Hip fractures may occur in the round upper end (head) of the thighbone, in the narrow part of the thighbone just below the head (neck), or in the bumps in the broader area just below the neck.
Hip fractures usually occur in older people and often result from a minor fall, particularly in people with osteoporosis.
Usually, moving the affected leg, standing, and/or walking causes substantial pain
Doctors confirm the diagnosis with x-rays or sometimes other imaging tests.
Surgery is usually done to repair the hip or sometimes to replace the joint.
(See also Overview of Fractures.)
Hip fractures are more common among older people because they are more likely
To have osteoporosis (which weakens bones)
To fall
To take medications that increase the risk of hip fractures (see Aging and Medications)
Most hip fractures result from falls, but in older people with osteoporosis, the stresses of ordinary activity—such as rolling over in bed, getting up from a chair, or walking—can break the hip.
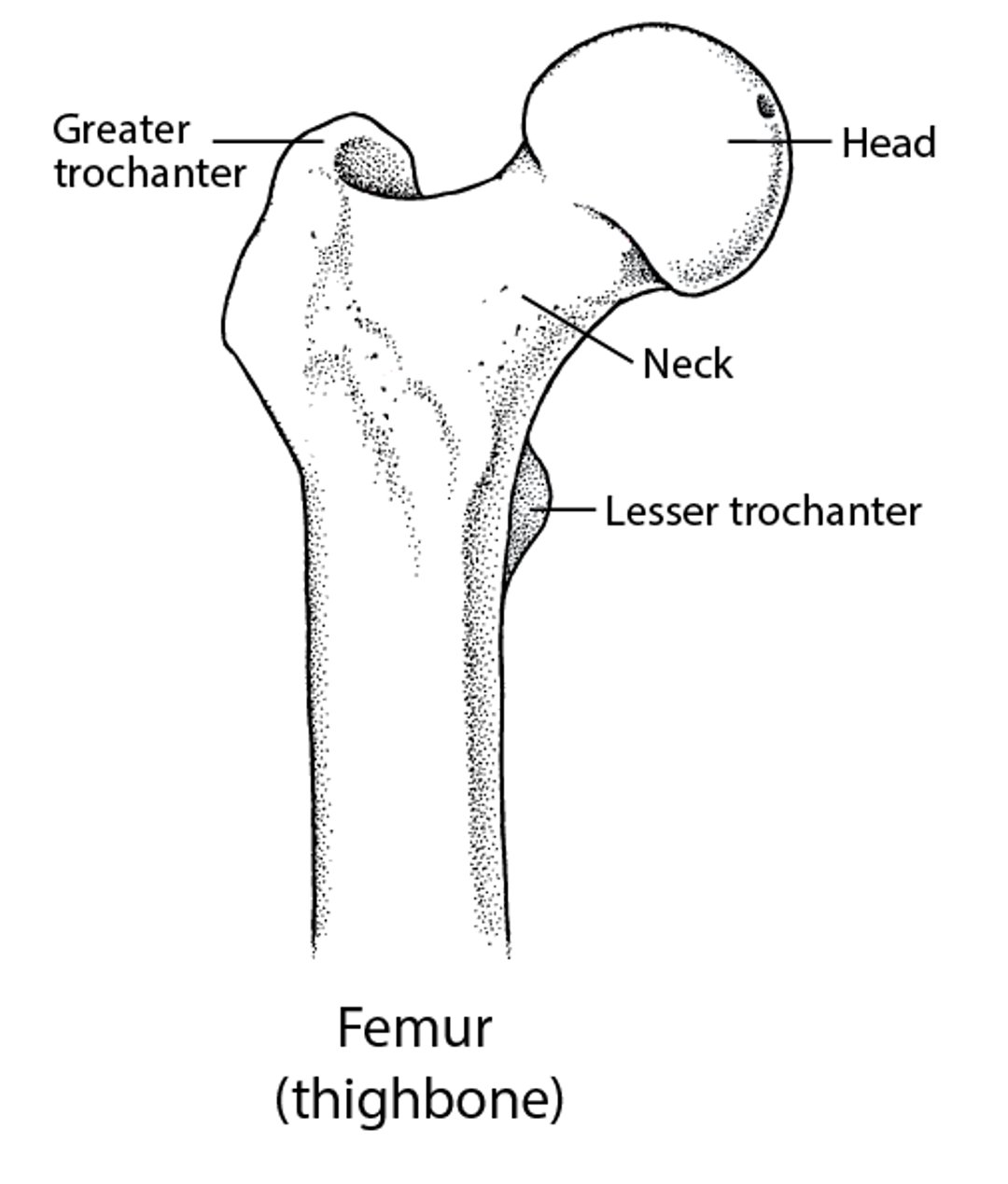
The hip joint consists of the round upper end (head) of the thighbone (femur) and part of the pelvic bone. The round head of the thighbone fits into the cup-shaped cavity in the pelvic bone, making a ball-and-socket joint. Below the head, the thighbone narrows, forming the neck of the thighbone. Below the neck is a broader area that contains two large bumps (called trochanters). The strong muscles of the legs and buttocks are attached to the trochanters by tendons.
The Femur: Part of the Hip Joint

Most hip fractures occur just below the head of the thighbone. There are two common types:
Femoral neck (subcapital) hip fractures, which occur in the neck of the thighbone
Intertrochanteric hip fractures, which go through the large bumps just below the neck
Hip fractures can also occur in the head of the femur or below the large bumps (called subtrochanteric fractures).
Femoral neck hip fractures are particularly problematic because the fracture often disrupts the blood supply to the head of the bone. Without a good blood supply, the bone cannot grow back together, and it may eventually collapse and die (called osteonecrosis). Severe, painful arthritis may develop.
Intertrochanteric hip fractures rarely interrupt the blood supply to the head of the femur. The broken surface of the bone may bleed but not usually enough to cause serious problems. These fractures usually result from a fall or direct blow.

Symptoms of Hip Fractures
Hip fractures are usually very painful and usually cause pain in the groin.
If the broken pieces of bone have separated, people cannot walk, stand, or move their leg. When they lie down, the affected leg may appear shorter and may turn out. However, if the broken pieces have been jammed together and the fracture is small, people can sometimes walk and may have only mild pain, and the leg appears normal.
If a lot of blood leaks from the fracture or from torn blood vessels nearby, people may feel light-headed or weak. The area may swell, and a purplish bruise may develop.
Sometimes when the hip is broken, pain seems to come from the knee instead of the hip. It feels that way because the knee and the hip share part of the same nerve pathways. Such pain is called referred pain.
If the hip fracture forces people to stay in bed for a long time, they are at increased risk of developing serious problems. Problems due to bed rest include
Blood clots, which may lead to pulmonary embolism
Mental confusion
Loss of muscle and a decrease in general physical fitness (called deconditioning)
Older people are more likely to have problems due to bed rest, and these problems may have more serious consequences. The hip fracture may change how they live. Older people may be unable to do their usual daily activities. They may need someone to help them at home or may need to move to a nursing home. People may become depressed if the fracture limits what they can do or ends their independence.
Diagnosis of Hip Fractures
X-rays
Sometimes magnetic resonance imaging or computed tomography
(See also Diagnosis of Fractures.)
Doctors suspect a hip fracture based on the person's description of the injury, symptoms, and results of the physical examination.
An x-ray usually shows obvious fractures and can help doctors confirm the diagnosis of a hip fracture. However, x-rays sometimes appear normal even when a fracture is present—for example, when the fracture is small and the fragments are still in place. Thus, if doctors still suspect a hip fracture or if the person continues to have pain and cannot stand a day or more after a fall, they use magnetic resonance imaging (MRI) to check for small fractures. Computed tomography (CT) is sometimes used, but it is less accurate for detecting small hip fractures.
Treatment of Hip Fractures
Usually surgery to repair or replace the hip
Rehabilitation
Usually, treatment of a hip fracture consists of surgery because it shortens the time people have to stay in bed and reduces the risk of the serious problems that bed rest can cause. Surgery enables people to get out of bed and begin walking as soon as possible. Usually, people can take a few steps with a walker 1 to 2 days after the operation.
Rehabilitation (physical therapy) is started as soon as possible after treatment of a hip fracture.
Did You Know...
|
Fractured hips may be surgically repaired or replaced. The procedure used for repair is called open reduction with internal fixation (ORIF). The hip is repaired if the fracture is not too severe. The hip may be replaced (called arthroplasty) when the fracture is severe or when the blood supply to the head of the thighbone has been disrupted.
While waiting for hip surgery in the emergency department, older people may be in pain. To help control the pain, doctors may inject an anesthetic into a nerve in the hip. This procedure (called a nerve block) prevents the nerves from sending pain signals to the brain.
Hip repair
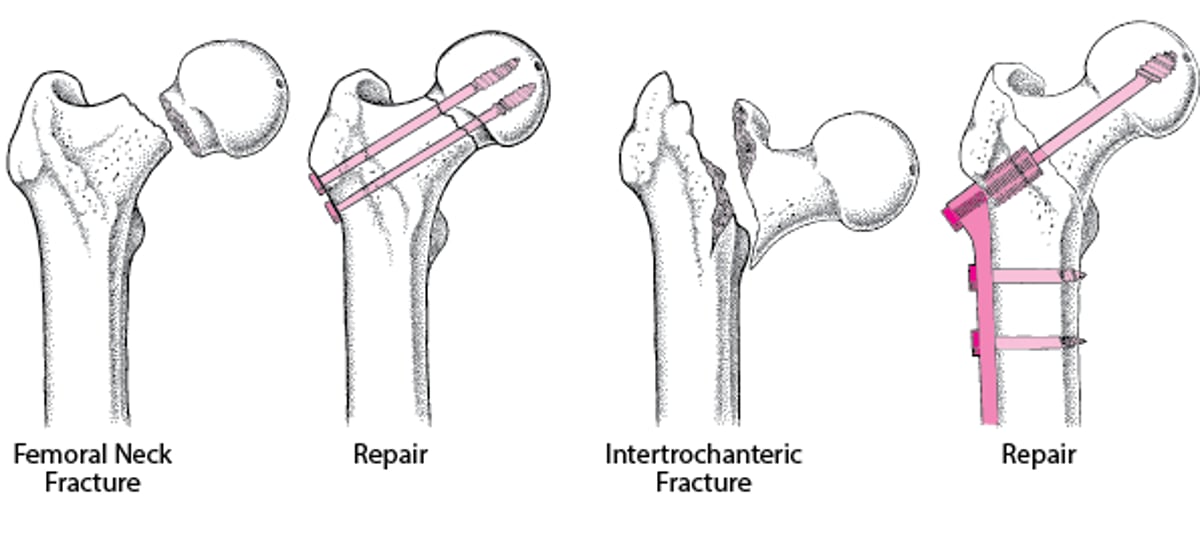
Femoral neck hip fractures may be repaired by inserting metal pins through the neck and into the head of the thighbone.
Intertrochanteric hip fractures can be repaired by attaching a sliding compression screw and metal side plate, which holds the bone fragments in their normal position while the fracture heals. This repair is usually strong enough to enable people to stand and put their weight on the affected leg shortly after surgery. Although the bone usually heals in a couple of months, most people need at least 6 months before they feel as comfortable and strong and can walk as they did before the fracture. However, increasingly, hip fractures are being treated with intramedullary screws (a type of screw used to stabilize the bone) or total hip replacement.
Repairing a Fractured Hip
Hip joints are repaired when the fracture is not too severe. How the repair is done depends on where the thighbone (femur) is fractured:
Hip repair preserves the person’s own hip joint. |

Hip replacement
Part or all of the hip joint may be replaced. Before replacing the joint, doctors remove the broken pieces of bone.
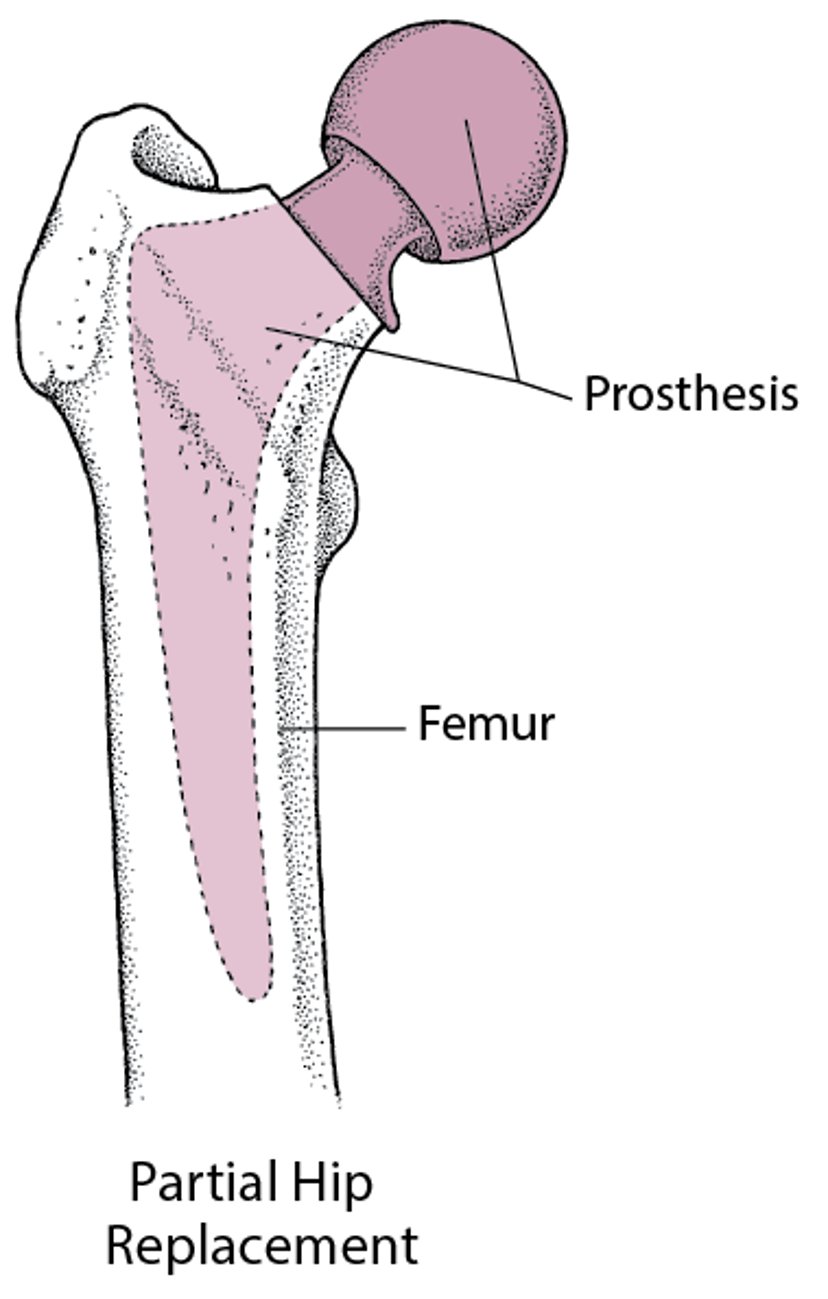
If partial hip replacement (hemiarthroplasty) is needed, doctors use a ball-shaped metal part (prosthesis) designed to fit into the joint socket in the pelvic bone. The prosthesis has a strong stem that fits within the center of the thighbone. Some prostheses are secured to the bone with a plastic cement that sets rapidly. Other prostheses have special porous or ceramic coatings that the surrounding living bone can bond to directly. Older people who walk very little and thus put little stress on the hip joint are usually treated with partial hip replacement.
Total hip replacement (total hip arthroplasty) is sometimes needed—for example, when a femoral neck fracture is likely to disrupt the hip's blood supply. Total hip replacement has greater risks than partial hip replacement. But because it results in better function, it is being increasingly used in older people who are active. For total hip replacement, the femoral head and the surface of the socket are replaced.

After most hip replacement operations, people usually begin walking with crutches or a walker 1 to 2 days after the operation, and they switch to a cane in 6 weeks.
Artificial joints do not last forever. People, especially if they are active or heavy, may need to have another operation 10 to 20 years later.
Joint replacement is often a good choice for older people because they are less likely to need another operation. Also, older people benefit greatly from being able to walk almost immediately after surgery.
Replacing a Hip
Part or all of the hip joint may be replaced:
|