



Mitral regurgitation is leakage of blood backward through the mitral valve each time the left ventricle contracts.
Disorders that directly affecting the mitral valve, such as mitral valve prolapse, and heart attack are the most common causes of mitral regurgitation. Rheumatic fever is the most common cause in places where antibiotics are not readily available to treat streptococcal infections.
When regurgitation is severe, people may have shortness of breath.
Mild regurgitation may not need treatment, but people with more severe regurgitation may need surgery to replace the damaged heart valve.
(See also Overview of Heart Valve Disorders and the video .)
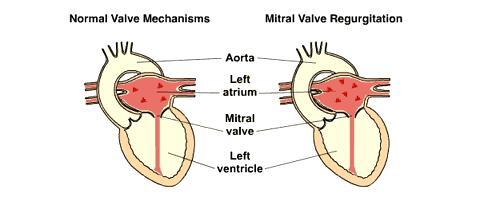
The mitral valve is in the opening between the left atrium and the left ventricle. The mitral valve opens to allow blood from the left atrium to fill the left ventricle and closes as the left ventricle contracts to pump blood only out into the aorta and not back into the left atrium. When the mitral valve does not close completely, some blood leaks backward into the left atrium, termed regurgitation.

Complications
Mitral valve regurgitation increases the amount of blood (blood volume) and the pressure in the left atrium. The increased blood pressure in the left atrium increases blood pressure in the veins leading from the lungs to the heart (pulmonary veins) and causes the left atrium to enlarge to accommodate the extra blood leaking back from the ventricle. An enlarged atrium often beats rapidly in an irregular pattern (a disorder called atrial fibrillation), which reduces the heart's pumping efficiency because the fibrillating atrium is quivering rather than pumping. Consequently, blood does not flow through the atrium briskly, and blood clots may form inside the chamber. If a clot breaks loose (becoming an embolus), it is pumped out of the heart and may block an artery, possibly causing a stroke or other damage.
Severe regurgitation can result in heart failure, in which increased pressure in the atrium causes fluid accumulation (congestion) in the lungs, or in which reduced forward flow of blood from the ventricle to the body deprives organs of the proper amount of blood. The left ventricle may gradually enlarge and weaken, further worsening heart failure.
Causes of Mitral Regurgitation
Mitral valve regurgitation may develop suddenly as a result of infective endocarditis, an infection of the valve, or because of injury to the valve or its supporting structures. The valve or its supporting structures can be damaged by a heart attack, coronary artery disease, or weakness in the tissues of these structures (myxomatous degeneration).
More often, however, mitral regurgitation develops slowly as a result of gradual deterioration of the valve (caused by mitral valve prolapse or rheumatic heart disease) or enlargement of the left ventricle, which pulls the valve apart and prevents it from closing properly. This enlargement is caused by a heart attack or another disorder that weakens the heart muscle (such as a cardiomyopathy).
Rheumatic fever—a childhood illness that sometimes occurs after untreated strep throat or scarlet fever—is the most common cause of mitral regurgitation worldwide. In regions where rheumatic fever is common, it can cause regurgitation, mitral stenosis, or both, sometimes 10 years or more after the initial infection. Repeated attacks of rheumatic fever hasten valve deterioration. However, in regions where antibiotics are widely used to treat infections such as strep throat, like North America and Western Europe, rheumatic fever is rare . In these regions, rheumatic fever is a common cause of mitral regurgitation only among older adults who did not have the benefit of antibiotics during their youth and among people who have moved from regions where antibiotics are not widely used.
Symptoms of Mitral Regurgitation
Mild mitral regurgitation may not cause any symptoms. When regurgitation is more severe or when there is atrial fibrillation, people may have palpitations (an awareness that their heart beat has changed rhythm) or shortness of breath. People with heart failure may have cough, shortness of breath during exertion or at rest, and swelling in the legs.
Diagnosis of Mitral Regurgitation
Physical examination
Echocardiography
Mitral regurgitation is usually suspected based on the characteristics of the heart murmur (abnormal heart sound) heard through a stethoscope. The murmur is a distinctive sound produced by blood leaking backward into the left atrium when the left ventricle contracts. The disorder is sometimes diagnosed when a doctor hears this murmur during a routine physical examination.
Doctors then do echocardiography, which uses ultrasound waves to produce an image of the heart structures and blood flow, provides the most information about the size of the atrium and ventricle and the amount of blood leaking, so that the severity of the regurgitation can be determined.
Electrocardiography (ECG) and chest x-rays show that the left ventricle is enlarged. If mitral regurgitation is severe, the chest x-ray may also show fluid accumulation in the lungs.
Cardiac catheterization is often done when surgery is planned to repair or replace a mitral valve so that doctors can identify coronary artery disease that could also be treated during the heart surgery.
Treatment of Mitral Regurgitation
Sometimes valve repair or replacement
If mitral regurgitation is mild, no specific treatment may be required. However, the regurgitation may gradually worsen, so echocardiography is done periodically to help determine whether surgery has become necessary. Surgery must be done before the heart muscle becomes permanently weakened.
When more serious regurgitation causes heart failure in people who cannot undergo surgery, these people are given certain medications for heart failure, such as sacubitril/valsartan, spironolactone, and carvedilol (When more serious regurgitation causes heart failure in people who cannot undergo surgery, these people are given certain medications for heart failure, such as sacubitril/valsartan, spironolactone, and carvedilol ( ). People with atrial fibrillation are given anticoagulants such as warfarin.). People with atrial fibrillation are given anticoagulants such as warfarin.
Surgery may involve
Repairing the valve
Replacing it with an artificial (prosthetic) valve
Mitral valve repair can be done during open heart surgery in which doctors insert a ring that reduces the size of the valve opening. Another method of repair is transcatheter edge-to-edge repair (TEER). In TEER, which is less invasive than traditional mitral valve repair, the valve is repaired by inserting a clip that decreases the size of the valve opening. The clip is inserted using a catheter passed up to the heart through a vein in the groin (the femoral vein).
Mitral valve replacement with either a mechanical or a bioprosthetic valve is done via open-heart surgery.
Repairing or replacing the valve (via traditional open-heart surgery) eliminates regurgitation or reduces it enough to make the symptoms tolerable and prevent damage to the heart. When possible, repairing the valve with a ring is preferable to replacing it because a repaired valve usually functions better than a mechanical or bioprosthetic valve and the person does not require lifetime anticoagulation therapy. TEER is not as effective as the traditional repair or replacement. TEER is recommended only for patients with severe mitral regurgitation who are too frail for open-heart surgery.
Prosthetic heart valves are susceptible to serious infection (infective endocarditis). People with an artificial valve should take antibiotics before surgical, dental, or medical procedures (see table ) to reduce the risk of an infection on a valve, even though this risk is small.
Atrial fibrillation, if present, may require treatment, including use of anticoagulants to prevent blood clots.
Prognosis for Mitral Regurgitation
Prognosis for mitral regurgitation varies by duration, severity, and cause. Some mitral regurgitation worsens and eventually becomes severe. Once it becomes moderate or severe, about 15% of people require valve repair or replacement..
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association: Heart Valve Disease: Provides comprehensive information on diagnosis and treatment of diseases of the heart valves
Drug Information for the Topic





