


Multiple sclerosis (MS) is characterized by disseminated patches of demyelination in the brain and spinal cord. Common symptoms include visual and oculomotor abnormalities, paresthesias, weakness, spasticity, urinary dysfunction, and mild cognitive symptoms. Typically, neurologic deficits are multiple, with remissions and exacerbations gradually producing disability. Diagnosis requires clinical or MRI evidence of ≥ 2 characteristic neurologic lesions that are separated in both time and space (location in the central nervous system). Treatment includes corticosteroids for acute exacerbations, immunomodulatory medications to prevent exacerbations, and supportive measures.
(See also Overview of Demyelinating Disorders.)
Multiple sclerosis is believed to involve an immunologic mechanism. One postulated cause is infection by a latent virus (possibly a human herpesvirus such as Epstein-Barr virus), which, when activated, triggers a secondary autoimmune response.
An increased incidence among certain families and presence of human leukocyte antigen (HLA) allotypes (HLA-DR2) suggests genetic susceptibility.
Age at onset ranges from 15 to 60 years, typically 20 to 40 years; women are affected somewhat more often.
Neuromyelitis optica spectrum disorder (Devic disease), previously considered a variant of MS, is now recognized as a separate disorder.
Pathophysiology of Multiple Sclerosis
Localized areas of demyelination (plaques) occur, with destruction of oligodendroglia, perivascular inflammation, and chemical changes in lipid and protein constituents of myelin in and around the plaques. Axonal damage is common, and neuronal cell bodies may also die or be damaged.
Fibrous gliosis develops in plaques that are disseminated throughout the central nervous system (CNS), primarily in white matter, particularly in the lateral and posterior columns (especially in the cervical regions), optic nerves, and periventricular areas. Tracts in the midbrain, pons, and cerebellum are also affected. Gray matter in the cerebrum and spinal cord can be affected but to a much lesser degree.
Symptoms and Signs of Multiple Sclerosis
Multiple sclerosis is characterized by varied CNS deficits, with remissions and recurring exacerbations. When MS is not treated with immunomodulating medications, exacerbations average about 1 every 2 years, but frequency varies greatly.
Although MS may progress and regress unpredictably, there are typical patterns of progression:
Relapsing-remitting pattern: Exacerbations alternate with remissions, when partial or full recovery occurs or symptoms are stable. Remissions may last months or years. Exacerbations can occur spontaneously or can be triggered by an infection such as influenza. Relapsing forms of MS include active secondary MS (defined as a clinical relapse or new lesion seen on an MRI scan of the brain or spinal cord).
Primary progressive pattern: The disease progresses gradually with no remissions, although there may be temporary plateaus during which the disease does not progress. Unlike in the relapsing-remitting pattern, there are no clear exacerbations.
Secondary progressive pattern: This pattern begins with relapses alternating with remissions (relapsing-remitting pattern), followed by gradual progression of the disease.
Progressive relapsing pattern: The disease progresses gradually, but progression is interrupted by sudden, clear relapses. This pattern is rare.
The most common initial symptoms of multiple sclerosis are the following:
Paresthesias in one or more extremities, in the trunk, or on one side of the face
Weakness or clumsiness of a leg or hand
Visual disturbances (eg, partial loss of vision and pain in one eye due to retrobulbar optic neuritis, diplopia due to internuclear ophthalmoplegia, scotomas)
Other common early symptoms of MS include slight stiffness or unusual fatigability of a limb, minor gait disturbances, vertigo, and mild affective disturbances; all usually indicate scattered CNS involvement and may be subtle. Most patients with MS have difficulty with bladder control (eg, frequency, urgency, hesitancy, incontinence, retention). Fatigue is common. Excess heat (eg, warm weather, a hot bath, fever) may temporarily exacerbate symptoms and signs (Uhthoff phenomenon).
Mild cognitive symptoms are common. Apathy, poor judgment, or inattention may occur. Affective disturbances, including emotional lability, euphoria, or, most commonly, depression, are common. Depression may be reactive or partly due to cerebral lesions of MS. A few patients have seizures.
Cranial nerves
Unilateral or asymmetric optic neuritis and bilateral internuclear ophthalmoplegia are typical.
Central vision is affected more than peripheral vision.
Optic neuritis causes loss of vision (ranging from scotomas to blindness), eye pain during eye movement, and sometimes abnormal visual fields, a swollen optic disk, or a partial or complete afferent pupillary defect.
Internuclear ophthalmoplegia results if there is a lesion in the medial longitudinal fasciculus connecting the 3rd, 4th, and 6th nerve nuclei. During horizontal gaze, adduction of one eye is decreased, with nystagmus of the other (abducting) eye; convergence is intact. In MS, internuclear ophthalmoplegia is typically bilateral; unilateral internuclear ophthalmoplegia is often caused by ischemic stroke.
Rapid, small-amplitude eye oscillations in straight-ahead (primary) gaze (pendular nystagmus) are uncommon but characteristic of MS. Vertigo is common. Intermittent unilateral facial numbness or pain (resembling trigeminal neuralgia), palsy, or spasm may occur. Mild dysarthria may occur, caused by bulbar weakness, cerebellar damage, or disturbance of cortical control. Other cranial nerve deficits are unusual but may occur secondary to brain stem injury.
Motor
Weakness is common. It usually reflects corticospinal tract damage in the spinal cord, affects the lower extremities preferentially, and is bilateral and spastic.
Deep tendon reflexes (eg, knee and ankle jerks) are usually increased, and an extensor plantar response (Babinski sign) and clonus are often present. Spastic paraparesis produces a stiff, imbalanced gait; in advanced cases, it may confine patients to a wheelchair. Painful flexor spasms in response to sensory stimuli (eg, bedclothes) may occur late. Cerebral or cervical spinal cord lesions may result in hemiparesis, which sometimes is the presenting symptom.
Reduced mobility increases the risk of osteoporosis.
Cerebellar
In advanced MS, cerebellar ataxia plus spasticity may be severely disabling; other cerebellar manifestations include slurred speech, scanning speech (slow enunciation with a tendency to hesitate at the beginning of a word or syllable), and Charcot triad (intention tremor, scanning speech, and nystagmus).
Sensory
Paresthesias and partial loss of any type of sensation are common and often localized (eg, to one or both hands or legs).
Various painful sensory disturbances (eg, burning or electric shocklike pains) can occur spontaneously or in response to touch, especially if the spinal cord is affected. An example is Lhermitte sign, an electric shocklike pain that radiates down the spine or into the legs or arms when the neck is flexed.
Objective sensory changes tend to be transient and difficult to demonstrate early in the disease.
Spinal cord
Involvement commonly causes bladder dysfunction (eg, urinary urgency or hesitancy, partial retention of urine, mild urinary incontinence). Constipation, erectile dysfunction in men, and genital anesthesia in women may occur. Frank urinary and fecal incontinence may occur in advanced MS.
Spinal cord lesions (plaques) are a common source of neuropathic pain.
Progressive myelopathy, a variant of MS, causes spinal cord motor weakness but no other deficits.
Diagnosis of Multiple Sclerosis
Clinical criteria
Brain and spinal MRI
Sometimes cerebrospinal fluid (CSF) IgG levels and evoked potentials
Multiple sclerosis is suspected in patients with optic neuritis, internuclear ophthalmoplegia, or other symptoms that suggest MS, particularly if deficits are multifocal or intermittent. If MS is suspected, brain MRI and spinal MRI are done.
MRI is the most sensitive imaging test for MS and can exclude other treatable disorders that may mimic MS, such as nondemyelinating lesions at the junction of the spinal cord and medulla (eg, subarachnoid cyst, foramen magnum tumors). Gadolinium-contrast enhancement can distinguish actively inflamed from older plaques. Also, higher-field MRI magnets (3 to 7 Tesla) can distinguish perivenular MS plaques from nonspecific white-matter lesions.

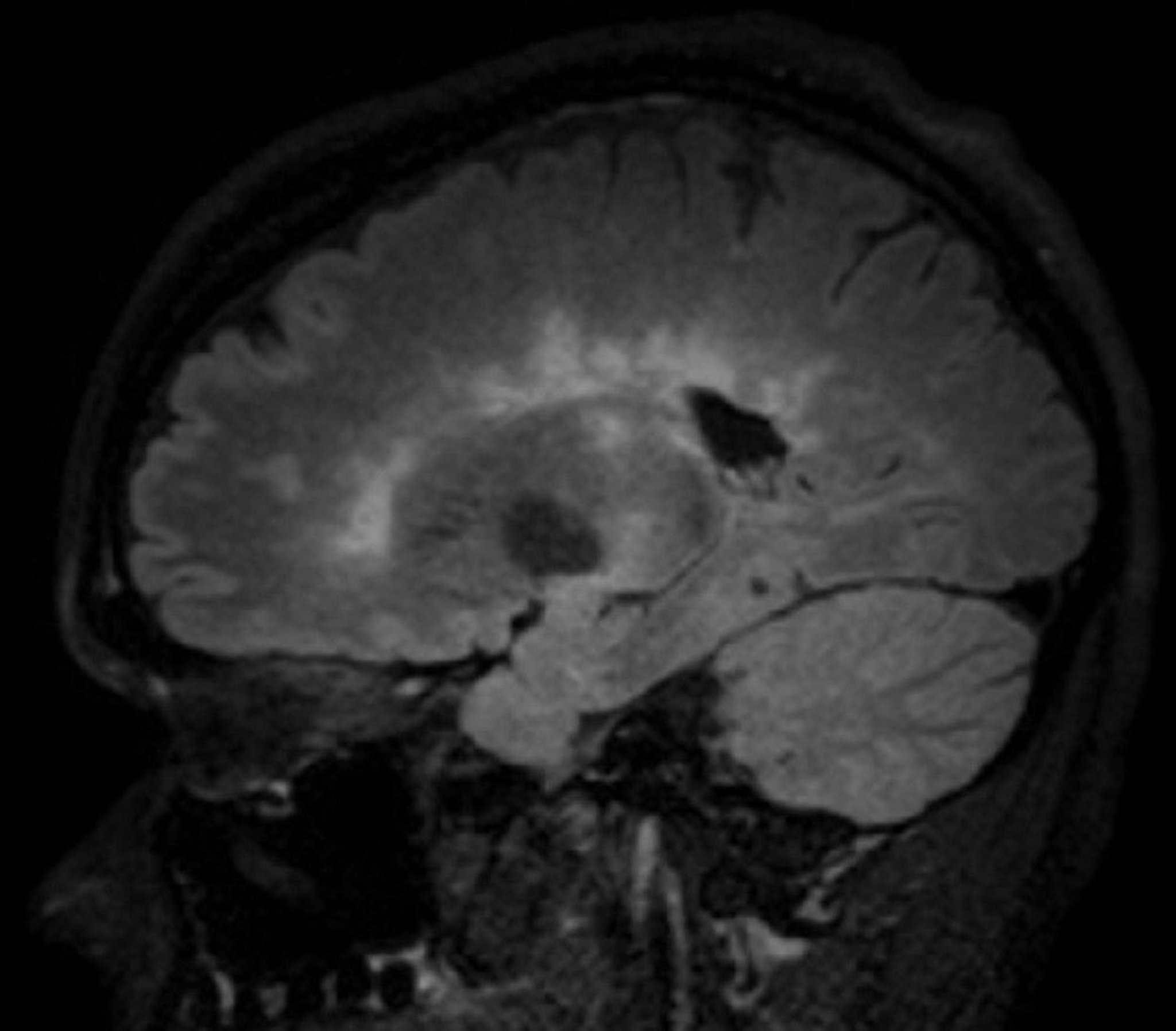
© 2017 Elliot K. Fishman, MD.
MS must be distinguished from the following:
Clinically isolated syndromes (consisting of only a single clinical manifestation typical of MS)
Radiologically isolated syndrome (MRI findings typical of MS that are incidentally noted in patients with no clinical manifestations)
MS can be distinguished because diagnosis of MS requires evidence of CNS lesions that are separated in both time and space (location in the CNS). For example, any of the following can indicate separation in time:
A history of exacerbations and remissions
MRI that shows simultaneous enhancing and nonenhancing lesions, even if patients are asymptomatic
A new lesion on a subsequent MRI in patients with a previous lesion
Separation (dissemination) in space can be established by finding lesions in ≥ 2 of the 5 following CNS areas typically affected by MS (1):
Periventricular: ≥ 3 lesions
Cortical/juxtacortical (white matter next to cortex and/or cortex): ≥ 1 lesions
Infratentorial: ≥ 1 lesions
Spinal cord: ≥ 1 lesions
Optic nerve: ≥ 1 lesions (either by MRI or clinical evaluation)
Additional testing
If MRI plus clinical findings are not diagnostic, additional testing may be necessary to objectively demonstrate separate neurologic abnormalities. Such testing may include evoked potentials and, occasionally, CSF examination or blood tests.
Evoked potentials (delays in electrical responses to sensory stimulation) are often more sensitive for MS than symptoms or signs. Visual evoked responses are sensitive and particularly helpful in patients with no confirmed cranial lesions (eg, those with lesions only in the spinal cord). Somatosensory evoked potentials and brain stem auditory evoked potentials are sometimes also measured.
CSF examination is being done less frequently (because the diagnosis can usually be based on MRI) but can be helpful if MRI plus clinical findings are inconclusive or if infection (eg, CNS Lyme disease<
Blood tests may be necessary. Sometimes systemic disorders (eg, SLE) and infections (eg, Lyme disease) can mimic MS and should be excluded with specific blood tests. Blood tests to measure an IgG antibody specific for neuromyelitis optica spectrum disorder (aquaporin-4 antibody [also known as NMO-IgG] and anti-MOG [myelin oligodendrocyte glycoprotein] antibodies) may be done to differentiate that disorder from MS.
Diagnosis reference
1. Filippi M, Rocca MA, Ciccarelli O, et al: MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines. Lancet Neurol 15 (3):292–303, 2016. doi: 10.1016/S1474-4422(15)00393-2
Treatment of Multiple Sclerosis
Corticosteroids
Immunomodulators to prevent exacerbations and delay eventual disability
Supportive care
Goals for treatment of multiple sclerosis include the following:
Shortening acute exacerbations
Decreasing frequency of exacerbations
Relieving symptoms
Delaying disability, particularly maintaining the patient’s ability to walk
Treatment of exacerbations and relapses
Corticosteroids, given in brief courses, are used to treat acute onset of symptoms or exacerbations that cause objective deficits sufficient to impair function (eg, loss of vision, strength, or coordination); regimens include
1, 2). Some evidence indicates that IV corticosteroids shorten acute exacerbations, slow progression, and improve MRI measures of disease.
If corticosteroids are ineffective in reducing the severity of an exacerbation, plasma exchange may be used. Plasma exchange can be used for any relapsing form of MS (relapsing-remitting, progressive relapsing, secondary progressive). It is not used for primary progressive MS.
Plasma exchange and hematopoietic stem cell transplantation may be somewhat useful for severe, intractable disease.
Disease-modifying therapies
For additional information, see Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis.
Common adverse effects of interferons include flu-like symptoms and depression (which tend to decrease over time), development of neutralizing antibodies after months of therapy, and cytopenias.
The following oral immunomodulatory medications can be used to treat relapsing forms of MS, including active secondary MS.
Because most people are averse to self-injection, oral immunomodulatory medications are being increasingly used as first-line treatments for relapsing forms of MS.
Disease-modifying therapies can be used to treat relapsing forms of MS. There is no consensus regarding choice of disease-modifying immunomodulatory therapy. Many experts recommend patient education and shared decision-making, including when disease-modifying therapies are offered to patients who have > 1 lesion (seen on imaging) and a clinically isolated syndrome. If one medication is ineffective, a different one can be tried.
progressive multifocal leukoencephalopathy (PML).
Medications that increase the risk of PML include the following (in descending order of risk):
If any of these medications are used, consultation with a neurologist with training in MS is highly recommended. Before these medications are started, blood tests should be done to check for antibodies to JC virus (JCV), which causes PML. Based on the results, the following is done:
If results are positive, patients should be counseled about the risk of PML.
If results are negative, antibody tests should be done every 6 months as long as any of these medications is used because seroconversion is common.
If test results become positive, patients should be counseled again about the risk, and clinicians should consider switching to a medication without this risk.
If the high-risk medication is continued, MRI of the brain should be done about every 6 months.
Development of PML symptoms (eg, aphasia, change in mental status, hemianopia, ataxia) requires immediate brain MRI, with and without gadolinium. MRI can often distinguish PML from MS. After MRI, a lumbar punctureplasma exchange can be done to remove the medication quickly, and if immune reconstitution inflammatory syndrome (IRIS) develops, corticosteroids are given.
Pearls & Pitfalls
7]).
9, 10). Treatments should be tailored to the patient and managed by MS specialists with expertise in their use.
If immunomodulatory medications are ineffective, monthly IV immune globulin may help.
Symptom control
Other treatments can be used to control specific symptoms:
Spasticity
Problems with gait
Painful paresthesias
Depression is treated with counseling and antidepressants.
Bladder dysfunction is treated based on its underlying mechanism.
Constipation may be treated with stool softeners or laxatives, taken regularly.
Fatigue
Tremor:11).
Supportive care
Encouragement and reassurance help patients with multiple sclerosis.
Regular exercise (eg, stationary biking, treadmill, swimming, stretching, balance exercises), with or without physical therapy, is recommended, even for patients with advanced MS, because exercise conditions the heart and muscles, reduces spasticity, prevents contractures and falls, and has psychologic benefits.
Patients should maintain as normal and active a life as possible but should avoid overwork, fatigue, and exposure to excess heat. Cigarette smoking should be stopped.
Vaccination does not appear to increase risk of exacerbations.
Debilitated patients require measures to prevent pressure ulcers and urinary tract infections; intermittent urinary self-catheterization may be necessary.
Treatment references
1. Le Page E, Veillard D, Laplaud DA, et alLancet 386 (9997):974–981, 2015. doi: 10.1016/S0140-6736(15)61137-0
2. Burton JM, O'Connor PW, Hohol M, Beyene J: Oral versus intravenous steroids for treatment of relapses in multiple sclerosis. Cochrane Database Syst Rev 12:CD006921, 2012. doi: 10.1002/14651858.CD006921.pub3
3. Freedman MS, Devonshire V, Duquette P, et al: Treatment optimization in multiple sclerosis: Canadian MS working group recommendations. Can J Neurol Sci 47 (4):437–455, 2020. doi: 10.1017/cjn.2020.66 Epub 2020 Apr 6
4. Li H, Hu F, Zhang Y, Li K: Comparative efficacy and acceptability of disease-modifying therapies in patients with relapsing–remitting multiple sclerosis: A systematic review and network meta-analysis. J Neurol 267(12):3489-3498, 2020. doi: 10.1007/s00415-019-09395-w Epub 2019 May 25
5. Rae-Grant A, Day GS, Ruth Ann Marrie RA, et al: Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 90 (17):777–788, 2018. doi: 10.1212/WNL.0000000000005347
6. Hauser SL, Bar-Or A, Comi G, et alN Engl J Med 376 (3):221–234, 2017. doi: 10.1056/NEJMoa1601277
7. Hauser SL, Bar-Or A, Cohen JA, et alN Engl J Med 383 (6):546–557, 2020. doi: 10.1056/NEJMoa1917246
8. Granqvist M, Boremalm M , Poorghobad A, et alJAMA Neurol 75 (3):320–327, 2018. doi: 10.1001/jamaneurol.2017.4011
9. Casanova B, Quintanilla-Bordás C, Gascón F: Escalation vs. early intense therapy in multiple sclerosis. J Pers Med 12 (1):119, 2022. doi: 10.3390/jpm12010119
10. Simonsen CS, Flemmen HO, Broch, L, et al: Early high efficacy treatment in multiple sclerosis is the best predictor of future disease activity over 1 and 2 years in a Norwegian population-based registry. Front Neurol 12:693017, 2021. doi: 10.3389/fneur.2021.693017
11. Makhoul K, Ahdab R, Riachi N, et al: Tremor in multiple sclerosis-An overview and future perspectives. Brain Sci 10 (10):722, 2020. doi: 10.3390/brainsci10100722
12. Multiple Sclerosis Society of CanadaPublic Health Nutr (23) 7: 1278–1279, 2020.
Prognosis for Multiple Sclerosis
The course of multiple sclerosis is highly varied and unpredictable. In most patients, especially when MS begins with optic neuritis, remissions can last months to > 10 years.
Most patients (60 to 80% [1]) who initially have a clinically isolated syndrome eventually develop MS, with a second lesion becoming evident or MRI detecting a lesion, usually within 5 years after the initial symptoms begin. Treatment with disease-modifying therapies can delay this progression. If patients have a radiologically isolated syndrome without a history of a clinical episode consistent with demyelination, the risk of developing MS is 19 to 90%, depending on the patient's age and the presence of spinal cord or gadolinium-enhancing lesions (2).
If the initial brain or spinal MRI shows more extensive disease, patients may be at risk of earlier disability, as may patients who have motor, bowel, and/or bladder symptoms when they present or who have incomplete recovery during relapses. Some patients, such as men with onset in middle age and with frequent exacerbations, can become rapidly incapacitated. Cigarette smoking may accelerate disease progression.
Life span is shortened only in very severe cases.
Prognosis references
1. National Multiple Sclerosis Society: Clinically isolated syndrome (CIS). Accessed 5/1/23.
2. Lebrun-Frénay C, Rollot F, Mondot L, et al: Risk factors and time to clinical symptoms of multiple sclerosis among patients with radiologically isolated syndrome. JAMA Netw Open 4 (10):e2128271, 2021. doi: 10.1001/jamanetworkopen.2021.28271
Key Points
Multiple sclerosis involves demyelination of the CNS; MS may progress unpredictably but has several typical patterns of progression.
The most common symptoms are paresthesias, weakness or clumsiness, and visual symptoms, but a wide variety of symptoms are possible.
MS is confirmed if MRI and clinical findings establish characteristic lesions that are separate in time and space; however, progression to MS is likely if patients have even a single characteristic clinical deficit or possibly a single radiologic lesion.
Treat patients with corticosteroids (for severe exacerbations) and immunomodulatory medications (to delay or prevent exacerbations).
Treat patients supportively, using medications to treat symptoms (eg, spasticity, painful paresthesias, depression, bladder dysfunction, fatigue, gait problems) when warranted.






