


The peripheral nervous system refers to parts of the nervous system outside the brain and spinal cord. It includes the cranial nerves and spinal nerves from their origin to their end. The anterior horn cells, although technically part of the central nervous system (CNS), are sometimes discussed with the peripheral nervous system because they are part of the motor unit.
Motor neuron dysfunction results in muscle weakness or paralysis. Sensory neuron dysfunction results in abnormal or lost sensation. Some disorders are progressive and fatal.
Anatomy of Peripheral Nerves
A motor unit consists of
An anterior horn cell
Its motor axon
The muscle fibers it innervates
The connection between them (neuromuscular junction)
The anterior horn cells are located in the gray matter of the spinal cord and thus are technically part of the CNS. In contrast to the motor system, the cell bodies of the afferent sensory fibers lie outside the spinal cord, in dorsal root ganglia.
Nerve fibers outside the spinal cord join to form anterior (ventral) motor nerve roots and posterior (dorsal) sensory nerve roots. The ventral and dorsal roots combine to form a spinal nerve. Thirty of the 31 pairs of spinal nerves have dorsal and ventral roots; C1 has no sensory root (see figure Spinal Nerve).
Spinal Nerve

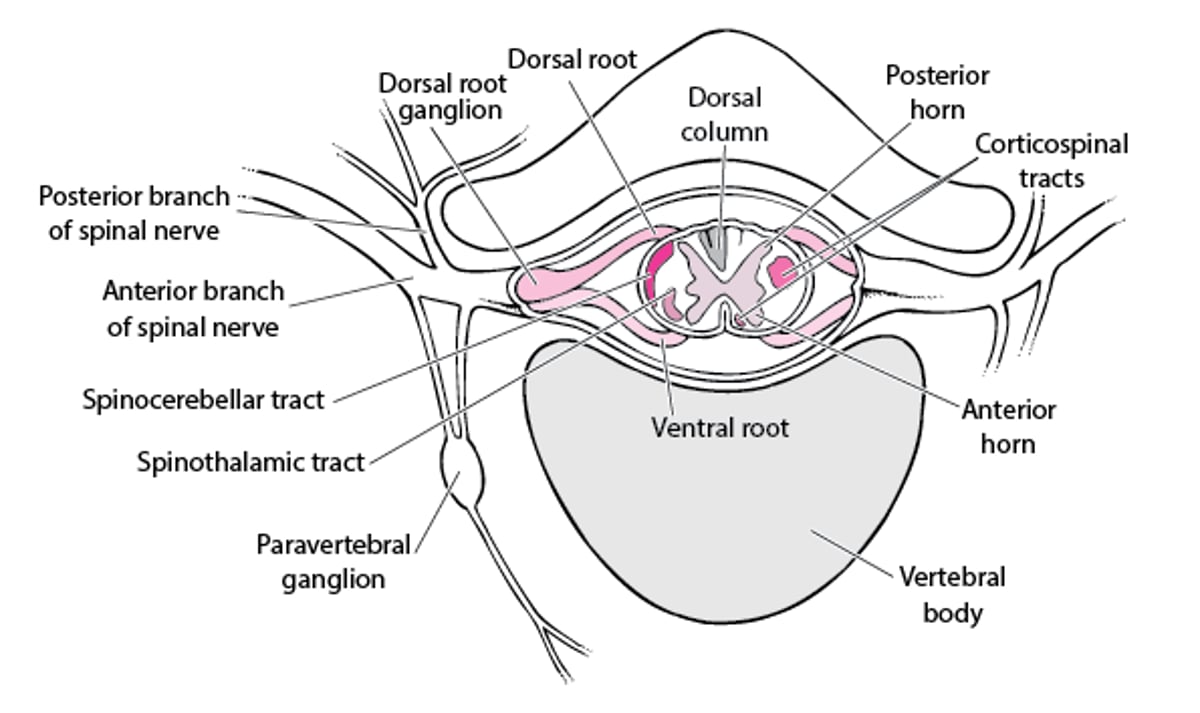
The spinal nerves exit the vertebral column via an intervertebral foramen. Because the spinal cord is shorter than the vertebral column, the more caudal the spinal nerve, the further the foramen is from the corresponding cord segment. Thus, in the lumbosacral region, nerve roots from lower cord segments descend within the spinal column in a near-vertical sheaf, forming the cauda equina. Just beyond the intervertebral foramen, spinal nerves branch into several parts.
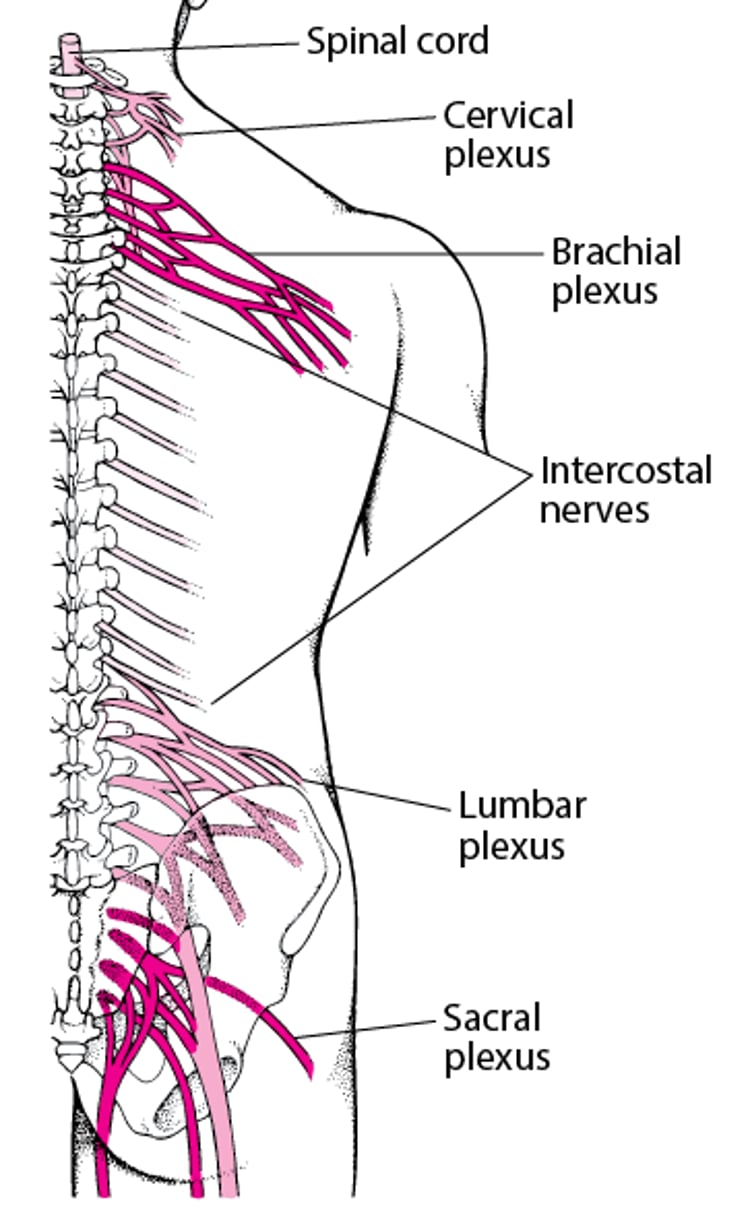
Branches of the cervical and lumbosacral spinal nerves anastomose peripherally into plexuses, then branch into nerve trunks that terminate up to 1 m away in peripheral structures (see figure Plexuses). The intercostal nerves are segmental.
Plexuses

The term peripheral nerve refers to the part of a spinal nerve distal to the root and plexus. Peripheral nerves are bundles of nerve fibers, which range in diameter from 0.2 to 18 mcm. Schwann cells form a thin cytoplasmic tube around each fiber and further wrap larger fibers in a multilayered insulating membrane (myelin sheath).
Physiology of Peripheral Nerves
The myelin sheath enhances impulse conduction. The largest and most heavily myelinated fibers conduct quickly; they convey motor, touch, and proprioceptive impulses. The less myelinated and unmyelinated fibers conduct more slowly; they convey pain, temperature, and autonomic impulses.
Because nerves are metabolically active tissues, they require nutrients, supplied by blood vessels called the vasa nervorum.
Etiology of Peripheral Nerve Disorders
Peripheral nerve disorders can result from damage to or dysfunction of the one of the following:
Cell body
Myelin sheath
Axons
Neuromuscular junction
Disorders can be genetic or acquired (due to toxic, metabolic, traumatic, infectious, or inflammatory conditions—see table Some Causes of Peripheral Nervous System Disorders).
Peripheral neuropathies may affect
One nerve (mononeuropathy)
Several discrete nerves (multiple mononeuropathy, or mononeuritis multiplex)
Multiple nerves diffusely (polyneuropathy)
A plexus (plexopathy)
A nerve root (radiculopathy)
More than one site can be affected; eg, in the most common variant of Guillain-Barré syndrome, multiple segments of cranial nerves, usually the 2 facial nerves, may be affected.
Pathophysiology of Peripheral Nerve Disorders
Because sensory and motor cell bodies are in different locations, a nerve cell body disorder typically affects either the sensory or motor component but rarely both.
Damage
Damage to the myelin sheath (demyelination) slows nerve conduction. Demyelination affects mainly heavily myelinated fibers, causing large-fiber sensory dysfunction (buzzing and tingling sensations), motor weakness, and diminished reflexes. The hallmark of acquired demyelinating polyneuropathy is severe motor weakness with minimal atrophy.
Because the vasa nervorum are furthest from the center of a nerve, centrally located fascicles are most vulnerable to vascular disorders (eg, vasculitis, ischemia). These disorders result in small-fiber sensory dysfunction (sharp pain and burning sensations, decreased temperature sensation), motor weakness proportional to atrophy, and less severe reflex abnormalities than in other nerve disorders. The distal two thirds of a limb is affected most. Initially, deficits tend to be asymmetric because the vasculitic or ischemic process is random. However, multiple infarcts may later coalesce, causing symmetric deficits (polyneuropathy).
Toxic-metabolic or genetic disorders usually begin symmetrically. Immune-mediated processes may be symmetric or, early in rapidly evolving processes, asymmetric.
Damage to the axon transport system for cellular constituents, especially microtubules and microfilaments, causes significant axon dysfunction. First affected are the smaller fibers (because they have greater metabolic requirements) at the most distal part of the nerve. Then, axonal degeneration slowly ascends, producing the characteristic distal-to-proximal pattern of symptoms (stocking-glove sensory loss, followed by weakness).
Recovery
Damage to the myelin sheath (eg, by injury or Guillain-Barré syndrome) can often be repaired by surviving Schwann cells in about 6 to 12 weeks.
After axonal damage, the fiber regrows within the Schwann cell tube at about 1 mm/day once the pathologic process ends. However, regrowth may be misdirected, causing aberrant innervation (eg, of fibers in the wrong muscle, of a touch receptor at the wrong site, or of a temperature instead of a touch receptor).
Regeneration is impossible when the cell body dies and is unlikely when the axon is completely lost.
Evaluation of Peripheral Nerve Disorders
Deficits defined by history and examination
Attention to clinical clues to peripheral nervous system disorders
Usually nerve conduction studies and electromyography
Sometimes nerve or skin punch biopsy
Genetic testing (for hereditary neuropathies)
Clinical evaluation
History should focus on type of symptom, onset, progression, and location, as well as information about potential causes (eg, family history, toxic exposures, past medical disorders).
Physical and neurologic examination should further define the type of deficit (eg, motor deficit, type of sensory deficit, combination). The following are evaluated:
Sensation (using pinprick and temperature for small fibers; using vibration and proprioception tests for large fibers)
Motor strength (noting whether motor weakness is proportional to the degree of atrophy)
Deep tendon reflexes (noting type and distribution of reflex abnormalities)
Central and peripheral nerve function
Physicians should suspect a peripheral nervous system disorder based on the pattern and type of neurologic deficits, especially if deficits are localized to particular nerve roots, spinal nerves, plexuses, specific peripheral nerves, or a combination. These disorders are also suspected in patients with mixed sensory and motor deficits, with multiple foci, or with a focus that is incompatible with a single anatomic site in the CNS.
Physicians should also suspect peripheral nervous system disorders in patients with generalized or diffuse weakness but no sensory deficits; in these cases, peripheral nervous system disorders may be overlooked because they are not the most likely cause of such symptoms.
Clues that a peripheral nervous system disorder may be the cause of generalized weakness include the following:
Patterns of generalized weakness that suggest a specific cause (eg, predominant ptosis and diplopia, which suggest early myasthenia gravis)
Symptoms and signs other than weakness that suggest a specific disorder or group of disorders (eg, cholinergic effects, which suggest organophosphate poisoning)
Deficits in a stocking-glove distribution, which suggest diffuse axonal disorders or polyneuropathy
Fasciculations
Hypotonia
Muscle wasting without hyperreflexia
Weakness that is progressive, chronic, and unexplained
Clues that the cause may not be a peripheral nervous system disorder include
Hyperreflexia
Hypertonia
Clonus
Extensor plantar response (eg, Babinski sign)
These deficits suggest an upper motor neuron disorder as the cause of weakness. Hyporeflexia is consistent with peripheral nervous system deficits but is nonspecific. For example, acute cervical transverse myelitis can mimic Guillain-Barré syndrome, particularly in patients with preexisting neuropathy.
Although many exceptions are possible, certain clinical clues may also suggest possible causes of peripheral nervous system deficits (see table Clinical Clues to Causes of Peripheral Nervous System Disorders).
Clinical assessment narrows diagnostic possibilities and guides further testing.
Testing
Usually, nerve conduction studies and electromyography (collectively called electrodiagnostic testing) are done. These tests help do the following:
Differentiate peripheral nervous system disorders from neuromuscular junction and muscle disorders
Localize site of peripheral nervous system dysfunction (eg, root, plexus, peripheral nerve)
Distinguish demyelinating disorders (very slow conduction) from axonal disorders
Patients with weakness but no sensory deficits can be evaluated with electrodiagnostic testing.
Other testing, such as imaging, depends on whether a CNS lesion must be ruled out (eg, MRI if all limbs are affected, to rule out cervical spinal cord compression).
Nerve biopsy is occasionally done to help differentiate demyelinating from vasculitic large-fiber neuropathies. If vasculitis is a consideration, the biopsy specimen should include skin and muscle to increase the likelihood of a definitive diagnosis. If a small-fiber neuropathy is suspected, skin punch biopsy can be done; loss of nerve endings and sweat glands supports that diagnosis.
Pearls & Pitfalls
|
Genetic testing is indicated if a hereditary neuropathy is suspected.
Treatment of Peripheral Nerve Disorders
Treatment of underlying disorder
Supportive care, often by a multidisciplinary team
Treatment of a peripheral nerve disorder is directed at the underlying disorder when possible. Otherwise, treatment is supportive. A multidisciplinary team approach helps patients cope with progressive neurologic disability:
Physical therapists may help patients maintain muscle function.
Occupational therapists can recommend adaptive braces and walking devices to help with activities of daily living.
Speech and language therapists may provide alternative communication devices.
If pharyngeal weakness develops, a speech therapist or a multidisciplinary team that specializes in swallowing problems can help assess risk of aspiration and recommend measures for prevention (eg, precautions for oral feeding and/or need for tube feedings).
A gastroenterologist may recommend percutaneous endoscopic gastrostomy.
If respiratory weakness develops, forced vital capacity is measured, and pulmonary or intensive care specialists help assess whether intensive care, noninvasive respiratory support (eg, bilevel positive airway pressure), and tracheostomy with full ventilatory support are needed.
Early in fatal disorders, health care professionals must talk frankly with patients, family members, and caregivers to determine the level of intervention acceptable. Patients are encouraged to put their decisions in writing (advance directives) before they become incapacitated. These decisions should be reviewed and confirmed at various stages of the disorder.
Key Points
Peripheral nervous system disorders are often suspected based on clinical findings (eg, stocking-glove distribution, hyporeflexia, distal muscle weakness and wasting, localization to a peripheral nerve distribution).
If patients have profound motor weakness with minimal atrophy and areflexia, consider acquired demyelinating polyneuropathy.
If patients have abnormal pain and temperature sensation and atrophy in proportion to weakness (sometimes with disproportionate preservation of reflexes), consider a vasculitic or ischemic neuropathy.
If patients have chronic progressive muscle weakness, fasciculations, muscle atrophy, and no sensory deficits, consider motor neuron disease.
Nerve conduction studies and electromyography help identify level of involvement (root, plexus, peripheral nerve, neuromuscular junction, muscle fiber) and help distinguish demyelinating from axonal disorders.






