


Leprosy is a chronic infection usually caused by the acid-fast bacilli Mycobacterium leprae or the closely related organism M. lepromatosis
M. leprae was the only known cause of leprosy until 2008, when a second species, M. lepromatosis was identified in Mexico. Together, these two organisms are called M. leprae complex.
In much of the world, leprosy is rare. It is a complex, poorly understood, and difficult-to-study infection.
Although leprosy is not highly contagious (contrary to popular belief), rarely causes death, and can be effectively treated with antibiotics, it continues to be associated with considerable social stigma. Misunderstanding about the disease probably exists because leprosy was incurable before the advent of effective antibiotic therapy in the 1940s. People with the disease would become disfigured and often have significant disability, causing them to be feared and shunned by others. Because of this social stigma, the psychologic impact of leprosy is often significant.
Epidemiology of Leprosy
Globally, the number of leprosy cases is declining. In 2020, about 130,000 new cases were reported, and about 73% of cases occurred in India, Brazil, and Indonesia (1).
In 2020, 159 new cases were reported in the US; about three quarters occurred in 6 states: California, Florida, Hawaii, Louisiana, New York, and Texas (2). Most cases of leprosy in the US involve people who emigrated from or worked in countries where leprosy is common. Most of the indigenously acquired cases involved people who live in southern states where nine-banded armadillos infected with unique genotypes of M. leprae are found. These same unique genotypes are found in US patients who likely acquired leprosy in the US, and many of these patients reported direct contact with armadillos (3).
Leprosy can develop at any age. Older age is a risk factor, but disease occurs most often in people aged 5 to 15 years or > 30 years.
Epidemiology references
1. World Health Organization (WHO): Leprosy (Hansen's disease). Accessed 4/26/2022.
2. Health Resources and Services Administration: National Hansen's Disease (Leprosy) Program Caring and Curing Since 1894. Accessed 4/26/2022.
3. Truman RW, Singh P, Sharma R, et al: Probable zoonotic leprosy in the southern United States. N Engl J Med 364(17):1626–1633, 2011. doi: 10.1056/NEJMoa1010536
Pathophysiology of Leprosy
Humans are the main natural reservoir for M. leprae. Armadillos are the only confirmed source other than humans, although other animal and environmental sources may exist.
Leprosy is thought to be spread by passage from person to person through nasal droplets and secretions. Casual contact (eg, simply touching someone with the infection) and short-term contact does not seem to spread it. About half of people with leprosy probably contracted it through close, long-term contact with an infected person. Even after contact with the bacteria, most people do not develop leprosy; health care workers often work for many years with people who have leprosy without contracting it. Most immunocompetent people who are infected with M. leprae do not develop leprosy because of effective immunity. People who do develop leprosy probably have a poorly defined genetic predisposition.
M. leprae grow slowly (doubling in 2 weeks). The usual incubation period ranges from 6 months to 10 years. Once infection develops, hematogenous dissemination can occur.
Classification of leprosy
Leprosy is classified by type and number of skin areas affected:
Paucibacillary: ≤ 5 skin lesions with no bacteria detected on samples from those areas
Multibacillary: ≥ 6 skin lesions, bacteria detected on samples from skin lesions, or both
Leprosy also is classified by cellular response and clinical findings:
Tuberculoid
Lepromatous
Borderline
People with tuberculoid leprosy typically have a strong cell-mediated response, which limits disease to a few skin lesions (paucibacillary), and the disease is milder, less common, and less contagious.
People with lepromatous or borderline leprosy typically have poor cell-mediated immunity to M. leprae and have more severe, systemic infection with widespread bacterial infiltration of skin, nerves, and other organs (eg, nose, testes, kidneys). They have more skin lesions (multibacillary), and the disease is more contagious.
In both classifications, the type of leprosy dictates
Long-term prognosis
Likely complications
Duration of antibiotic treatment
Symptoms and Signs of Leprosy
Symptoms of leprosy usually do not begin until > 1 year after infection (average 5 to 7 years). Once symptoms begin, they progress slowly.


CNRI/SCIENCE PHOTO LIBRARY

ST MARY'S HOSPITAL MEDICAL SCHOOL/SCIENCE PHOTO LIBRARY
Leprosy affects mainly the skin and peripheral nerves. Nerve involvement causes numbness and weakness in areas controlled by the affected nerves.
Tuberculoid leprosy: Skin lesions consist of one or a few hypoesthetic, centrally hypopigmented macules with sharp, raised borders. The rash, as in all forms of leprosy, is nonpruritic. Areas affected by this rash are numb because of damage to the underlying peripheral nerves, which may be palpably enlarged.
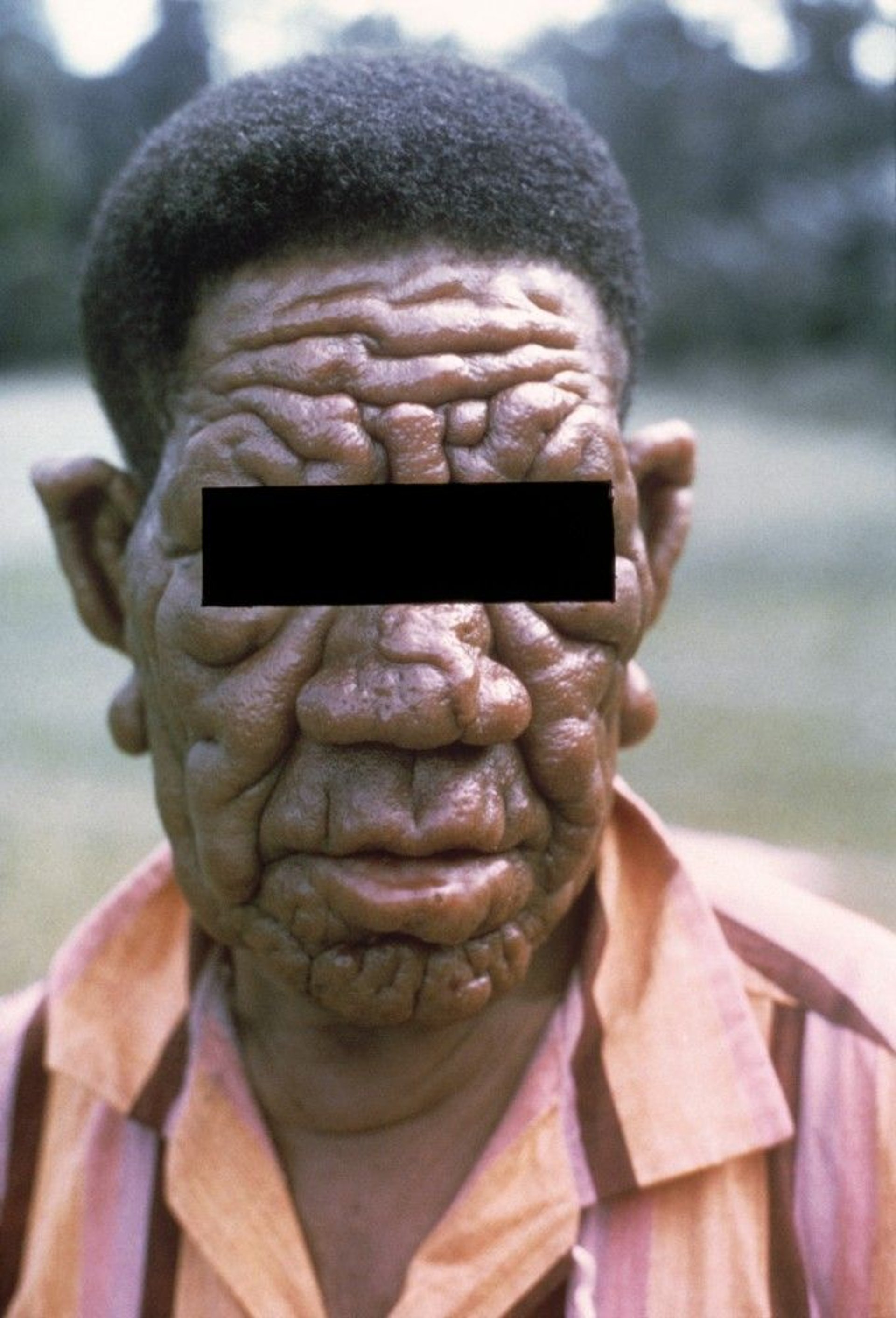
Lepromatous leprosy: Much of the skin and many areas of the body, including the kidneys, nose, and testes, may be affected. Patients have skin macules, papules, nodules, or plaques, which are often symmetric. Peripheral neuropathy is more severe than in tuberculoid leprosy, with more areas of numbness; certain muscle groups may be weak. Patients may develop gynecomastia or lose eyelashes and eyebrows.
Borderline leprosy: Features of both tuberculoid and lepromatous leprosy are present. Without treatment, borderline leprosy may become less severe and more like the tuberculoid form, or it may worsen and become more like the lepromatous form.
Complications of leprosy
The most severe complications result from the peripheral neuropathy, which causes deterioration of the sense of touch and a corresponding inability to feel pain and temperature. Patients may unknowingly burn, cut, or otherwise harm themselves. Repeated damage may lead to loss of digits. Muscle weakness can result in deformities (eg, clawing of the 4th and 5th fingers caused by ulnar nerve involvement, foot drop caused by peroneal nerve involvement).


Papules and nodules can be particularly disfiguring on the face.

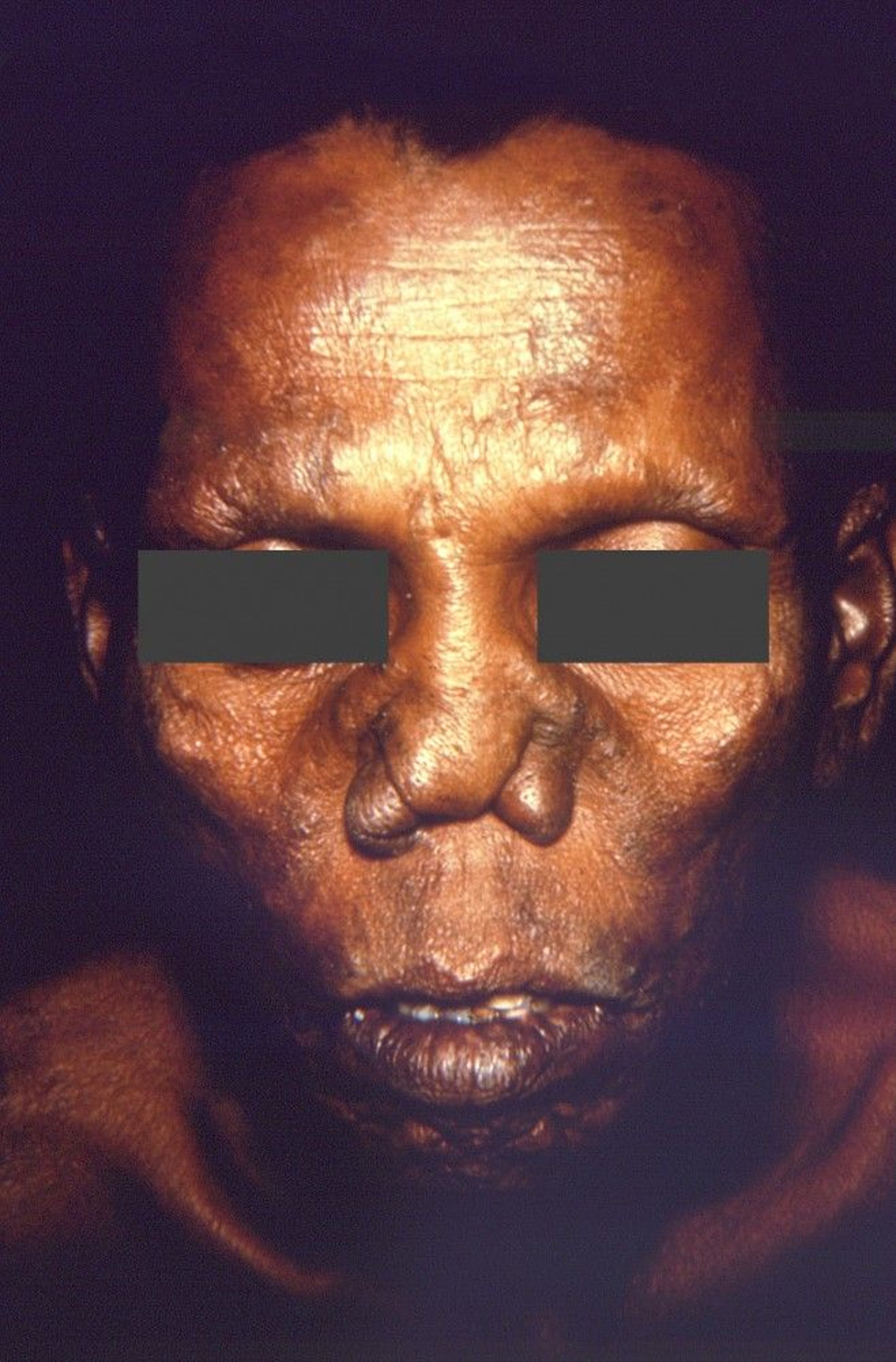
Image courtesy of Dr. Andre J. Lebrun via the Public Health Image Library of the Centers for Disease Control and Prevention.
Other areas of the body may be affected:
Feet: Plantar ulcers with secondary infection are a major cause of morbidity, making walking painful.
Nose: Damage to the nasal mucosa can result in chronic nasal congestion and nosebleeds and, if untreated, erosion and collapse of the nasal septum.
Eyes: Iritis may lead to glaucoma, and corneal insensitivity may lead to scarring and blindness.
Sexual function: Men with lepromatous leprosy may have erectile dysfunction and infertility. The infection can reduce testosterone and sperm production by the testes.
Kidneys:Amyloidosis and consequent renal failure occasionally occur in lepromatous leprosy.
Leprosy reactions
During the course of untreated or even treated leprosy, the immune system may produce inflammatory reactions. There are 2 types.
Type 1 leprosy reactions result from a spontaneous increase in cell-mediated immunity. These reactions can cause fever and inflammation of the preexisting skin and peripheral nerve lesions, resulting in skin edema, erythema, and tenderness and worsening nerve function. These reactions, particularly if not treated early, contribute significantly to nerve damage. Because the immune response is increased, these reactions are termed reversal reactions, despite the apparent clinical worsening.
Type 2 leprosy reactions
Diagnosis of Leprosy
Microscopic examination of skin biopsy specimen
Diagnosis of leprosy is often delayed in the US because clinicians are unfamiliar with the clinical manifestations.
Leprosy is suggested by the presence of skin lesions and peripheral neuropathy and confirmed by microscopic examination of biopsy specimens. M. leprae and M. lepromatosis do not grow on artificial culture media. Biopsy specimens should be taken from the advancing edge of tuberculoid lesions or, in lepromatous leprosy, from nodules or plaques.

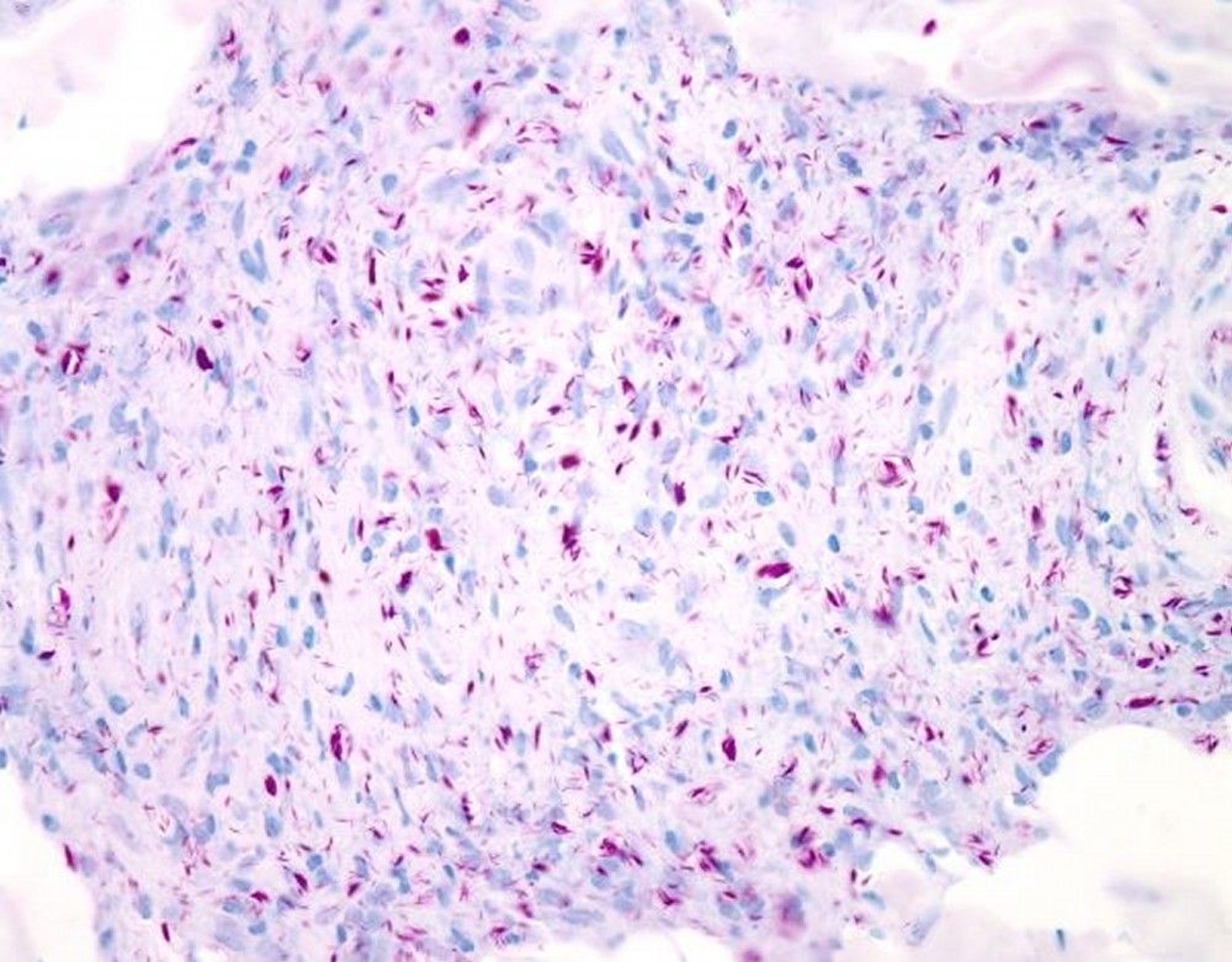
WEBPATHOLOGY/SCIENCE PHOTO LIBRARY
Serum IgM antibodies to M. leprae are specific but insensitive (present in only two thirds of patients with tuberculoid leprosy). Diagnostic usefulness is further limited in endemic areas because such antibodies may be present in asymptomatic infection.
Treatment of Leprosy
Sometimes lifelong maintenance antibiotics
Antibiotics can stop the progression of leprosy but do not reverse any nerve damage or deformity. Thus, early detection and treatment are vitally important.
Because of antibiotic resistance, multidrug regimens are used. The drugs chosen depend on the type of leprosy; multibacillary leprosy requires more intensive regimens and a longer duration than paucibacillary leprosy does.
Advice about diagnosis and treatment is available from the US Health Resources and Services Administration's National Hansen’s Disease (Leprosy) Program (or call 1-800-642-2477). Standard regimens recommended by the World Health Organization (WHO) differ somewhat from those used in the US (see the WHO's 2018 guidelines for the diagnosis, treatment and prevention of leprosy).
Multibacillary leprosy
The standard WHO regimen includes dapsone, rifampin, and clofazimine
Paucibacillary leprosy
Drugs for leprosy
is relatively inexpensive and generally safe to use. Adverse effects include hemolysis and anemia (which are usually mild) and allergic dermatoses (which can be severe); rarely, dapsone syndrome (exfoliative dermatitis, high fever, mononucleosis-like white blood cell differential) occurs.
is primarily bactericidal for M. leprae and is even more effective than dapsone. However, if given at the recommended US dosage of 600 mg orally once/day, it is too expensive for many poorer countries, but it is available free from the WHO. Adverse effects include hepatotoxicity, flu-like syndromes, and, rarely, thrombocytopenia and renal failure.
is extremely safe. The main side effect is reversible skin pigmentation, but discoloration may take months to resolve. Clofazimine can be obtained in the US only from the Department of Health and Human Services as an investigational new drug. To request further information or investigator status to be able to use clofazimine, clinicians can contact the National Hansen's Disease (Leprosy) Program or call 1-800-642-2477.
Leprosy reactions
National Hansen's Disease (Leprosy) Program). However, because of its teratogenicity, thalidomide should not be given to women who may become pregnant. Adverse effects are mild constipation, mild leukopenia, and sedation.
Prevention of Leprosy
Because leprosy is not very contagious, risk of spread is low. Only the untreated lepromatous form is contagious, but even then, the infection is not easily spread. However, household contacts (particularly children) of patients with leprosy should be monitored for development of symptoms and signs of leprosy. Once treatment has begun, leprosy cannot be spread.
The best prevention is
Avoiding contact with bodily fluids from and the rash on infected people
2018 WHO guidelines recommend a single dose of rifampicin as preventive treatment for contacts of leprosy patients who are ≥ 2 years of age. This treatment is given only after leprosy and TB disease have been ruled out and no other contraindications exist.
Key Points
Leprosy is a chronic infection usually caused by the acid-fast bacilli Mycobacterium leprae.
Leprosy is not very contagious in untreated patients and not at all contagious once treatment starts.
Leprosy affects mainly the skin and peripheral nerves.
The most severe complications result from loss of the sense of touch, pain, and temperature; muscle weakness that can result in deformities; and disfiguring lesions of the skin and nasal mucosa.
Inflammatory reactions called leprosy reactions can occur and require treatment with corticosteroids.
Diagnose based on biopsy; M. leprae and M. lepromatosis cannot be grown in culture.
dapsone and rifampin for paucibacillary.
More Information
The following are some English-language resources that may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
US Health Resources and Services Administration: National Hansen’s Disease (Leprosy) Program (or call 1-800-642-2477)
World Health Organization (WHO): Guidelines for the diagnosis, treatment and prevention of leprosy (2018)






