


Angiostrongyliasis is infection with larvae of worms of the genus Angiostrongylus. Depending on the infecting species, abdominal symptoms (Angiostrongylus costaricensis) or neural involvement with eosinophilic meningitis (A. cantonensis) result. Diagnosis is suspected by history and presence of eosinophilia in cerebrospinal fluid (CSF) and/or blood. Anthelmintics are either ineffective or deleterious.
(See also Approach to Parasitic Infections.)
Angiostrongylus are parasites of rats (rat lung worms). Excreted larvae are taken up by intermediate hosts (land snails and slugs) and paratenic or transport hosts (hosts that are not required for the parasite's development but that can transmit infection to humans). Human infection is acquired by ingestion of raw or undercooked snails or slugs or transport hosts (certain land crabs, freshwater shrimp and prawns, frogs, or toads); it is unclear whether larval contamination of vegetables (eg, in slime from snails or slugs that crawl on the food) can cause infection.

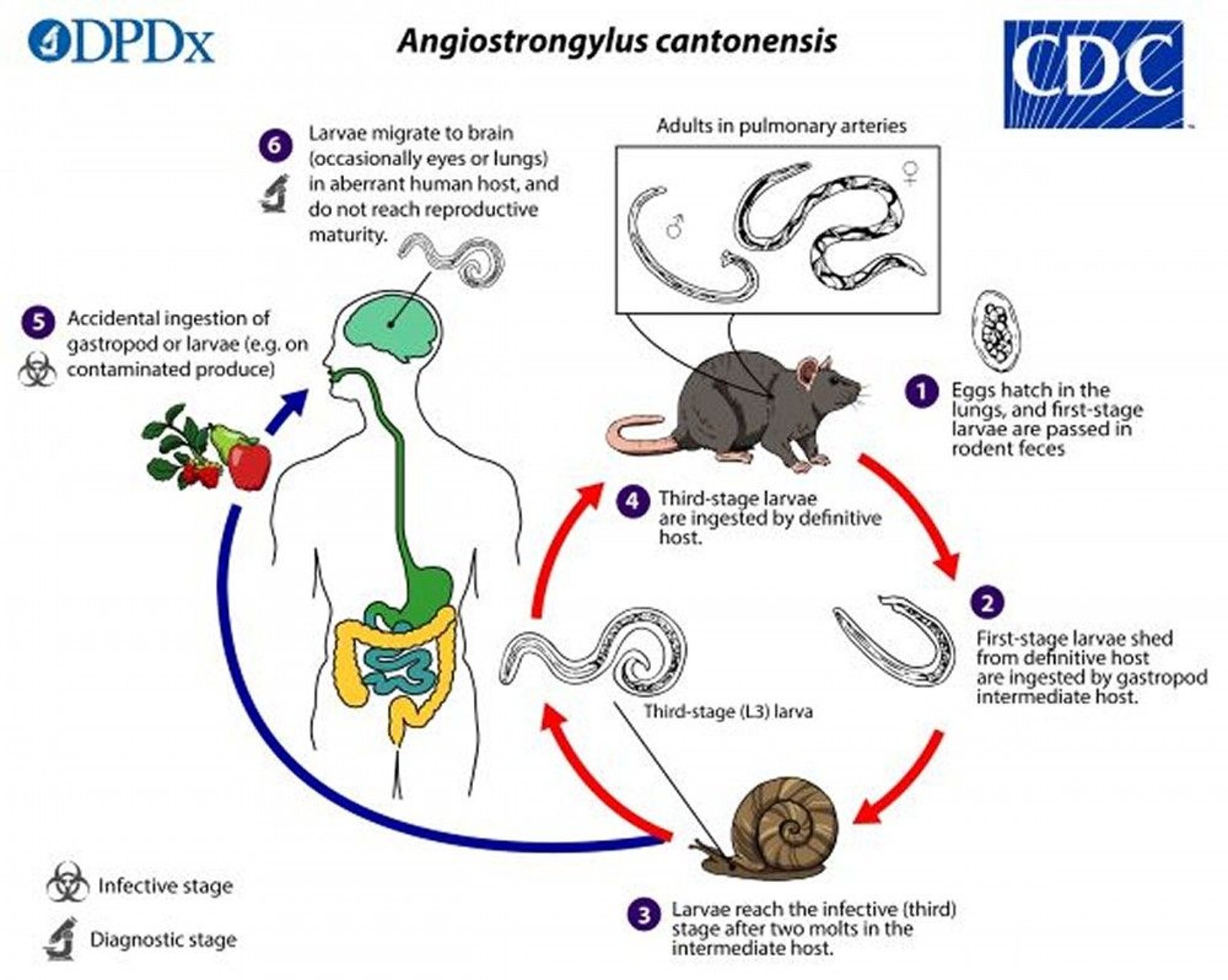
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
A. cantonensis infection (neural angiostrongyliasis) occurs predominantly in Southeast Asia and the Pacific Basin, although infection has been reported elsewhere, including the Caribbean, Hawaii, and parts of the southern United States. The larvae migrate from the gastrointestinal (GI) tract to the meninges, where they cause eosinophilic meningitis, with fever, headache, and meningismus, accompanied by eosinophilia. Occasionally, ocular invasion occurs.
A. costaricensis infection (abdominal angiostrongyliasis) occurs in the Americas, predominantly in Latin America and the Caribbean. Adult worms reside in arterioles of the ileocecal area, and eggs can be released into the intestinal tissues, resulting in local inflammation with abdominal pain, vomiting, and fever; this infection can mimic appendicitis. Abdominal angiostrongyliasis is often accompanied by eosinophilia, and a painful right lower quadrant mass may develop.
Diagnosis of Angiostrongyliasis
If meningitis signs are present, cerebrospinal fluid (CSF) analysis and complete blood count (A. cantonensis)
Sometimes identification of eggs and larvae in tissue obtained during abdominal surgery (A. costaricensis)
Angiostrongyliasis is suspected based on a history of ingesting potentially contaminated material, including land snails, slugs, or transfer hosts such as certain land crabs, frogs, toads, or freshwater prawns or shrimp.
Patients with meningeal findings require lumbar puncture, which typically shows elevated CSF pressure, protein, and white cells with eosinophils > 10%. Complete blood count shows eosinophilia > 5% in blood; A. cantonensis parasites are rarely visible. Focal lesions are not usually seen in CT of the brain. A. cantonensis larvae and eggs are not present in stool.
Diagnosis of gastrointestinal infection due to A. costaricensis is difficult because larvae and eggs are not present in stool; however, if surgery is done (eg, for suspected appendicitis), eggs and larvae can be identified in tissues removed during surgery. A high percentage of eosinophils (>10%) may be present in blood.
Immunoassays are not widely available. The Centers for Disease Control and Prevention (CDC) offers a polymerase chain reaction (PCR) for A. cantonensis in CSF; molecular tests for A. costaricensis are available only in research laboratories.
Treatment of Angiostrongyliasis
For meningitis, analgesics, corticosteroids, and removal of cerebrospinal fluid (CSF)
A. cantonensis meningitis is treated with analgesics, removal of CSF at frequent intervals to reduce central nervous system (CNS) pressure; corticosteroids can decrease the frequency of therapeutic lumbar puncture. Anthelmintic therapy may increase the inflammatory response because it results in the release of parasite antigens. Most patients have a self-limited course and recover completely.
There is no specific treatment for A. costaricensis infection; most infections resolve spontaneously. Anthelmintics do not appear to be effective and may lead to additional migration of worms and worsening symptoms.
Prevention of Angiostrongyliasis
People who live in or travel to areas with A. cantonensis should avoid eating raw or undercooked snails, slugs, freshwater shrimp, land crabs, frogs, centipedes, and lizards, as well as potentially contaminated vegetables and vegetable juices.
People who live in or travel to areas with A. costaricensis should avoid eating raw or undercooked slugs and potentially contaminated vegetables or juices.
Key Points
Humans acquire Angiostrongylus when they consume raw or undercooked snails or slugs or the organisms' transport hosts (certain land crabs, frogs, toads, or freshwater prawns or shrimp).
A. cantonensis larvae migrate from the gastrointestinal tract to the meninges, where they cause eosinophilic meningitis; A. costaricensis eggs can be released into the intestinal tissues, causing abdominal pain, vomiting, and fever.
Eggs are not present in the stool of patients with angiostrongyliasis.
Treat A. cantonensis neural infection with meningitis with analgesics, corticosteroids, and, if intracranial pressure is elevated, removal of cerebrospinal fluid at frequent intervals.
Treating A. costaricensis abdominal infection with anthelmintics does not appear to be effective and may lead to additional migration of worms and worsening symptoms; most of these infections resolve spontaneously.






