


Noncancerous bone tumors are benign, which means they are not cancer and in general never or rarely spread to other areas of the body. However, they can cause problems because they may weaken bones, interfere with joint movement, or destroy nearby healthy tissue.
Benign tumors may be painless, but often they cause bone pain. The pain can be severe. Pain may occur when at rest or at night and tends to progressively worsen.
(See also Overview of Bone Tumors.)
Chondroblastomas
Chondroblastomas are rare tumors that grow in the ends of bones. They usually occur in people aged 10 to 20 years. These tumors may cause pain.
To diagnose a chondroblastoma, doctors take x-rays and may do other imaging tests, such as magnetic resonance imaging (MRI). Doctors also remove a tissue sample for examination under a microscope (biopsy).

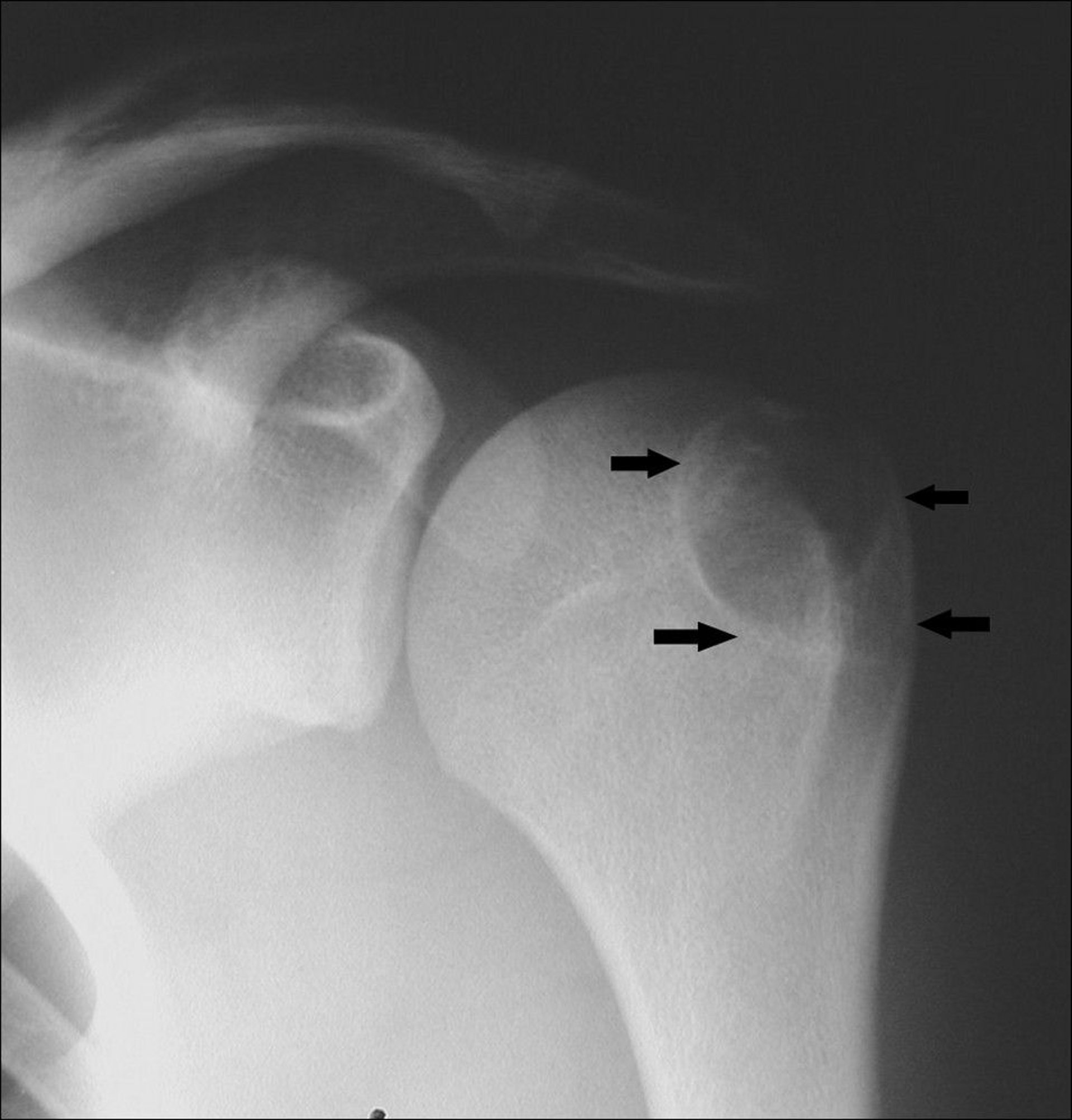
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
If untreated, these tumors may continue to grow and destroy bone and the joint. Therefore, treatment consists of surgical removal and use of a bone graft (transplantation of bone tissue from one bone to another) to fill in the defect. Graft material can be bone removed from the person’s own pelvis (autograft), processed bone tissue from another person (allograft), or a synthetic bone substitute. Occasionally, these tumors return after surgery.
Chondromyxofibromas
Chondromyxofibromas are very rare tumors that usually occur in people younger than 30. They are usually located off to one side near the ends of the bones in the extremities (the limbs). Pain is the usual symptom.
To diagnose chondromyxofibromas, doctors take x-rays and do MRI). To confirm the diagnosis, doctors also do a biopsy.


Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Treatment of chondromyxofibromas consists of surgical removal, which usually provides a cure. However, these tumors sometimes return.
Enchondromas
Enchondromas may occur at any age but tend to develop in people aged 10 to 40 years. These tumors develop in the central part of a bone (the marrow cavity) in long bones.
These tumors usually do not cause symptoms, but some may grow larger and cause pain.
The tumors often are discovered when x-rays are taken for other reasons, and doctors often can diagnose them by their appearance on the x-ray.
If the tumor cannot be identified with certainty on x-rays or if it causes pain, removal of a tissue sample for examination under a microscope (biopsy) may be needed to confirm the diagnosis of enchondroma and rule out the possibility of a cancerous tumor.
If an enchondroma does not cause pain and if repeated x-rays show no enlargement, it does not have to be removed or treated.
Enchondromas may change into a cancerous (malignant) bone tumor called a chondrosarcoma. This change is rare in people who have only a single enchondroma, but in people who have multiple enchondromas (called enchondromatosis), the change to a cancerous tumor is more common.

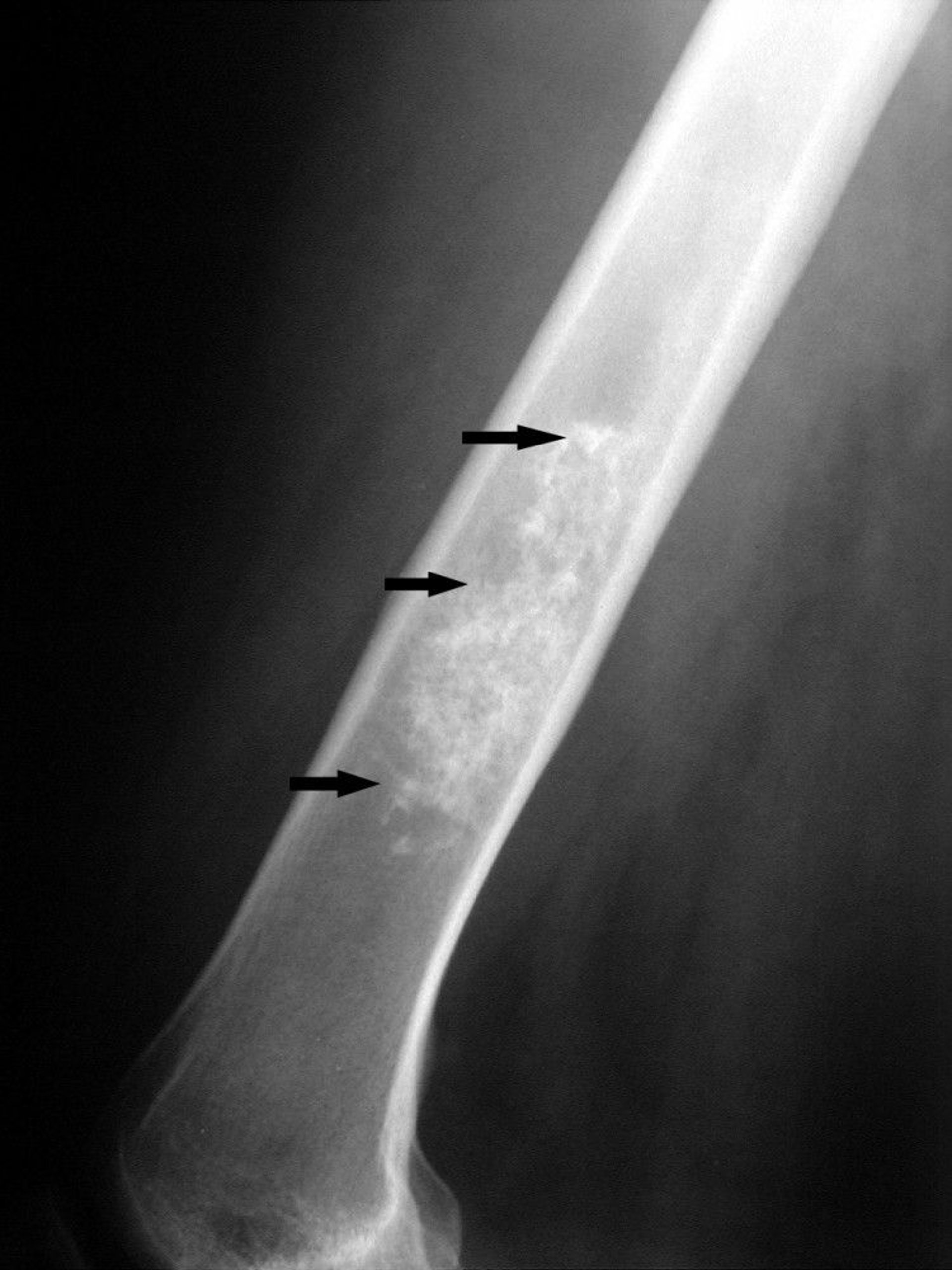
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Follow-up x-rays may be taken to monitor any changes in size and make sure the tumor has not become a chondrosarcoma.
Fibrous dysplasia
Fibrous dysplasia is abnormal bone development that occurs during childhood. It may affect one bone or several bones. The bones of the pelvis or hip are most frequently affected.
Children may have birth marks and signs of early puberty, which indicate a disorder called Albright syndrome (or McCune-Albright syndrome). The abnormal bone growths commonly stop developing at puberty. This condition rarely becomes cancerous (malignant).
This disorder is often found when x-rays are done for other reasons. If the x-ray results are not clear, doctors do a biopsy.
Benign giant cell tumors
Benign (noncancerous) giant cell tumors (GCT) usually occur in people in their 20s and 30s. These tumors most commonly start in the ends of bones and may extend into nearby tissue. They may cause pain.
To diagnose benign giant cell tumors, doctors first take x-rays. Because these tumors rarely spread (metastasize) to the lungs, doctors may do computed tomography (CT) of the chest. Doctors also do a biopsy to be sure that the tumor is benign.
Nonossifying fibroma (fibrous cortical defect, fibroxanthoma)
A nonossifying fibroma is an abnormality that results when part of a bone does not harden normally and instead is filled with fibrous tissue rather than bone tissue. A very small nonossifying fibroma is called a fibrous cortical defect. Nonossifying fibromas are common among children. They commonly occur close to the ends of the bones of the legs.
Most nonossifying fibromas eventually harden, sometimes more than normal bone. Small nonossifying fibromas do not cause symptoms. However, some small fibromas grow larger and may cause pain and increase the risk of a break (fracture).
Nonossifying fibromas are most often found when an x-ray is taken for another reason.


Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Small nonossifying fibromas require no treatment. However, fibromas that cause pain or have grown large are removed and a bone graft is done to fill in the defect.
Osteoblastomas
Osteoblastomas are rare noncancerous tumors. Some doctors simply consider them to be large osteoid osteomas. Osteoblastomas are much more common among males and typically develop between ages 10 and 35. These tumors develop in the bones of the spine, legs, hands, and feet. They grow slowly and destroy normal bone and are painful.
To diagnose osteoblastomas, doctors take x-rays and do other imaging tests such as computed tomography (CT) and magnetic resonance imaging (MRI). To confirm the diagnosis of osteoblastoma, doctors remove a tissue sample for examination under a microscope (biopsy).
Treatment of osteoblastomas requires surgery. Often the tumors are removed and then bone grafting (transplantation of bone tissue from one bone to another) is done to fill in the defect. Sometimes the tumors return after surgery but do not spread (metastasize) to other parts of the body.
Osteochondromas
Osteochondromas (osteocartilaginous exostoses), the most common type of noncancerous bone tumors, usually develop in people aged 10 to 20 years. These tumors are growths on the surface of a bone, which stick out as hard lumps. A person may have one or several tumors. The tendency to develop several tumors can run in families.
At some point in their lives, about 10% of people who have more than one osteochondroma (called multiple osteochondromatosis) may develop a cancerous (malignant) bone tumor called a chondrosarcoma (presumably formed from an existing osteochondroma). People with multiple osteochondromatosis should visit their doctor for regular examinations. However, people who have only one osteochondroma are unlikely to develop a chondrosarcoma. Therefore, a single osteochondroma usually does not need to be removed unless it causes symptoms.
Doctors do x-rays to see the growths on the surface of the bone. Most osteochondromas are diagnosed by x-rays. Imaging tests, such as magnetic resonance imaging (MRI) or occasionally computed tomography (CT), are also done, especially if x-ray findings are unclear.

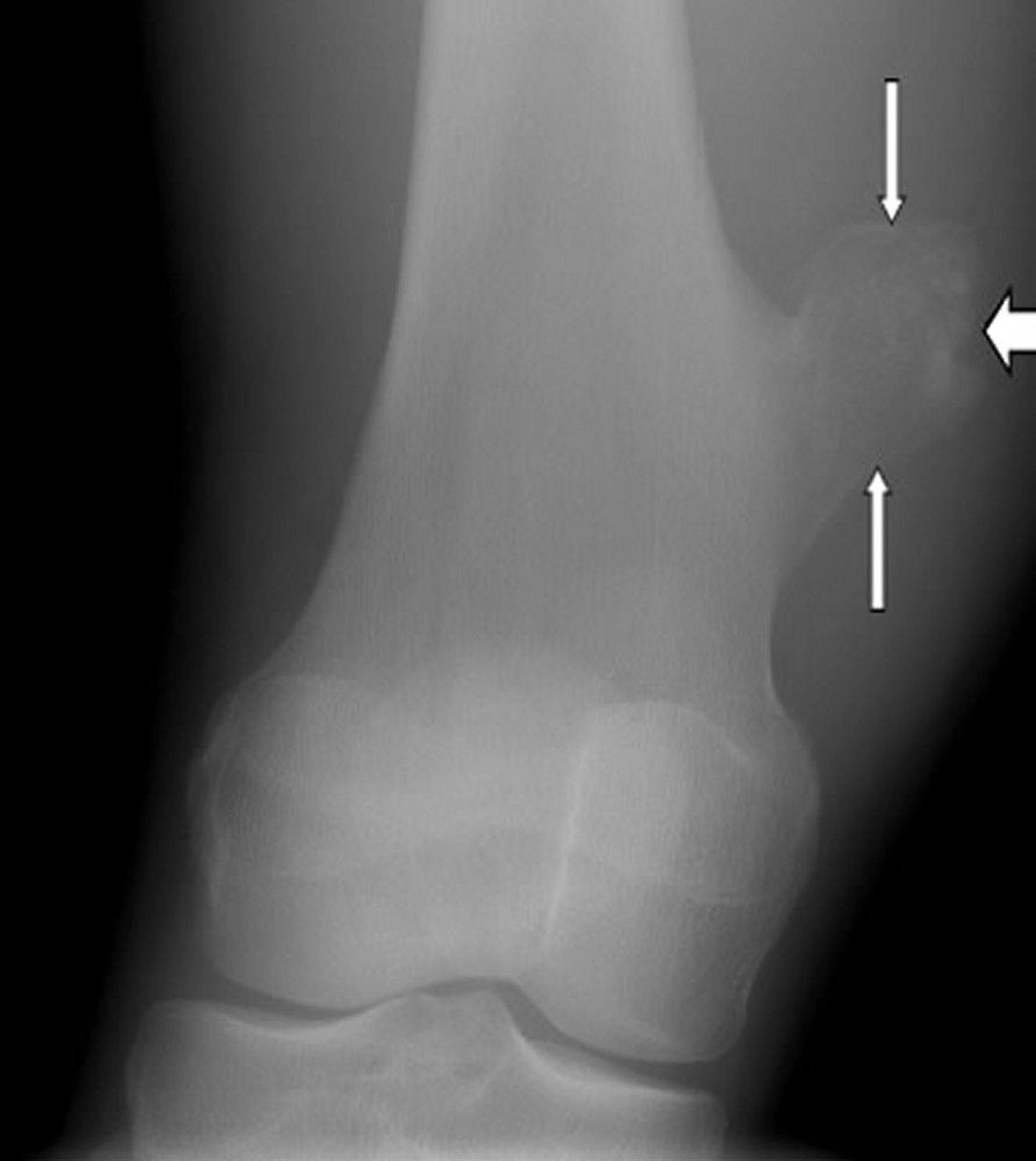
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Surgical removal of an osteochondroma is typically done if it grows larger or causes new symptoms. For example, if the tumor disturbs growth of the bone, causes pain, or presses on nearby nerves, muscles, blood vessels, or surrounding structures, it should be removed.
Osteoid osteomas
Osteoid osteomas are very small tumors that commonly develop in people aged 10 to 35. They are most common in the long bones of the legs (the thighbones and shinbones) but can occur in any bone.
To diagnose osteoid osteomas, doctors take x-rays. Bone scans using radioactive tracers are also done to help determine the exact location of the tumor. Sometimes the tumor is difficult to locate, and additional tests, such as computed tomography (CT) or magnetic resonance imaging (MRI), may be needed. If the results of the imaging tests are unclear, doctors remove a tissue sample for examination under a microscope (biopsy). The biopsy can sometimes be done when the tumor is treated.
To treat the tumor permanently, usually a doctor punctures the skin and inserts a needle-like probe into the tumor, using computed tomography as guidance for placement. A radiofrequency pulse, which heats the needle-like probe, is then applied to destroy the tumor. While this is done, the person is under general, spinal, or nerve block anesthesia. The prognosis is good, and pain should go away. Surgically removing the tumor is another way to eliminate the pain permanently. Alternatively, some people prefer to take pain relievers (analgesics) indefinitely rather than undergo a procedure. The pain may eventually go away without treatment.






