



Burns are injuries to tissue that result from heat, electricity, radiation, or chemicals.
Burns cause varying degrees of pain, blisters, swelling, and skin loss.
Small, shallow burns may need only to be kept clean and to have an antibiotic salve applied.
Deep, extensive burns can cause serious complications, such as shock and severe infections.
People with deep or extensive burns may require intravenous fluids, surgery, and rehabilitation, often at a burn center.
(See also Burns to the Eye.)
Burns are usually caused by heat (thermal burns), such as fire, steam, tar, or hot liquids. Burns caused by chemicals are similar to thermal burns, whereas burns caused by radiation, sunlight, and electricity differ significantly. Events associated with a burn, such as jumping from a burning building, being struck by debris, or being in a motor vehicle crash, may cause other injuries. Also, people who were burned by a fire often breathe smoke from the fire (smoke inhalation). Smoke can suffocate people, but it also contains different chemicals produced by the burning substance. Some of these chemicals, such as carbon monoxide and cyanide, can be toxic.
Thermal and chemical burns usually occur because heat or chemicals contact part of the body’s surface, most often the skin. Thus, the skin usually sustains most of the damage. However, severe surface burns may penetrate to deeper body structures, such as fat, muscle, or bone.
When tissues are burned, fluid leaks into them from the blood vessels, causing swelling. In addition, damaged skin and other body surfaces are easily infected because they can no longer act as a barrier against invading microorganisms.
Each year, more than 400,000 people in the United States visit an emergency department for treatment of burns, and approximately 4,000 people die of severe burns. Older adults and young children are particularly vulnerable. When children and older adults are burned, doctors also consider the possibility that the person was abused (see Child Neglect and Abuse and Elder Abuse).
Classification of Burns
Doctors classify burns according to strict, widely accepted definitions. The definitions classify the burn’s depth and the extent of tissue damage.
Burn depth
The depth of injury from a burn is described as superficial, partial thickness, or full thickness:
Superficial burns are the most shallow (also called first-degree burns). They affect only the top layer of skin (epidermis).
Partial-thickness burns (also called second-degree burns) extend into the middle layer of skin (dermis). Partial-thickness burns are sometimes further described as superficial (involving the more superficial part of the dermis) or deep (involving both the superficial and the deep parts of the dermis).
Full-thickness burns (also called third-degree burns) involve all 3 layers of skin (epidermis, dermis, and fat layer). Usually, the sweat glands, hair follicles, and nerve endings are destroyed as well.
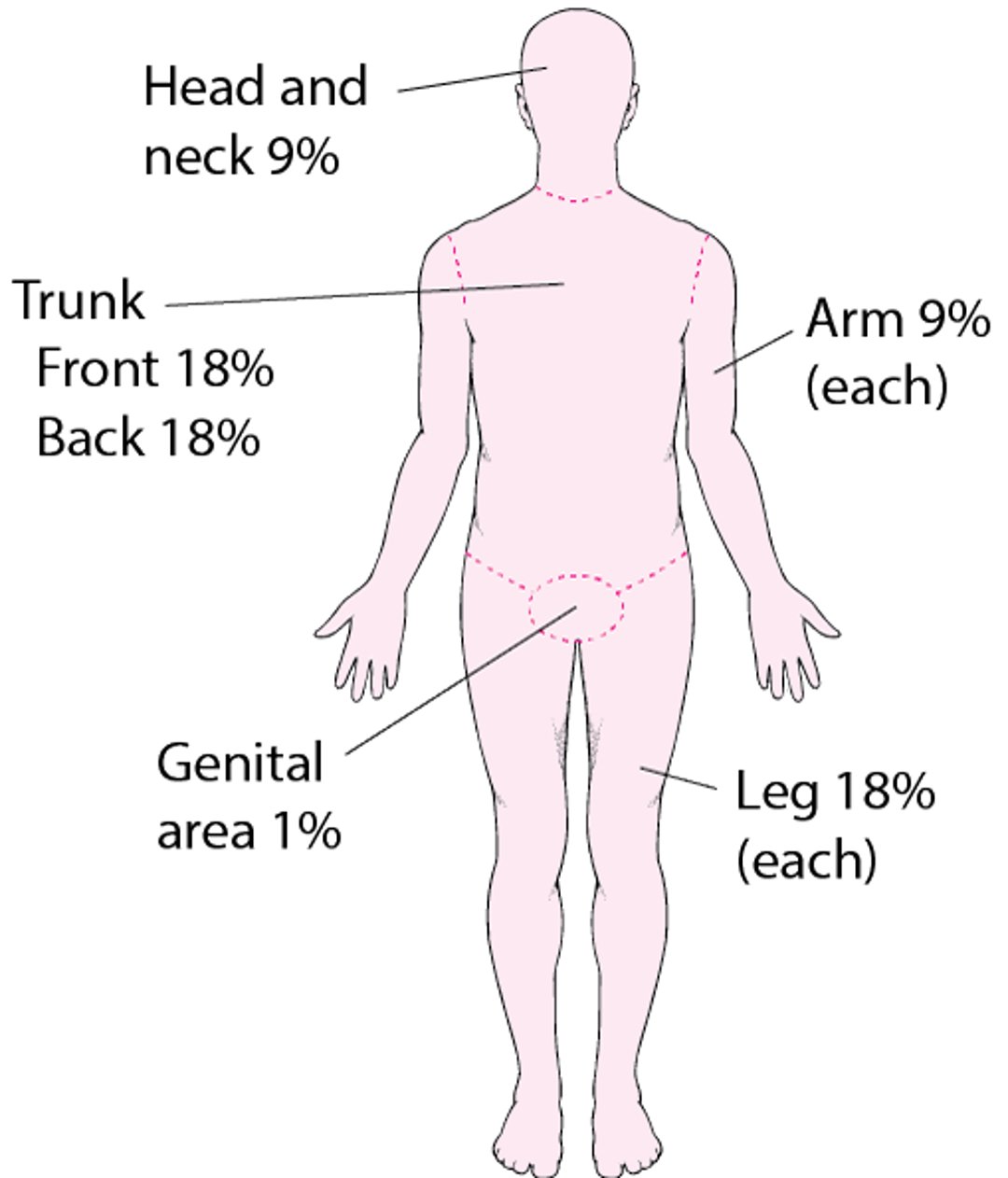
Estimating the Extent of a Burn
To determine the severity of a burn, doctors estimate what percentage of the body’s surface has partial-thickness or full-thickness burns. For adults, doctors use the rule of nines. This method divides almost all of the body into sections of 9% or of 2 times 9% (18%). For children, doctors use charts that adjust these percentages according to the child’s age (Lund-Browder charts). Adjustment is needed because different areas of the body grow at different rates. |

Burn severity


These burns are red and tender to the touch. They developed after contact with a hot stove.
© Springer Science+Business Media


This partial-thickness burn shows blisters and redness.
Image provided by Steven E. Wolf, MD.


Most of the third finger has a full-thickness (severe) burn, where the skin is dark and leathery. The base of the finger has blisters and redness, indicating that this part of the finger has a partial-thickness (second-degree) burn.
Image provided by Steven E. Wolf, MD.
Burns are classified as minor, moderate, or severe. These classifications may not correspond to a person’s understanding of those terms. For example, doctors may classify a burn as minor even though it can cause the person significant pain and interfere with normal activities. The severity determines how they are predicted to heal and whether complications are likely. Doctors determine the severity of the burn by its depth and by the percentage of the body surface that has partial-thickness or full-thickness burns. Special charts are used to show what percentage of the body surface various body parts comprise. For example, in an adult, the arm constitutes about 9% of the body. Separate charts are used for children because their body proportions are different.
Minor burns: All superficial burns as well as partial-thickness burns that involve less than 10% of the body surface usually are classified as minor.
Moderate and severe burns: Burns involving the hands, feet, face, or genitals, partial-thickness burns involving more than 10% of the body surface area, and all full-thickness burns involving more than 1% of the body are classified as moderate or, more often, as severe.
Symptoms of Burns
Symptoms of a burn wound vary with the burn’s depth:
Superficial burns are red, swollen, and painful. The burned area whitens (blanches) when lightly touched but does not develop blisters.
Partial-thickness burns are pink or red, swollen, and extremely painful. Within 24 hours (often shortly after the burn), blisters usually develop that may ooze a clear fluid. The burned area may blanch when touched.
Full-thickness burns usually are not painful because the nerves that sense pain have been destroyed. The skin becomes leathery and may be white, black, or bright red. The burned area does not blanch when touched, and hairs can easily be pulled from their roots without pain.
The appearance and symptoms of deep burns can worsen during the first hours or even days after the burn.
Did You Know...
|
Complications of Burns
Minor burns are usually superficial and do not cause complications. However, deep partial-thickness and full-thickness burns swell and take more time to heal. In addition, deeper burns can cause scar tissue to form. This scar tissue shrinks (contracts) as it heals. If the scarring occurs in a limb or digit, the resulting contracture may restrict movement of nearby joints.
Severe burns and some moderate burns can cause serious complications due to extensive fluid loss and tissue damage. These complications may take hours or days to develop. The deeper and more extensive the burn, the more severe the problems it tends to cause. Young children and older adults tend to be more seriously affected by complications than other age groups. The following are some complications of some moderate and severe burns:
Dehydration eventually develops in people with widespread burns, because fluid seeps from the blood into the burned tissues and, if burns are deep and extensive enough, into the whole body.
Shock develops if dehydration is severe.
Chemical imbalances can result from extensive burns.
Destruction of muscle tissue (rhabdomyolysis) sometimes occurs with full-thickness burns. The muscle tissue releases myoglobin, one of the muscle’s proteins, into the blood. If present in high concentrations, myoglobin harms the kidneys.
Infection can complicate burn wounds. Sometimes the infection can spread throughout the bloodstream and cause severe illness or death.
Thick, crusty surfaces (eschars) are produced by deep full-thickness burns. Eschars that completely encircle a limb or the chest can become too tight, cutting off blood supply to healthy tissues or impairing breathing.
The body temperature can become dangerously low (hypothermia) when cool fluids are given to try to correct dehydration, especially if the person is exposed in a cool emergency room environment as doctors evaluate and treat severe burns.
Diagnosis of Burns
Evaluation of depth and extent of wound
Sometimes blood and urine tests
Doctors frequently examine hospitalized people for complications and assess burn wound depth and extent. In people with large burns, blood pressure, heart rate, and urine volume are measured often to help assess the extent of dehydration or shock and the need for intravenous fluids. Doctors do blood tests to monitor the body’s electrolytes and blood count. Electrocardiography (ECG) and chest x-ray are also sometimes required. Tests of blood and urine are done to detect proteins caused by the destruction of muscle tissue (rhabdomyolysis) that sometimes occurs with deep full-thickness burns.
Treatment of Burns
For minor burns, cooling the wound with room temperature water for several minutes, followed by wound care and dressing
For severe burns, hospitalization and treatment of complications as well as burns
Before burns are treated, the burning agent must be stopped from inflicting further damage. For example, fires are extinguished. Clothing—especially any that is smoldering (such as melted synthetic shirts), covered with a hot substance (for example, tar), or soaked with chemicals—is immediately removed.
Hospitalization is sometimes necessary for optimal care of burns. For example, extensive partial-thickness or full-thickness burns require treatment with intravenous fluids; elevating a severely burned arm or leg above the level of the heart to prevent swelling is more easily accommodated in a hospital. In addition, burns that prevent people from carrying out essential daily functions, such as walking or eating, or that cause severe pain, often make hospitalization necessary. Full-thickness burns, burns occurring in the very young or the very old, and burns involving the hands, feet, face, or genitals are usually best treated at burn centers. Burn centers are hospitals that are specially equipped and staffed to care for burn victims.
Superficial minor burns
Superficial minor burns are immediately cooled with room temperature water for several minutes, if possible. Chemical burns may need to be rinsed for longer periods. The burn is carefully cleansed to prevent infection. If dirt is deeply embedded, doctors can give analgesics or numb the area by injecting a local anesthetic and then scrub the burn with a brush.
Often, the only treatment required is application of an antibiotic salve or cream, such as silver sulfadiazine. The salves prevent infection and form a seal to prevent further bacteria from entering the wound. A sterile bandage is then applied to protect the burned area from dirt and further injury. A Often, the only treatment required is application of an antibiotic salve or cream, such as silver sulfadiazine. The salves prevent infection and form a seal to prevent further bacteria from entering the wound. A sterile bandage is then applied to protect the burned area from dirt and further injury. Atetanus vaccination is given if needed.
Care at home includes keeping the burn clean to prevent infection. In addition, many people are given analgesics (pain relievers), sometimes opioids, for at least a few days. The burn can be covered with a nonstick bandage or with sterile gauze. The gauze can be removed without sticking by first being soaked in water.
Deep minor burns
As with more superficial burns, deep minor burns are usually treated with antibiotic salves. Sometimes doctors do not use antibiotic salves but instead apply special sterile dressings that can be left in place for several days to a week. Some of these dressings contain silver, which helps kill bacteria. Other dressings are slightly porous—just enough to allow fluid to drain from the burn but not enough to let bacteria through. Any dead skin and broken blisters should be removed by a health care practitioner before the antibiotic salve or dressing is applied. In addition, keeping a deeply burned arm or leg elevated above the heart for the first few days reduces swelling and pain. Compression dressings, such as elastic wraps, may also help reduce swelling and improve wound healing. The burn may require admission to a hospital or frequent re-examination at a hospital or doctor’s office, possibly as often as daily for the first few days.
A skin graft may be needed to replace burned skin that will not heal. Other skin grafts help by temporarily covering and protecting the skin as it heals on its own. In a skin grafting procedure, a piece of healthy skin is taken from sources including an
Unburned area of the person’s body (autograft)
Dead person (allograft)
Animal (xenograft)
Autografts can be solid pieces of skin or meshed grafts. For a meshed graft, doctors use a tool to make multiple, regularly spaced, small incisions in the piece of skin. The incisions allow the donor skin to be stretched to cover a much larger area (often several times the area of the original piece of skin). Meshed grafts are used in areas where appearance is less of a concern and when burns involve more than 20% of the body surface and donor skin is scarce. Meshed grafts heal with an uneven gridlike appearance, sometimes with excessive scarring. After any dead tissue is removed and the wound is clean, a surgeon sews or staples the skin graft over the burned area. Artificial skin can also be used. Autografts are permanent.
Allografts and xenografts provide temporary protection to skin that is healing but are rejected after 10 to 21 days by the person’s immune system, and will need to be removed. After allografts and xenografts are removed, an autograft will be needed if the wound is full-thickness (third-degree) burn and is too large to heal by itself. Burned skin can be replaced anytime within several days of the burn.
Physical and occupational therapy usually are needed to prevent immobility caused by scarring around the joints and to help people function if joint motion is limited. Stretching exercises are started within the first few days after the burn. Splints are applied to ensure that joints that are likely to be immobile rest in positions that are least likely to lead to contractures. The splints are left in place except when the joints are moved. If a skin graft has been used, therapy is not started for less than 1 to more than 3 days after the graft is attached so that the healing graft is not disturbed. Bulky dressings that put pressure on the burn can prevent large scars from developing.
Severe burns
Severe, life-threatening burns require immediate care. People who have gone into shock as a result of dehydration are given oxygen through a face mask.
Large amounts of intravenous fluids are given, beginning immediately, for people who have dehydration, shock, or burns that cover a large area of the body. Fluids are also given to people who develop destruction of muscle tissue. The fluids dilute the myoglobin in the blood, preventing extensive damage to the kidneys. Sometimes a chemical (sodium bicarbonate) is given intravenously to help dissolve myoglobin and thus also prevent further damage to the kidneys., or burns that cover a large area of the body. Fluids are also given to people who develop destruction of muscle tissue. The fluids dilute the myoglobin in the blood, preventing extensive damage to the kidneys. Sometimes a chemical (sodium bicarbonate) is given intravenously to help dissolve myoglobin and thus also prevent further damage to the kidneys.
A surgical procedure to cut open eschars that cut off blood supply to a limb or that impair breathing may be needed. This procedure is called escharotomy. Escharotomy usually causes some bleeding, but because the burn causing the eschar has destroyed the nerve endings in the skin, there is little pain.
Skin care is extremely important. Keeping the burned area clean is essential, because the damaged skin is easily infected. Cleansing may be accomplished by gently running water over the burns periodically. Wounds are cleansed and bandages changed at various intervals (usually once per day or less frequently), depending on the type of dressing. As with deep minor burns, skin grafts are needed to cover burns that will not heal.
A proper diet that includes adequate amounts of calories, protein, and nutrients is important for healing. People who cannot consume enough calories may drink nutritional supplements or receive them by way of a tube inserted through the nose into the stomach (a nasogastric tube), or less often nutrition may be given intravenously. Additional vitamins and minerals are usually given.
Physical and occupational therapy are needed.
Depression is treated. Because severe burns take a long time to heal and can cause disfigurement, people can become depressed. Depression often can be relieved with medications, psychotherapy, or both.
Prognosis for Burns
Superficial and some partial-thickness burns heal in days to weeks without scarring. Deep partial-thickness and small full-thickness burns take weeks to heal and usually cause scarring. Most require skin grafting. Burns that involve more than 90% of the body surface, or more than 60% in an older adult, are often fatal.
Drug Information for the Topic





