


Infants whose weight is the 10th percentile for gestational age are classified as small for gestational age. Complications include perinatal asphyxia, meconium aspiration, polycythemia, and hypoglycemia.
Gestational age is loosely defined as the number of weeks between the first day of the mother's last normal menstrual period and the day of delivery. More accurately, the gestational age is the difference between 14 days before the date of conception and the date of delivery. Gestational age is not the actual embryologic age of the fetus, but it is the universal standard among obstetricians and neonatologists for discussing fetal maturation.
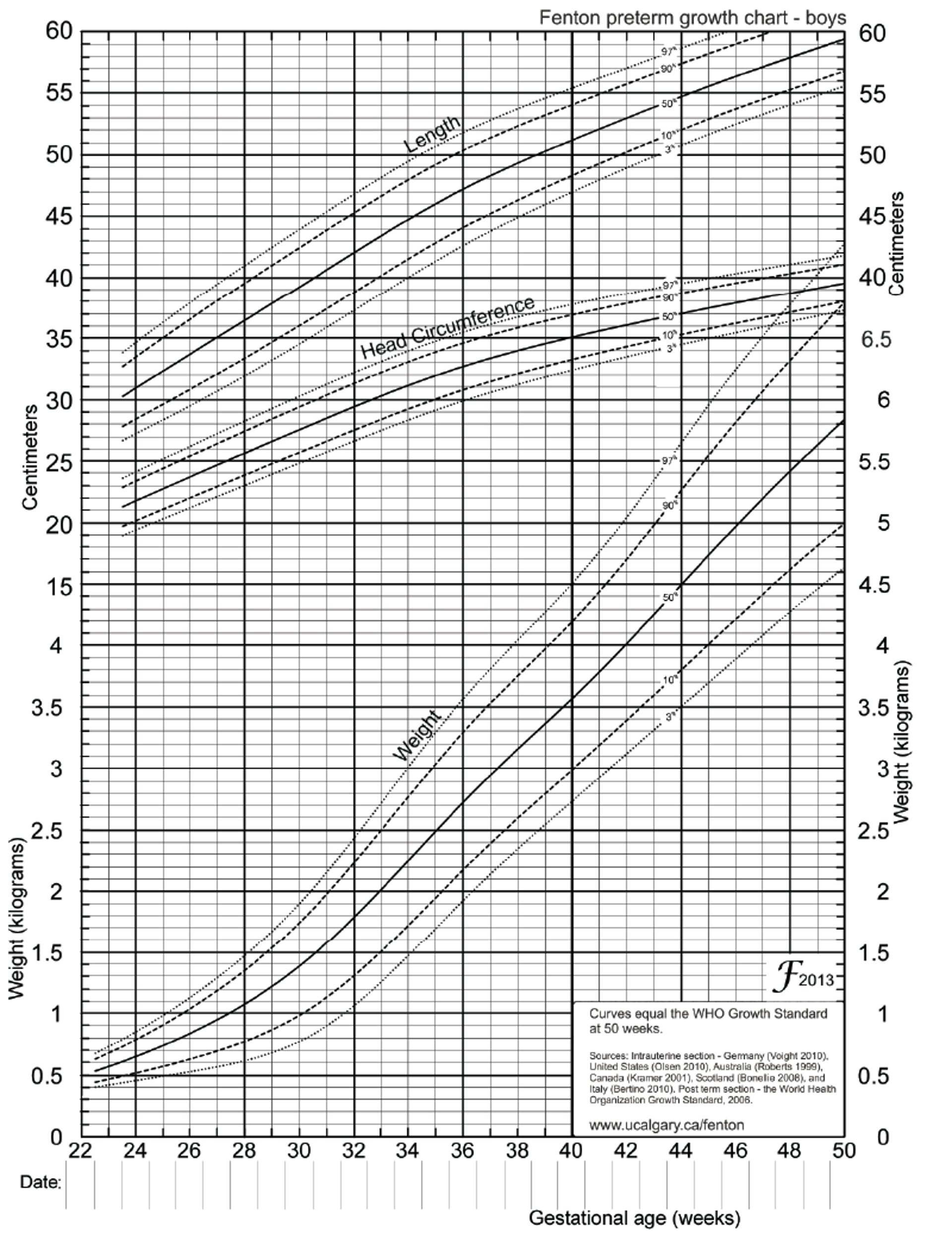
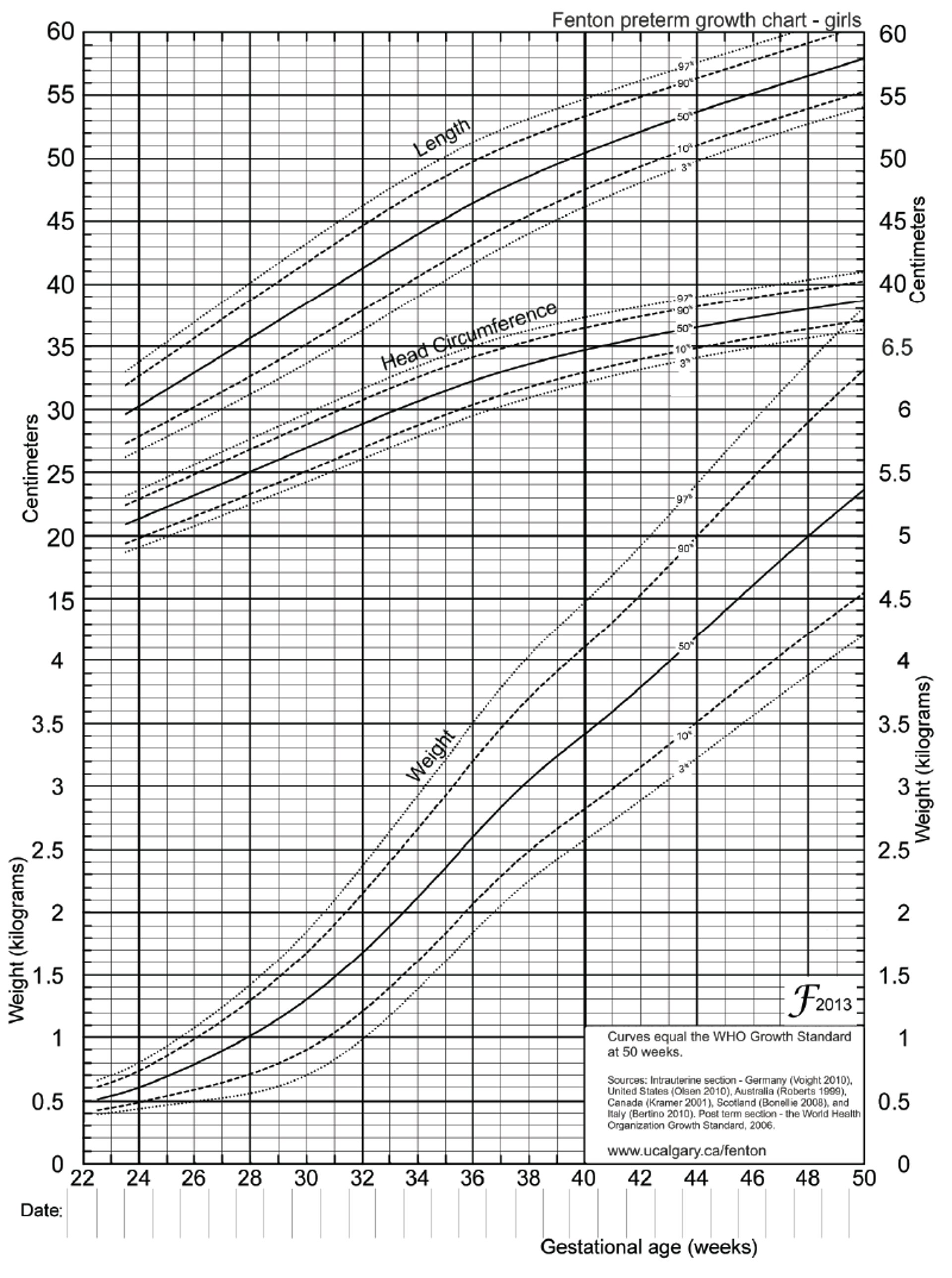
The Fenton growth charts provide a more precise assessment of growth vs gestational age; there are separate charts for boys and girls.
Fenton Growth Chart for Preterm Boys
Fenton T, Kim J: A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatrics 13:59, 2013. doi: 10.1186/1471-2431-13-59; used with permission. Available at www.biomedcentral.com. |

Fenton Growth Chart for Preterm Girls
Fenton T, Kim J: A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatrics 13:59, 2013. doi: 10.1186/1471-2431-13-59; used with permission. Available at www.biomedcentral.com. |

Etiology of SGA Infant
Causes may be divided into those in which the growth restriction is
Symmetric: Height, weight, and head circumference are about equally affected.
Asymmetric: Weight is most affected, with a relative sparing of growth of the brain, cranium, and long bones.
Symmetric growth restriction usually results from a fetal problem that begins early in gestation, often during the first trimester. When the cause begins relatively early in gestation, the entire body is affected, resulting in fewer cells of all types. Common causes include
Genetic disorders
First-trimester congenital infections (eg, with cytomegalovirus, rubella virus, or Toxoplasma gondii)
Asymmetric growth restriction usually results from placental or maternal problems that typically manifest in the late second or the third trimester. When the cause begins relatively late in gestation, organs and tissues are not equally affected, resulting in asymmetric growth restriction. Common causes include
Placental insufficiency resulting from maternal disease involving the small blood vessels (eg, preeclampsia, hypertension, renal disease, antiphospholipid antibody syndrome, long-standing diabetes)
Relative placental insufficiency caused by multiple gestation
Placental involution accompanying postmaturity
Chronic maternal hypoxemia caused by pulmonary or cardiac disease
Maternal malnutrition
Conception using assisted reproductive technology
Social and Illicit Drugs During Pregnancy).
Many SGA infants are healthy but just constitutionally small, and not all infants whose growth was restricted in utero are SGA (ie, weight is < the 10th percentile for gestational age).
Symptoms and Signs of SGA Infant
Despite their size, SGA infants have physical characteristics (eg, skin appearance, ear cartilage, sole creases) and behavior (eg, alertness, spontaneous activity, zest for feeding) similar to those of normal-sized infants of like gestational age. However, they may appear thin with decreased muscle mass and subcutaneous fat tissue. Facial features may appear sunken, resembling those of an elderly person ("wizened facies"). The umbilical cord can appear thin and small.
Complications
Full-term SGA infants do not have the complications related to organ system immaturity that preterm infants of similar size have. They are, however, at risk of
Perinatal asphyxia
Meconium aspiration
Perinatal asphyxia during labor is the most serious potential complication. It is a risk if intrauterine growth restriction is caused by placental insufficiency (with marginally adequate placental perfusion) because each uterine contraction slows or stops maternal placental perfusion by compressing the spiral arteries. Therefore, when placental insufficiency is suspected, the fetus should be assessed before labor and the fetal heart rate should be monitored during labor. If fetal compromise is detected, rapid delivery, often by cesarean delivery, is indicated.
Meconium aspiration may occur during perinatal asphyxia. SGA infants, especially those who are postterm, may pass meconium into the amniotic sac and begin deep gasping movements. The consequent aspiration may result in meconium aspiration syndrome. Meconium aspiration syndrome is often most severe in growth-restricted or postterm infants, because the meconium is contained in a smaller volume of amniotic fluid and thus more concentrated.
Hypoglycemia often occurs in the early hours and days of life because of a lack of adequate glycogen synthesis and thus decreased glycogen stores and must be treated quickly with IV glucose.
Polycythemia may occur when SGA fetuses experience chronic mild hypoxia caused by placental insufficiency. Erythropoietin release is increased, leading to an increased rate of erythrocyte production. The neonate with polycythemia at birth appears ruddy and may be tachypneic or lethargic.
Hypothermia may occur because of impaired thermoregulation, which involves multiple factors including increased heat loss due to the decrease in subcutaneous fat, decreased heat production due to intrauterine stress and depletion of nutrient stores, and increased surface to volume ratio because of small size. SGA infants should be in a thermoneutral environment to minimize oxygen consumption.
Treatment of SGA Infant
Supportive care
Underlying conditions and complications are treated.
There is no specific intervention for the SGA state, but prevention is aided by prenatal advice on the importance of avoiding alcohol, tobacco, and illicit drugs.
Prognosis for SGA Infant
If asphyxia can be avoided, neurologic prognosis for term SGA infants is quite good. However, later in life there is probably increased risk of ischemic heart disease, hypertension, and stroke, which are thought to be caused by abnormal vascular development.
If intrauterine growth restriction is caused by chronic placental insufficiency, adequate nutrition may allow SGA infants to demonstrate remarkable “catch-up” growth after delivery.
Infants who are SGA because of genetic factors, congenital infection, or maternal substance use often have a worse prognosis, depending on the specific diagnosis.
Key Points
Infants whose weight is < the 10th percentile for gestational age are small for gestational age (SGA).
Disorders early in gestation cause symmetric growth restriction, in which height, weight, and head circumference are about equally affected.
Disorders late in gestation cause asymmetric growth restriction, in which weight is most affected, with relatively normal growth of the brain, cranium, and long bones.
Although small, SGA infants do not have the complications related to organ system immaturity that preterm infants of similar size have.
Complications are mainly those of the underlying cause but generally also include perinatal asphyxia, meconium aspiration, hypoglycemia, polycythemia, and hypothermia.






