


Achalasia is a neurogenic esophageal motility disorder characterized by impaired esophageal peristalsis and a lack of lower esophageal sphincter relaxation during swallowing. Symptoms are slowly progressive dysphagia, usually to both liquids and solids, and regurgitation of undigested food. Evaluation typically includes manometry, barium swallow, and endoscopy. Treatments include dilation, botulinum toxin injection, surgical myotomy, and peroral endoscopic myotomy.
(See also Overview of Esophageal and Swallowing Disorders.)
Achalasia is thought to be caused by a loss of ganglion cells in the myenteric plexus of the esophagus, resulting in denervation of esophageal muscle. Etiology of the denervation is unknown, but viral and autoimmune causes are suspected, and certain tumors may cause achalasia either by direct obstruction or as a paraneoplastic process. Chagas disease, which causes destruction of autonomic ganglia, may result in achalasia.
Increased pressure at the lower esophageal sphincter (LES) causes obstruction with secondary dilation of the esophagus. Esophageal retention of undigested food and liquid is common.
Symptoms and Signs of Achalasia
Achalasia occurs at any age but usually begins between ages 20 and 60. Onset is insidious, and progression is gradual over months or years. Dysphagia for both solids and liquids is the major symptom. Nocturnal regurgitation of undigested food occurs in about 33% of patients and may cause cough and pulmonary aspiration. Chest pain is less common but may occur with swallowing or spontaneously.
Mild to moderate weight loss occurs; when weight loss is pronounced, particularly in older adults whose symptoms of dysphagia developed rapidly, pseudoachalasia secondary to a tumor of the gastroesophageal junction should be considered.
Diagnosis of Achalasia
Esophageal manometry
Sometimes barium swallow
Sometimes upper endoscopy
Sometimes functional lumen imaging probe (FLIP)
(See also the American College of Gastroenterology’s 2020 practice guidelines on the diagnosis and management of achalasia.)
Esophageal manometry is the preferred diagnostic test for achalasia. This test shows incomplete relaxation of the LES with a median integrated relaxation pressure ≥ 15, and 100% failed peristalsis.

© Springer Science+Business Media
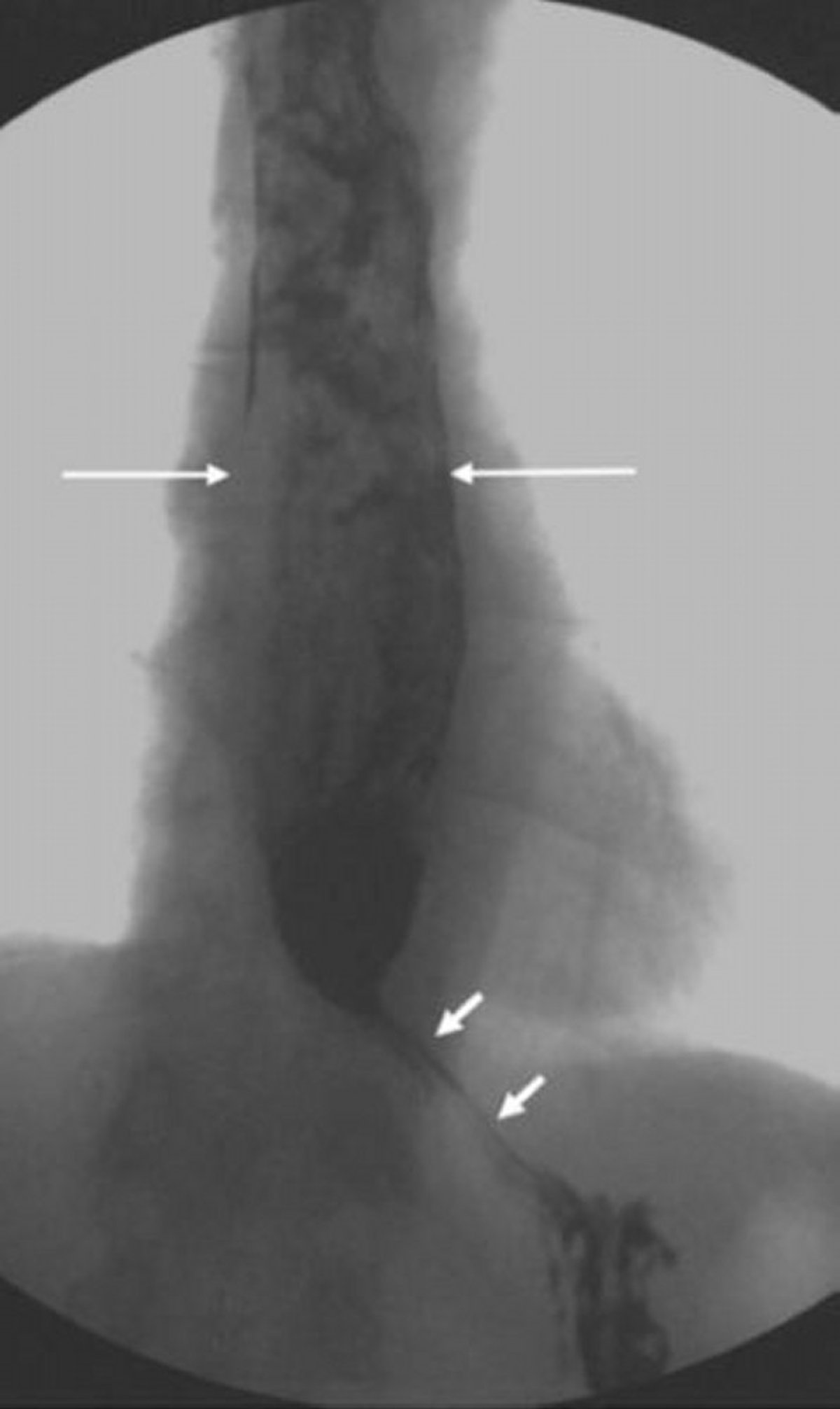
Barium swallow is a complementary test that is often done during the initial phase of testing when the cause of dysphagia is unknown because manometry is more invasive. Barium swallow may show absence of progressive peristaltic contractions during swallowing. Typically, the esophagus is dilated, often enormously, but is narrowed and beaklike at the LES.
Esophagoscopy is often done. Findings include upstream esophageal dilation and chronic stasis changes in the mucosa but no obstructing lesion. A classic "pop" is often felt when the esophagoscope passes into the stomach.
Impedance planimetry, when available, can be used to evaluate achalasia and can provide useful diagnostic information where manometry is nondiagnostic or if the patient cannot tolerate manometry. Guidelines recommend its use in the diagnosis and management of achalasia (1, 2). Additionally, in patients undergoing interventions for achalasia (eg, surgery, peroral endoscopic myotomy), measurement of esophagogastric junction distensibility during and after the intervention may show clinical response to interventions and can help guide therapy.
Functional lumen imaging probe (FLIP) is a high-resolution impedance system that assesses cross-sectional area and simultaneous pressure (distensibility) (3). FLIP is useful in diagnosing achalasia and may help in equivocal cases where manometry fails to diagnose achalasia despite a high clinical suspicion (4).
Achalasia must be differentiated from a peptic stricture, particularly in patients with systemic sclerosis, in whom esophageal manometry may also show aperistalsis. Systemic sclerosis is usually accompanied by a history of Raynaud phenomenon and symptoms of gastroesophageal reflux disease (GERD) due to low resting LES pressure.
Symptoms similar to those of achalasia (ie, pseudoachalasia) may be due to cancer at the gastroesophageal junction, which can be diagnosed by CT of the chest and abdomen or by endoscopic ultrasound with biopsy.
Diagnosis references
1. Gyawali CP, Carlson DA, Chen JW, et al: ACG clinical guidelines: Clinical use of esophageal physiologic testing. Am J Gastroenterol 115(9):1412–1428, 2020. doi: 10.14309/ajg.0000000000000734
2. Hirano I, Pandolfino JE, Boeckxstaens GE: Functional lumen imaging probe for the management of esophageal disorders: Expert review from the clinical practice updates committee of the AGA Institute. Clin Gastroenterol Hepatol 15(3):325–334, 2017. doi: 10.1016/j.cgh.2016.10.022
3. Carlson DA, Lin Z, Kahrilas PJ, et al: High-Resolution Impedance Manometry Metrics of the Esophagogastric Junction for the Assessment of Treatment Response in Achalasia. Am J Gastroenterol 111(12):1702-1710, 2016. doi: 10.1038/ajg.2016.442
4. Vaezi MF, Pandolfino JE, Yadlapati RH, et al: ACG Clinical Guidelines: Diagnosis and Management of Achalasia. Am J Gastroenterol 115(9):1393-1411, 2020. doi: 10.14309/ajg.0000000000000731
Treatment of Achalasia
Pneumatic balloon dilation of the LES
Surgical myotomy of the LES
Peroral endoscopic myotomy
Sometimes botulinum toxin injection
No therapy restores peristalsis; treatment of achalasia is aimed at reducing the pressure at the LES.
The choice of specific therapy is based on achalasia subtype, procedure risk, and potential adverse effects. Pneumatic balloon dilation of the LES and surgical or peroral endoscopic myotomy appear similarly effective. A randomized trial involving patients with achalasia found that at 5-year follow-up pneumatic balloon dilation had comparable efficacy to laparoscopic Heller myotomy (1). A posthoc analysis of these data according to achalasia subtypes found better results with pneumatic balloon dilation for patients with type II achalasia (swallowing increases pressure in the entire esophagus) and better results with Heller myotomy for type III achalasia (spastic achalasia; swallowing often results in lumen-obliterating contractions). Both procedures produced similar outcomes in patients with type I achalasia (classic achalasia; swallowing results in no change in esophageal pressure) (1, 2). The most concerning complication of these procedures is esophageal perforation. Perforation rates vary by center, ranging from 0 to 14% for pneumatic balloon dilation and 0 to 4.6% for laparoscopic Heller myotomy (3). Other studies have shown peroral endoscopic myotomy to have good short-term and long-term outcomes (4). However, postprocedure gastroesophageal reflux disease rates are higher in patients who undergo peroral endoscopic myotomy than in those who undergo Heller myotomy.
In patients who are not candidates for these treatment options, chemical denervation of cholinergic nerves in the distal esophagus by direct endoscopic injection of botulinum toxin type A into the LES may be tried. Clinical improvement usually occurs in 70 to 80% of patients for the first month (5); results decline over time but may last 6 months to over 1 year.
Medications such as nitrates or calcium channel blockers have been used in the past but have not been shown to be effective.
Treatment references
1. Moonen A, Annese V, Belmans A, et al: Long-term results of the European achalasia trial: A multicentre randomised controlled trial comparing pneumatic dilation versus laparoscopic Heller myotomy. Gut 65(5):732–739, 2016. doi: 10.1136/gutjnl-2015-310602
2. Pandolfino JE, Kwiatek MA, Nealis T, et al: Achalasia: A new clinically relevant classification by high-resolution manometry. Gastroenterology 135(5):1526–1533, 2008. doi: 10.1053/j.gastro.2008.07.022
3. Lynch KL, Pandolfino JE, Howden CW, et al: Major complications of pneumatic dilation and Heller myotomy for achalasia: Single-center experience and systematic review of the literature. Am J Gastroenterol 107(12):1817–1825, 2012. doi: 10.1038/ajg.2012.332
4. Rentein DV, Fuchs K-H, Fockens P, et al: Peroral endoscopic myotomy for the treatment of achalasia: An international prospective multicenter study. Gastroenterology 145(2):272–273, 2013. doi: 10.1053/j.gastro.2013.04.057
5. Campos GM, Vittinghoff E, Rabl C, et al: Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Ann Surg 249(1):45-57, 2009. doi: 10.1097/SLA.0b013e31818e43ab
Prognosis for Achalasia
Esophageal dilation and tortuosity are poor prognostic indicators. Pulmonary aspiration is a late-stage complication. Nocturnal regurgitation and coughing suggest aspiration. Pulmonary complications secondary to aspiration are difficult to manage.
Incidence of esophageal cancer in patients with achalasia is not currently thought to be increased.
Key Points
A loss of ganglion cells in the myenteric plexus of the esophagus, thought to be viral- or autoimmune-induced, decreases esophageal peristalsis and impairs relaxation of the lower esophageal sphincter (LES).
Patients gradually develop dysphagia for both solids and liquids, and about one third regurgitate undigested food at night.
Esophageal manometry is the preferred test for achalasia and shows an elevated integrated relaxation pressure in conjunction with 100% failed peristalsis.
Barium swallow shows absence of progressive peristaltic contractions during swallowing and a markedly dilated esophagus with beaklike narrowing at the LES.
No therapy restores peristalsis; treatment is aimed at reducing the pressure (and thus the obstruction) at the LES.
Treatment is typically pneumatic balloon dilation or myotomy of the LES; patients who are not candidates for these treatments may be given botulinum toxin type A injections.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American College of Gastroenterology: Practice guidelines on the diagnosis and management of achalasia (2020)






