


Light microscopy can be done quickly, but accuracy depends on the experience of the microscopist and quality of equipment. Regulations often limit physicians’ use of microscopy for diagnostic purposes outside a certified laboratory.
Microscopic examination of tissue may be required to distinguish invasive disease from surface colonization—a distinction not easily achieved by culture methods.
Most specimens are treated with stains that color pathogens, causing them to stand out from the background, although wet mounts of unstained samples can be used to detect fungi and certain other pathogens.
The clinician orders a stain based on the likely pathogens. However, no stain is 100% specific (ie, different organisms may stain similarly). Most samples are treated with Gram stain and, if mycobacteria are suspected, with an acid-fast stain. However, some pathogens are not easily visible using these stains; if these pathogens are suspected, different stains or other identification methods are required.
Because microscopic detection usually requires a microbe concentration of at least about 1 ×104-5/mL, most body fluid specimens (eg, cerebrospinal fluid) are concentrated (eg, by centrifugation) before examination.
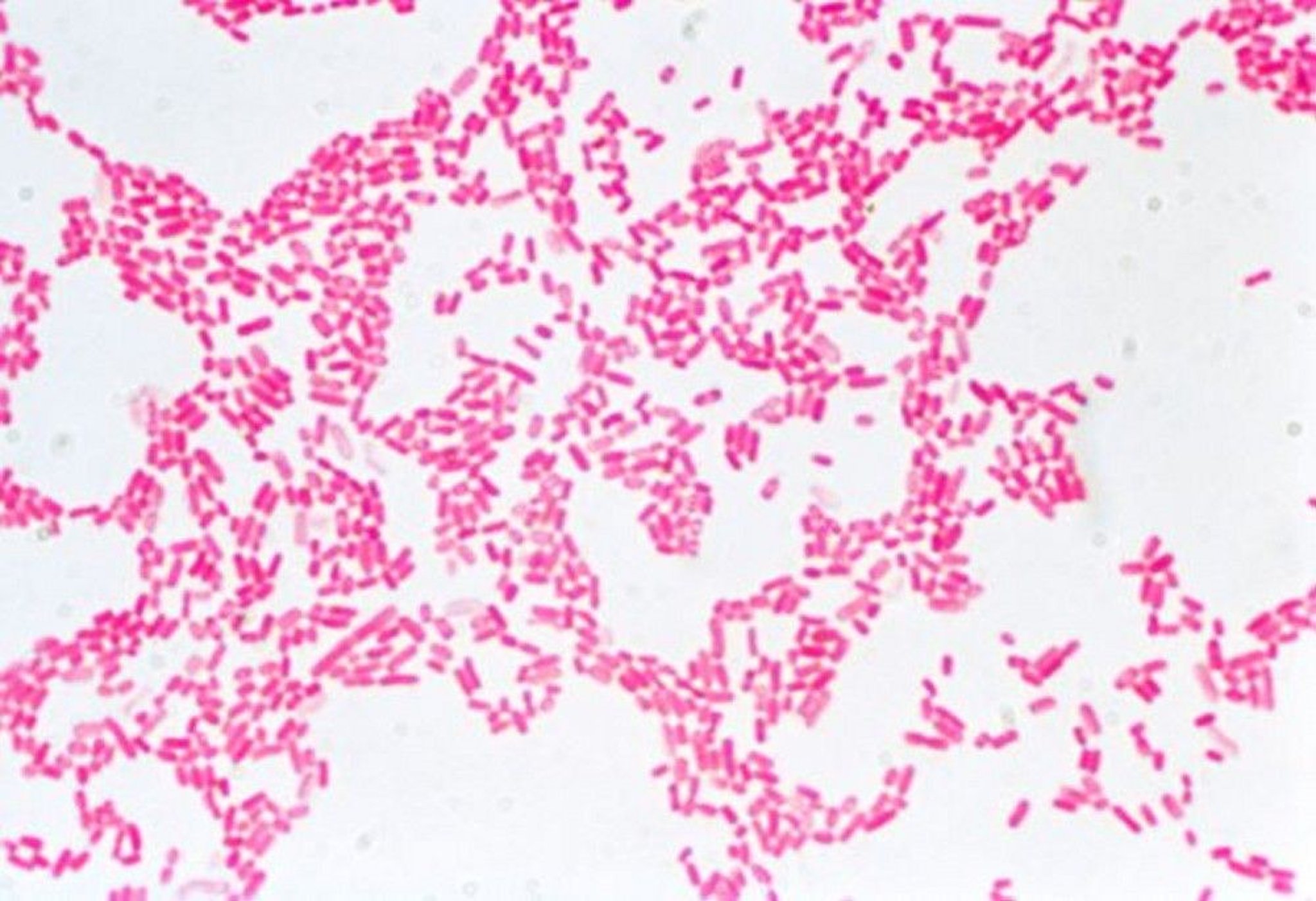
Gram stain
The Gram stain does the following:

DR. ROSALIND KING/SCIENCE PHOTO LIBRARY

CNRI/SCIENCE PHOTO LIBRARY
Classifies bacteria according to whether they retain crystal violet stain (gram-positive—blue) or not (gram-negative—red)
Highlights cell morphology (eg, bacilli, cocci) and cell arrangement (eg, clumps, chains, diploids)
Identifies polymorphonuclear leukocytes, indicating bacterial infection rather than colonization
Such characteristics can direct antibiotic therapy pending definitive identification. Finding a mixture of microorganisms with multiple morphologies and staining characteristics on Gram stain suggests a contaminated specimen or a polymicrobial bacterial infection. Finding many squamous cells in a sputum specimen suggests that the specimen is contaminated with saliva and thus is of limited diagnostic usefulness.
To do a Gram stain, technicians heat-fix specimen material to a slide and stain it by sequential exposure to Gram crystal violet, iodine, decolorizer, and counterstain (typically safranin).
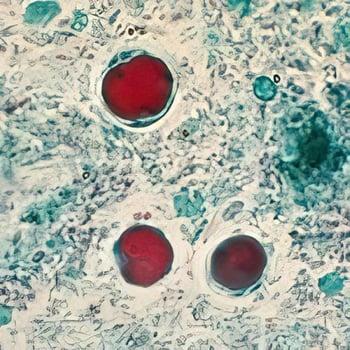
Acid-fast and modified acid-fast stains
These stains are used to identify the following:


CDC/SCIENCE PHOTO LIBRARY

WEBPATHOLOGY/SCIENCE PHOTO LIBRARY
Acid-fast organisms (Mycobacterium species)
Moderately acid-fast organisms (primarily Nocardia species)
Rhodococcus and related genera
Oocysts of some parasites (eg, Cryptosporidium, microsporidia, Cystoisospora [Isospora] belli, Cyclospora, Balantidium coli)
Although detection of mycobacteria in sputum requires at least 10,000 organisms/mL, mycobacteria are often present in lower levels, so sensitivity is limited. Usually, several mL of sputum are decontaminated with sodium hydroxide and concentrated by centrifugation for acid-fast staining. Specificity is better, although some moderately acid-fast organisms are difficult to distinguish from mycobacteria.
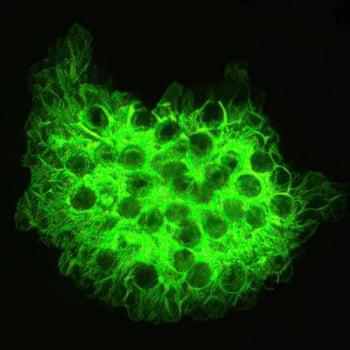
Fluorescent stains
Fluorescent stains allow detection at lower concentrations (< 1 × 104 cells/mL). Examples are
Acridine orange (bacteria and fungi)
Auramine-rhodamine and auramine O (mycobacteria)
Calcofluor white (fungi, especially dermatophytes)
Coupling a fluorescent dye to an antibody directed at a pathogen (direct or indirect immunofluorescence) should theoretically increase sensitivity and specificity. However, these tests are difficult to read and interpret, and few (eg, Pneumocystis and Legionella direct fluorescent antibody tests) are commercially available and commonly used.
Wet mounts
Wet mounts of unstained samples can be used to detect the following via darkfield microscopy:
Parasites (including helminth eggs and larvae)
Vaginal clue cells (present in bacterial vaginosis)
Motile organisms (eg, Trichomonas)
Treponema spirochetes (present in syphilis)
Visibility of fungi can be increased by applying 10% potassium hydroxide (KOH) to dissolve surrounding tissues and nonfungal organisms.
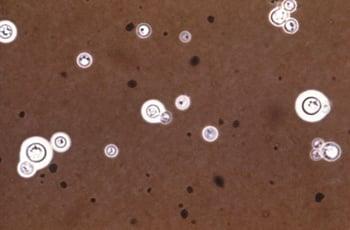
India ink (colloidal carbon) stain
India ink stain is used to detect mainly Cryptococcus neoformans and other encapsulated fungi in a cell suspension (eg, cerebrospinal fluid sediment). The background field, rather than the organism itself, is stained, making any capsule around the organism visible as a halo. In cerebrospinal fluid, the test is not as sensitive as cryptococcal antigen. Specificity is also limited; leukocytes may appear encapsulated.

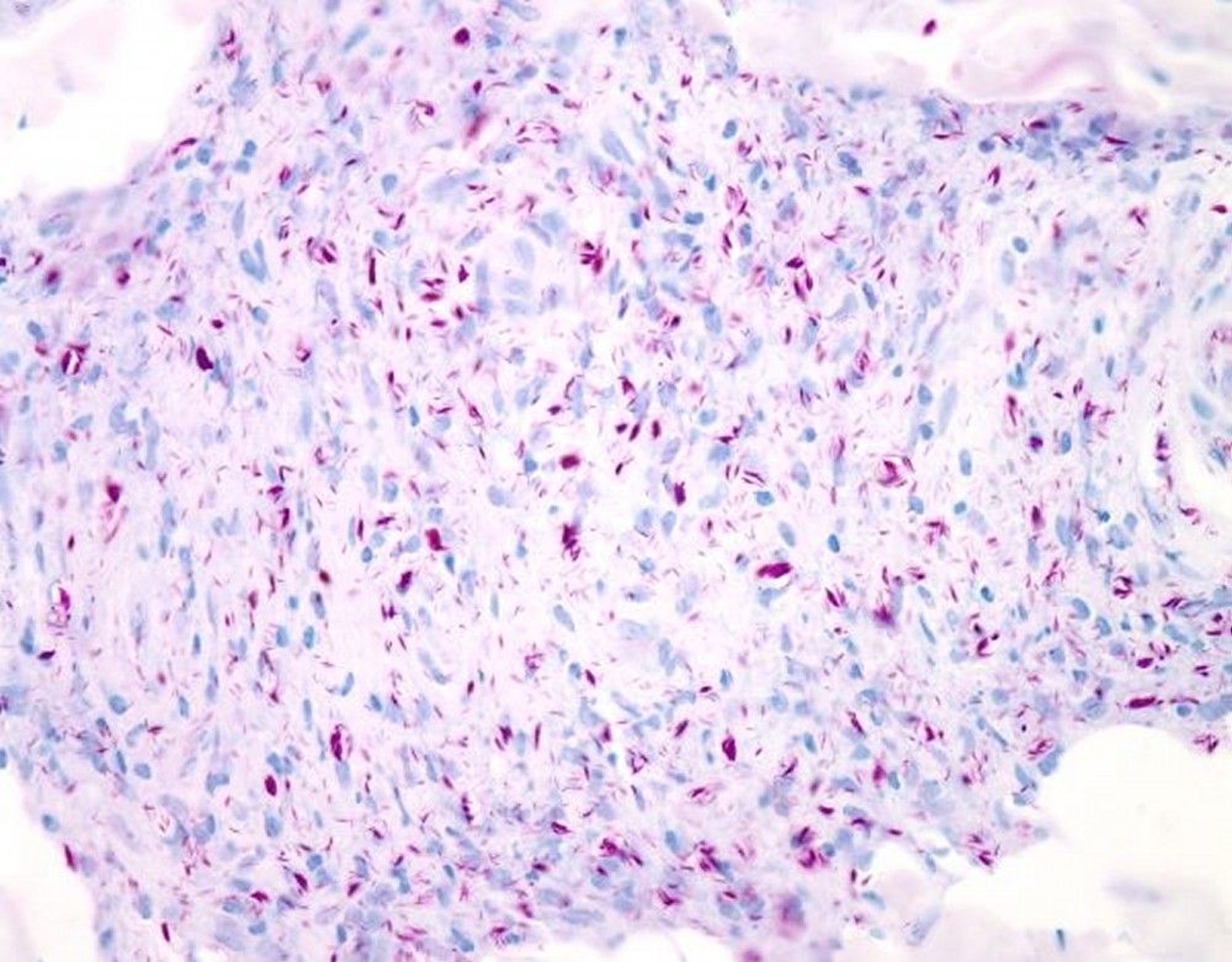
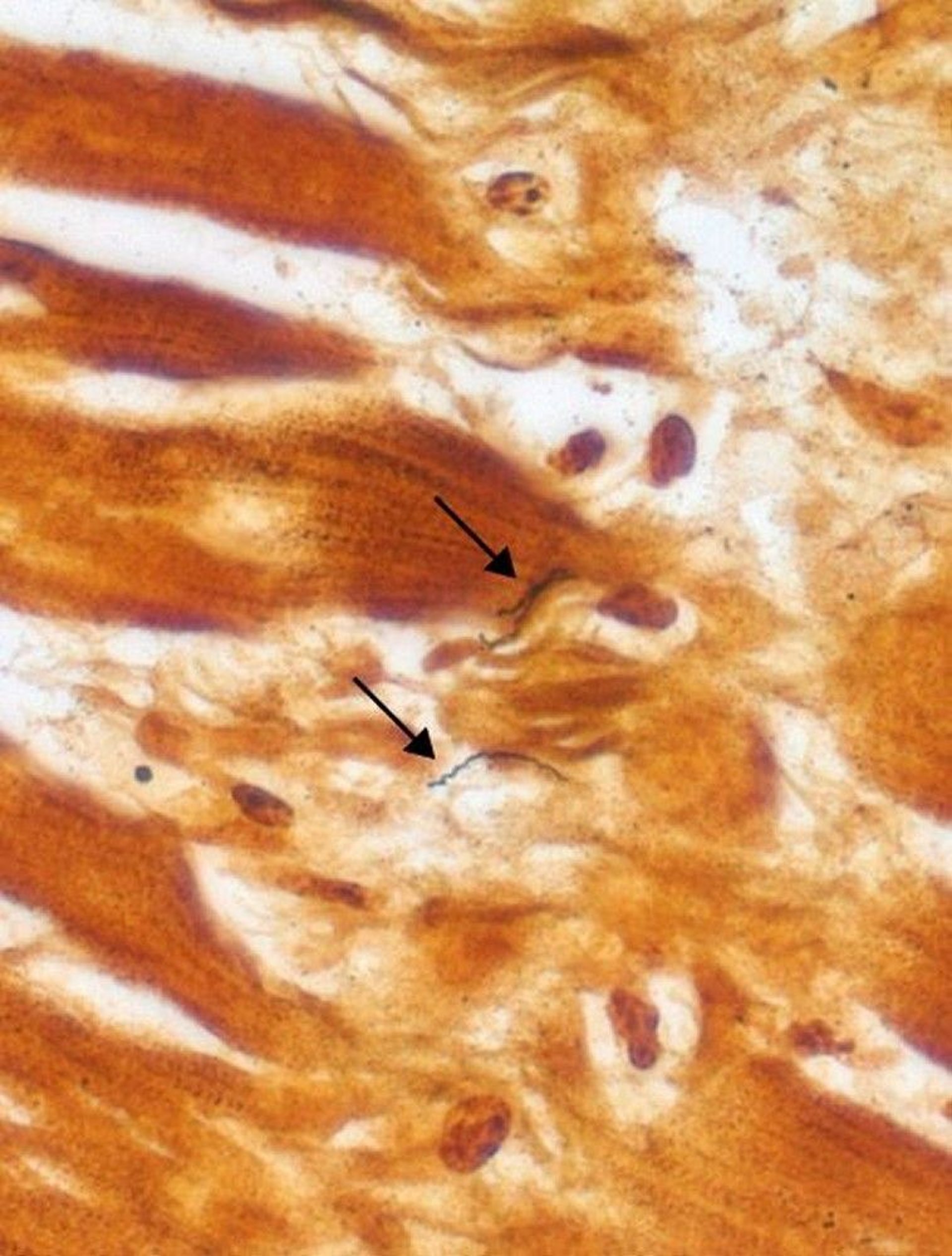
Warthin-Starry stain and Dieterle stain
These silver stains are used to visualize bacteria such as

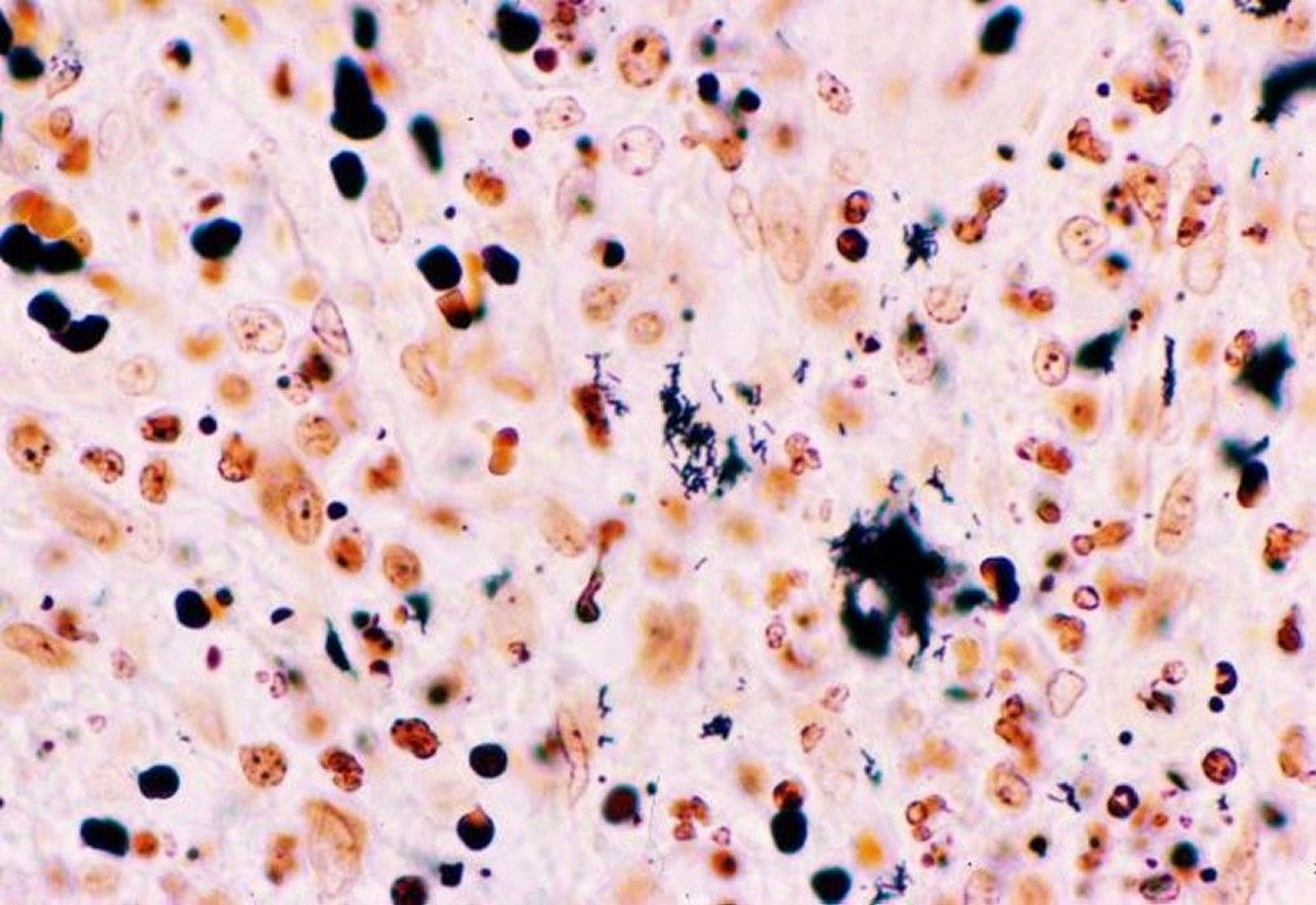
WEBPATHOLOGY/SCIENCE PHOTO LIBRARY

CDC/Sherif Zaki, M.D. Ph.D.; DVBD/SCIENCE PHOTO LIBRARY
Bartonella henselae (the cause of cat-scratch disease)
Wright stain and Giemsa stain
These stains are used for detection of the following:

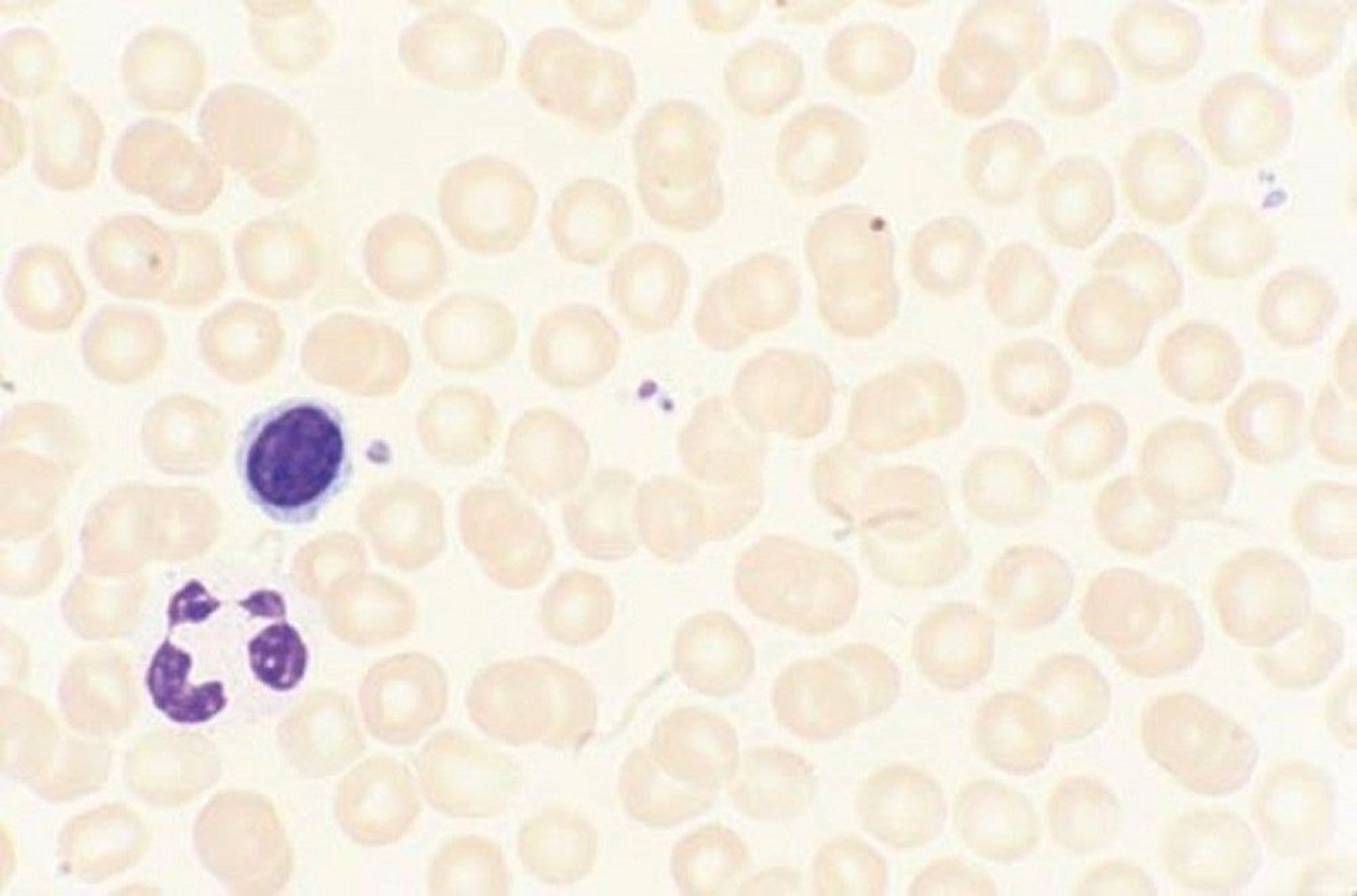
By permission of the publisher. From Tefferi A, Li C. In Atlas of Clinical Hematology. Edited by JO Armitage. Philadelphia, Current Medicine, 2004.
Parasites in blood
Histoplasma capsulatum in phagocytes and tissue cells
Intracellular inclusions formed by viruses and chlamydia
Trophozoites of Pneumocystis jirovecii
Some intracellular bacteria
Trichrome stain (Gomori-Wheatley stain) and iron hematoxylin stain
These stains are used to detect intestinal protozoa.
The Gomori-Wheatley stain is used to detect microsporidia. It may miss helminth eggs and larvae and does not reliably identify Cryptosporidium. Fungi and human cells take up the stain.
The iron hematoxylin stain differentially stains cells, cell inclusions, and nuclei. Helminth eggs may stain too dark to permit identification.






