


Bullous pemphigoid is a chronic autoimmune skin disorder resulting in generalized, pruritic, bullous lesions in older adults. Mucous membrane involvement is rare. Diagnosis is by skin biopsy and immunofluorescence testing of skin and serum. Topical and systemic corticosteroids are used initially. Most patients require long-term maintenance therapy, for which a variety of immunosuppressants can be used.
Bullae are elevated, fluid-filled blisters ≥ 10 mm in diameter.
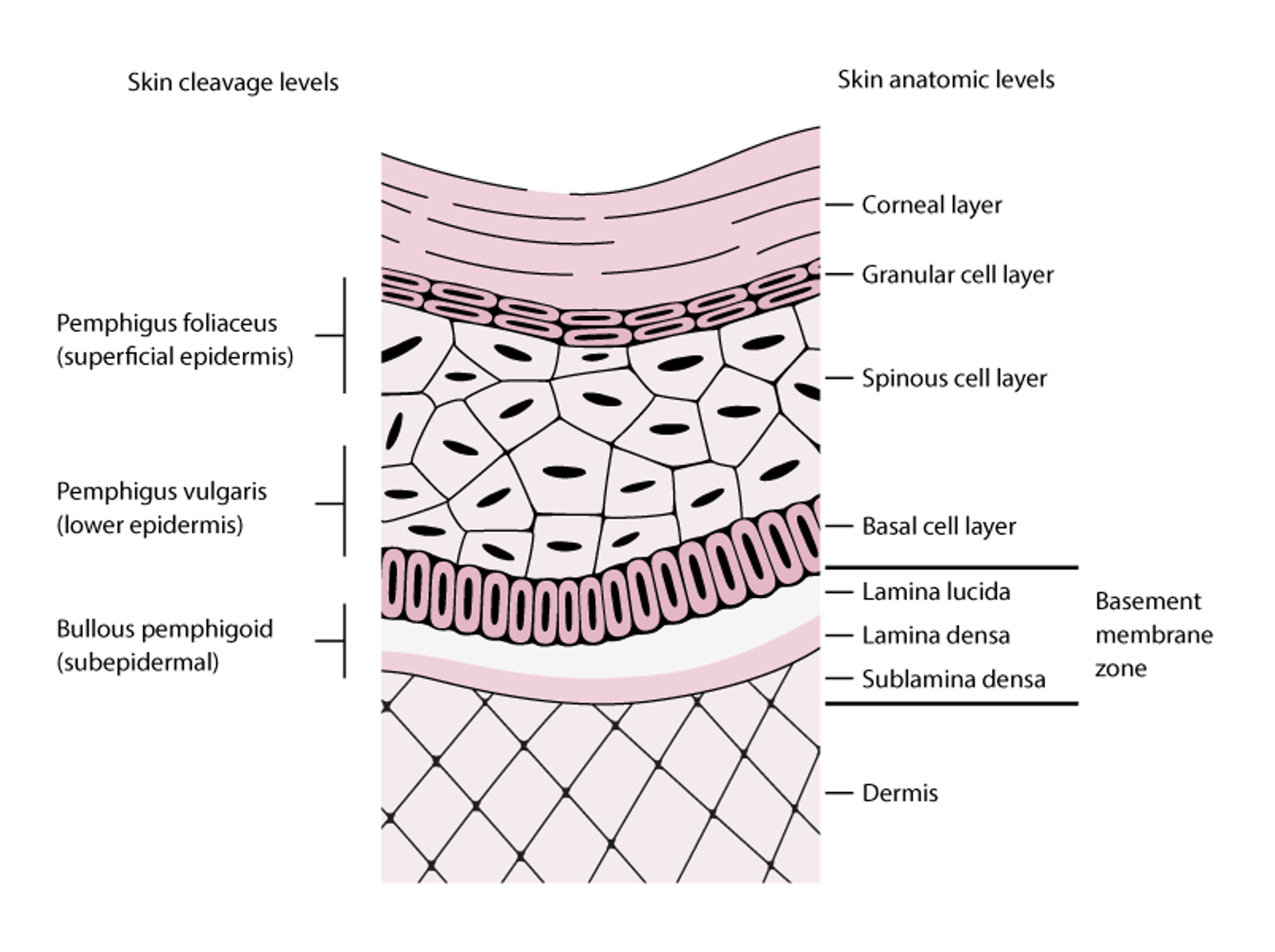
Bullous pemphigoid occurs more often in patients > age 60 but can occur in children. IgG autoantibodies bind to certain hemidesmosomal antigens (BPAg1 [BP230], BPAg2 [BP180]), resulting in the activation of complement to form a subepidermal blister (see figure Skin Cleavage Levels in Pemphigus and Bullous Pemphigoid).
Skin Cleavage Levels in Pemphigus and Bullous Pemphigoid
Pemphigus foliaceus blisters form in the superficial layers of the epidermis. Pemphigus vulgaris blisters can form at any epidermal level but typically form in the lower aspects of the epidermis. Bullous pemphigoid blisters form subepidermally (lamina lucida of the basement membrane zone). In this figure, the basement membrane zone is disproportionately enlarged to display its layers. |

Etiology of Bullous Pemphigoid
No cause of bullous pemphigoid has been proved; however, the following triggers have been suggested:
Skin disorders (including psoriasis, lichen planus, and some infections)
Disorders (diabetes mellitus, rheumatoid arthritis, ulcerative colitis, and multiple sclerosis)
Genetic and environmental factors may play a role.
Triggers may induce an autoimmune reaction by mimicking molecular sequences in the epidermal basement membrane (molecular mimicry, as with drugs and possibly infections), by exposing or altering normally tolerated host antigens (as with physical triggers and certain disorders), or by other mechanisms. Epitope spreading refers to the recruitment of autoreactive lymphocytes against normally tolerated host antigens, which contributes to disease chronicity and course.
Certain central nervous system (CNS) and psychiatric disorders may precede bullous pemphigoid, especially multiple sclerosis and schizophrenia, but also dementias, intracranial bleeds, stroke, delusional and personality disorders, and Parkinson disease
Symptoms and Signs of Bullous Pemphigoid
Pruritus is the first symptom of bullous pemphigoid. Skin lesions may not develop for several years. Often, characteristic tense bullae develop on skin of the trunk and in the flexural and intertriginous areas. Bullae may develop on normal-appearing skin or may be preceded by erythematous or urticarial-appearing plaques. Localized disease may occur at trauma sites, stomas, and anogenital and lower leg areas. Dyshidrotic pemphigoid is a rare form of bullous pemphigoid that affects the hands and feet and can look like dyshidrotic dermatitis (a form of hand and foot dermatitis) on the palms. Bullae usually do not rupture, but those that do often rapidly heal.
Polymorphic, annular, dusky-red, edematous lesions, with or without peripheral vesicles, can occur. Rarely, small blisters develop on the mucosa. Leukocytosis and eosinophilia are common, but fever is rare. The Nikolsky sign, where upper layers of epidermis move laterally with slight pressure or rubbing of skin adjacent to a blister, is negative.

© Springer Science+Business Media

Photo provided by Thomas Habif, MD.

Photo courtesy of Karen McKoy, MD.

Photo courtesy of Daniel M. Peraza, MD.

Photo courtesy of Karen McKoy, MD.


© Springer Science+Business Media


Photo provided by Thomas Habif, MD.


Photo courtesy of Karen McKoy, MD.


Photo courtesy of Daniel M. Peraza, MD.


Photo courtesy of Karen McKoy, MD.
Diagnosis of Bullous Pemphigoid
Skin biopsy and IgG titers
If blisters develop, bullous pemphigoid needs to be differentiated from pemphigus vulgaris, a blistering disorder with a worse prognosis; differentiation is usually possible using clinical criteria.
Test results help differentiate bullous pemphigoid from pemphigus vulgaris, linear IgA disease, erythema multiforme, drug-induced eruptions, mucous membrane pemphigoid, paraneoplastic pemphigoid, dermatitis herpetiformis, and epidermolysis bullosa acquisita.
If bullous pemphigoid is suspected, skin biopsy is done for histology and direct immunofluorescence testing. Samples from in and around the lesion itself are often used for histology, but samples of uninvolved skin (often about 3 mm from the edge of a lesion) are used for direct immunofluorescence. The blister in bullous pemphigoid is subepidermal, often containing many neutrophils and eosinophils. Direct immunofluorescence shows linear IgG and complement deposits along the basement membrane zone (dermal–epidermal junction). Indirect immunofluorescence shows circulating IgG deposits on the epidermal side of a salt-split preparation of normal (ie, test substrate) skin.
Serum is tested for IgG antibodies to BPAg1 and BPAg2 using an enzyme-linked immunosorbent assay (ELISA). Circulating IgG autoantibodies are present in about three fourths of patients (1). Newer, potentially more accurate ELISA tests are under investigation.
Diagnosis references
1. van Beek N, Krüger S, Fuhrmann T, et al: Multicenter prospective study on multivariant diagnostics of autoimmune bullous dermatoses using the BIOCHIP technology. J Am Acad Dermatol 83(5):1315-1322, 2020. doi: 10.1016/j.jaad.2020.01.049
Treatment of Bullous Pemphigoid
Corticosteroids, topical or oral
Anti-inflammatory drugs
Immunosuppressant drugs
1).
≤
Treatment reference
1. Borradori L, Van Beek N, Feliciani C, et al: Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol 36(10):1689-1704, 2022. doi: 10.1111/jdv.18220
Prognosis for Bullous Pemphigoid
Bullous pemphigoid is a chronic disease. Although topical and systemic therapies are helpful, they may cause adverse effects.
Remission is typical within months, but treatment is sometimes needed for several years.
Key Points
Bullous pemphigoid usually affects patients > age 60 and is autoimmune and idiopathic.
Pruritus may precede development of a rash by years, and mucous membrane involvement is rare.
Biopsy the skin for histology and immunofluorescence testing and measure circulating autoantibodies.
Treat patients with high-potency topical corticosteroids when possible to avoid or minimize use of systemic corticosteroids.
Anti-inflammatory and immunosuppressant therapy may be used to limit corticosteroid dose.
Symptoms usually lessen within months, but treatment is sometimes needed for several years.






