more expensive.
Methodology
Two-dimensional echocardiography is most commonly used; contrast, Doppler and other echocardiography modalities provide additional information.
Contrast echocardiography
Spectral Doppler echocardiography can record velocity, direction, and type of blood flow. This technique is useful for detecting abnormal blood flow (eg, due to regurgitant lesions) or velocity (eg, due to stenotic lesions). Spectral Doppler echocardiography does not provide spatial information about the size or shape of the heart or its structures.
Color Doppler echocardiography combines 2-dimensional and spectral Doppler echocardiography to provide information about the size and shape of the heart and its structures as well as the velocity of and direction of blood flow around the valves and outflow tracts. Color is used to code blood flow information; by convention, red is toward and blue away from the transducer.
Tissue Doppler imaging uses Doppler techniques to measure the velocity of myocardial tissue contraction (rather than of blood flow). Myocardial tissue movement can also be evaluated with speckle-tracking echocardiography, which uses algorithms to track myocardial echo speckles (characteristic reverberations from the myocardium during an ultrasonography) from frame to frame. Strain imaging uses these data to calculate myocardial strain (percentage change in length between contraction and relaxation) and myocardial strain rate (rate of change in length). Strain and strain rate measurements can help assess systolic and diastolic function and identify ischemia during stress testing.
Three-dimensional echocardiography is increasingly used; special transducers can obtain a real-time, 3-dimensional image of cardiac structures. Three-dimensional echocardiography is particularly useful in evaluating the mitral valve apparatus for surgical correction. It is also increasingly being used to quantify right ventricular volumes, because the crescent shape of the right ventricle limits evaluation by 2-dimensional echocardiography, and during interventional procedures such as transcatheter edge-to-edge repair of the mitral valve. Use of 3-dimensional echocardiography continues to evolve.
Stress echocardiography
Transthoracic echocardiography is an alternative to radionuclide imaging to identify myocardial ischemia during and after exercise or pharmacologic stress testing
Stress echocardiography is valuable in evaluating the hemodynamic severity of aortic valve stenosis in patients with significant symptoms but whose resting transvalvular pressure gradient is not markedly high. Stress echocardiography and radionuclide stress testing detect ischemia equally well. The choice between tests is often based on availability, the provider’s experience, and cost.
Evidence of high left ventricular filling pressures during exercise, including elevated E/e' ratio (ratio of transmitral flow to mitral annular velocity) or elevated tricuspid regurgitant velocity, can be used to diagnose heart failure with preserved ejection fraction or dynamic valvular disease such as mitral regurgitation.






