


Retinopathy of prematurity is a disorder of premature infants in which the small blood vessels in the back of the eye (retina) grow abnormally.
Retinopathy of prematurity is strongly associated with premature birth, with most cases occurring in infants who are born before 30 weeks of development in the uterus.
In the most severe cases, the rapid abnormal growth of the small blood vessels can lead to detachment of the retina and loss of vision.
Because affected newborns have no symptoms, diagnosis depends on a careful examination by an eye specialist (ophthalmologist).
This disorder is usually mild and resolves without treatment, but the eyes need to be monitored by an ophthalmologist until blood vessel growth is mature.
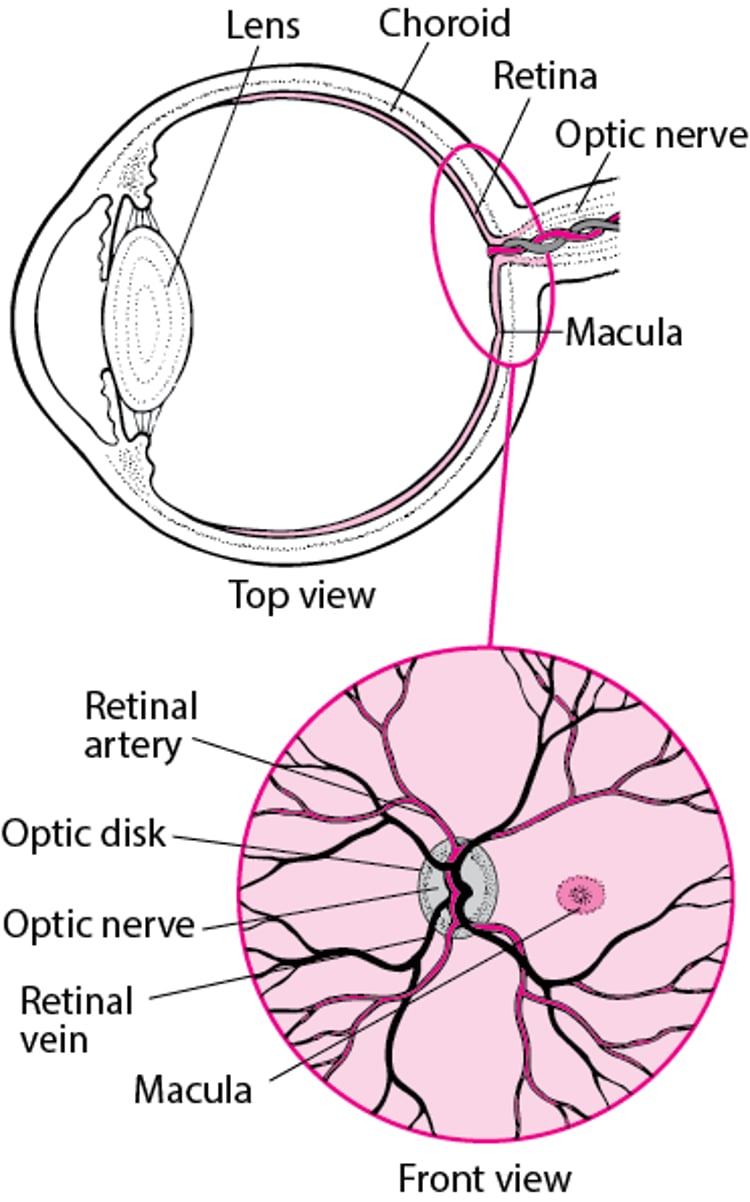
The retina is the transparent, light-sensitive structure at the back of the eye. The blood vessels in the retina start growing in a fetus at about 18 to 20 weeks of development in the uterus and continue growing until the fetus is full term. When infants are born very prematurely, the blood vessels supplying the retina may stop growing for a time. When growth resumes, it occurs in a disorganized fashion. During disorganized rapid growth, the small blood vessels may bleed. In the most severe cases, this process may ultimately result in detachment of the retina from the back of the eye and severe loss of vision.
Viewing the Retina

Premature infants are at increased risk of retinopathy of prematurity if they have serious disorders, such as infections, bleeding in the brain, or lung disorders (such as bronchopulmonary dysplasia), or had a low birth weight. Premature infants who receive oxygen for a long time (for example, because their lungs are immature) are also at increased risk.
Diagnosis of Retinopathy of Prematurity
Eye examinations
Retinopathy of prematurity does not cause symptoms, so diagnosis depends on careful examination of the back of the eyes by an ophthalmologist (a medical doctor who specializes in the evaluation and treatment of all types of eye disorders). Routinely, therefore, an ophthalmologist examines the eyes of all premature newborns who weigh less than 3 pounds (about 1,500 grams) at birth or who were in the uterus for less then 30 weeks. Eye examinations are repeated every 1 to 3 weeks as needed, until growth of the blood vessels in the retina is complete.
Newborns with severe retinopathy must have eye examinations, at least yearly, for the rest of their life. If detected early, detachment of the retina can be treated with surgery in an attempt to avoid loss of vision in the affected eye.
Treatment of Retinopathy of Prematurity
Laser photocoagulation
Bevacizumab
For very severe retinopathy of prematurity, laser photocoagulation treatment is done on the outermost portions of the retina. In this treatment, a laser beam is used to stop the abnormal growth of blood vessels and decrease the risk of detachment of the retina and loss of vision.
If retinopathy of prematurity leads to a partial or complete detachment of the retina, sometimes surgery is done to reattach the retina and prevent further vision loss.
Prognosis for Retinopathy of Prematurity
Retinopathy of prematurity is usually mild and resolves spontaneously. However, in a small percentage of affected infants weighing less than 2 pounds (about 1 kilogram) at birth, the disorder is severe and progresses to cause detachment of the retina and vision loss within 2 to 12 months after delivery.
Children whose retinopathy of prematurity has healed are at greater risk of developing other eye problems such as nearsightedness (myopia), strabismus, and amblyopia. A few children with moderate, healed retinopathy of prematurity are left with scars on the retina and are at risk of detachment of the retina later in life. Rarely, glaucoma and cataracts can also occur.
Prevention of Retinopathy of Prematurity
When premature newborns need oxygen, oxygen levels are monitored carefully so that the lowest amount of oxygen necessary can be used. Oxygen levels can be indirectly monitored using a pulse oximeter (an external sensor that measures the level of oxygen in the blood going through a finger or toe).
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
Children's Eye Foundation of AAPOS: Practical information about prevention, detection, research, and education to protect the vision of children






