



During pregnancy, women may need to take medications to treat new or existing health conditions. Also, certain vitamins are recommended during pregnancy. Before taking any medication (including over-the-counter medications) or dietary supplement (including medicinal herbs), a pregnant woman should consult a doctor. Women currently taking medications and planning to become pregnant should consult a doctor before pregnancy, if possible, to see if those medications need to be stopped or changed. (See also the Centers for Disease Control and Prevention: Medicine and Pregnancy.)
Medications or other substances taken by a pregnant woman may reach the fetus by crossing the placenta, the same route taken by oxygen and nutrients, which are needed for the fetus's growth and development. However, those that do not cross the placenta may still harm the fetus by affecting the uterus or the placenta.
Medications or other substances that a pregnant woman takes during pregnancy can affect the fetus in several ways:
No impact on the fetus and its development
Act directly on the fetus, causing damage, abnormal development (leading to birth defects), or death
Alter the function of the placenta, usually by causing blood vessels to narrow (constrict) and thus reducing the supply of oxygen and nutrients to the fetus from the mother (sometimes resulting in the baby being underweight and underdeveloped)
Cause the muscles of the uterus to contract forcefully, indirectly injuring the fetus by reducing its blood supply or triggering preterm labor and delivery
Affect the fetus indirectly (for example, medications that lower the mother's blood pressure may reduce blood flow to the placenta and thus reduce the supply of oxygen and nutrients to the fetus)
Some medications stay in the body and can have effects after they are stopped. For example, isotretinoin, a medication used to treat skin disorders, is stored in fat beneath the skin and is released slowly over weeks. Isotretinoin can cause birth defects if a woman becomes pregnant within 2 weeks after the medication is stopped. Therefore, women are advised to wait at least 3 to 4 weeks after the medication is stopped before they become pregnant. Some medications stay in the body and can have effects after they are stopped. For example, isotretinoin, a medication used to treat skin disorders, is stored in fat beneath the skin and is released slowly over weeks. Isotretinoin can cause birth defects if a woman becomes pregnant within 2 weeks after the medication is stopped. Therefore, women are advised to wait at least 3 to 4 weeks after the medication is stopped before they become pregnant.
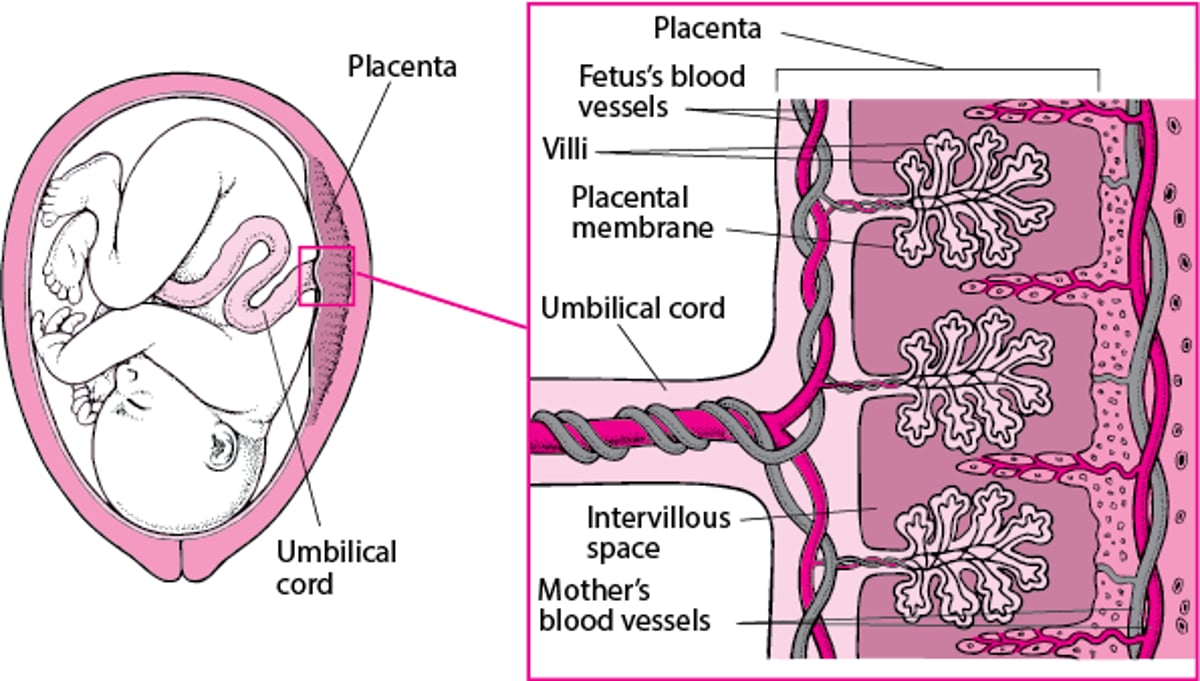
How Medications Cross the Placenta
Some of the fetus's blood vessels are contained in tiny hairlike projections (villi) of the placenta that extend into the wall of the uterus. The mother's blood passes through the space surrounding the villi (intervillous space). Only a thin membrane (placental membrane) separates the mother's blood in the intervillous space from the fetus's blood in the villi. Medications in the mother's blood can cross this membrane into blood vessels in the villi and pass through the umbilical cord to the fetus. |

How a medication affects a fetus depends on the
Stage of fetal development
Strength and dose of the medication
Permeability of the placenta (how easily substances pass through it)
Genetic factors in the pregnant woman, which affects how much of the medication is active and available
Pregnant woman's health (for example, nausea and vomiting may decrease absorption of a medication taken by mouth)
Timing and the Effects of Medications During Pregnancy
Time Frame | Possible Fetal Effects* | Status of the Fetus |
|---|---|---|
Within 20 days after fertilization | An all-or-nothing effect (death of the fetus or no effect at all) | The fetus is highly resistant to birth defects. |
3‒8 weeks after fertilization | Possibly no effect An obvious birth defect A permanent but subtle defect that is noticed only later in life An increased risk of childhood cancer, as may result from giving the mother radioactive iodine (to treat thyroid cancer) or using a radioactive substance in an imaging test (such as radionuclide scanning) | The fetus's organs are developing, making the fetus particularly vulnerable to birth defects. |
Second and third trimesters | Changes in the growth and function of normally formed organs and tissue Unlikely to cause obvious birth defects Unknown long-term effects | Organ development is complete. |
* Only certain medications are likely to have harmful effects. | ||
Government agencies that oversee drug safety may classify medications based on current knowledge about safety during pregnancy. In the United States, the US Food and Drug Administration (FDA) provides information about drug safety in pregnancy (see FDA: Medicine and Pregnancy). Knowledge about drug safety in pregnancy is based on research in humans and animals and on side effects that are reported by people who have taken the medication. In general, doctors advise pregnant women about taking a medication based on available research, importance of the medication to the health of the pregnant woman, and whether there are other treatments that have less risk to the pregnant woman or fetus. Medications are given in pregnancy if the benefits outweigh the risks.
Some Medications and Risk of Problems During Pregnancy*
Examples | Possible Problems |
|---|---|
Anti-anxiety medications | |
Benzodiazepines (such as diazepam, alprazolam, or lorazepam)(such as diazepam, alprazolam, or lorazepam) | When taken late in pregnancy, very slow breathing or a withdrawal syndrome (causing irritability, shaking, and exaggerated reflexes) in the newborn |
Antibiotics | |
Aminoglycosides (such as amikacin, gentamicin, neomycin, streptomycin, and tobramycin)(such as amikacin, gentamicin, neomycin, streptomycin, and tobramycin) | Damage to the fetus's ear (ototoxicity), resulting in variable deafness |
In women or fetuses with G6PD deficiency, the breakdown of red blood cells Possibly gray baby syndrome (a serious and often fatal disorder) | |
Fluoroquinolones (such as ciprofloxacin, ofloxacin, levofloxacin, and norfloxacin)(such as ciprofloxacin, ofloxacin, levofloxacin, and norfloxacin) | Possibility of bone and joint abnormalities (seen only in animals) |
In women or fetuses with G6PD deficiency, the breakdown of red blood cells | |
In women or fetuses with G6PD deficiency, the breakdown of red blood cells | |
Sulfonamides (such as sulfasalazine and trimethoprim- sulfamethoxazole)(such as sulfasalazine and trimethoprim- sulfamethoxazole) | When given late in pregnancy, jaundice and, without treatment, brain damage (kernicterus) in the newborn With sulfasalazine, much less risk of problemsWith sulfasalazine, much less risk of problems In women or fetuses with G6PD deficiency, the breakdown of red blood cells |
Slowed bone growth, permanent yellowing of the teeth, and increased risk of cavities in the child Occasionally, liver failure in the pregnant woman | |
Defects of the brain and spinal cord (neural tube defects), such as spina bifida | |
Factor Xa inhibitors such as rivaroxaban, apixaban, or edoxabanFactor Xa inhibitors such as rivaroxaban, apixaban, or edoxaban | Possible risk of bleeding in the pregnant woman or fetus |
Heparin or enoxaparinHeparin or enoxaparin | Rarely causes thrombocytopenia (a decrease in the number of platelets, which help blood clot) in the pregnant woman, possibly resulting in excessive bleeding |
WarfarinWarfarin | Birth defects including malformed bones, intellectual disability, congenital cataracts, and other problems with the eyes in the fetus Bleeding problems in the fetus and the pregnant woman |
Antidepressants | |
BupropionBupropion | Possible risk of birth defects in first trimester; likely safe in pregnancy |
CitalopramCitalopram | When taken during the first trimester, increased risk of birth defects (particularly heart defects) When taken during the third trimester, discontinuation syndrome (which includes dizziness, anxiety, irritability, fatigue, nausea, chills, and muscle aches) and persistent pulmonary hypertension of the newborn (the arteries to the lungs remain narrowed after delivery, limiting blood flow to the lungs and thus the amount of oxygen in the bloodstream) |
EscitalopramEscitalopram | When taken during the third trimester, discontinuation syndrome and persistent pulmonary hypertension of the newborn |
FluoxetineFluoxetine | When taken during the third trimester, discontinuation syndrome and persistent pulmonary hypertension of the newborn |
ParoxetineParoxetine | When taken during the first trimester, increased risk of birth defects, particularly heart defects When taken during the third trimester, discontinuation syndrome and persistent pulmonary hypertension of the newborn |
SertralineSertraline | When taken during the third trimester, discontinuation syndrome and persistent pulmonary hypertension of the newborn |
VenlafaxineVenlafaxine | When taken during the third trimester, discontinuation syndrome |
Antiemetic medications (used to relieve nausea) | |
Doxylamine and pyridoxine (vitamin B6)Doxylamine and pyridoxine (vitamin B6) | No increased risk of birth defects |
MetoclopramideMetoclopramide | When taken during the third trimester and/or delivery, abnormal muscle movements (extrapyramidal symptoms) or a blood disorder (methemoglobinemia) may potentially occur in the newborn |
MeclizineMeclizine | Birth defects seen only in animals |
OndansetronOndansetron | No conclusive evidence of birth defects in animals When taken during the first trimester, possible risk of congenital heart disease |
PromethazinePromethazine | No conclusive evidence of birth defects in animals Possible risk of bleeding in the newborn |
Antifungal medications | |
Amphotericin BAmphotericin B | No increased risk of birth defects, but no well-designed studies done in pregnant women |
FluconazoleFluconazole | No increased risk of birth defects after a single low dose When high doses are taken for most or all of the first trimester, increased risk of birth defects, such as abnormalities in the heart, face, skull, ribs, and limbs |
MiconazoleMiconazole | No increased risk of birth defects when applied to the skin When taken by mouth, side effects in animal studies When inserted into the vagina, no increased risk of birth defects |
TerconazoleTerconazole | No increased risk of birth defects When inserted into the vagina, no increased risk of birth defects |
Antihistamines | |
LoratadineLoratadine | Possibly in male newborns, a birth defect of the urethra in which the opening of the urethra is in the wrong place on the penis (hypospadias); likely safe in pregnancy |
MeclizineMeclizine | Birth defects in rodents but no proof of this effect in humans |
Antihypertensive medications | |
Aldosterone antagonists (medications that block the action of the hormone aldosterone), such as spironolactone and eplerenone(medications that block the action of the hormone aldosterone), such as spironolactone and eplerenone | With spironolactone, possible development of feminine characteristics in male fetusesWith spironolactone, possible development of feminine characteristics in male fetuses With eplerenone, no increased risk of birth defects in animals, but no well-designed studies done in pregnant womenWith eplerenone, no increased risk of birth defects in animals, but no well-designed studies done in pregnant women |
When taken late in pregnancy, possible kidney damage in the fetus, a reduction in the amount of fluid around the developing fetus (amniotic fluid), and defects of the face, limbs, and lungs | |
Labetalol is the preferred beta-blocker in pregnancyLabetalol is the preferred beta-blocker in pregnancy When atenolol, propranolol, and some other beta-blockers are taken during pregnancy, a slowed heart rate, a low blood sugar level, and possibly inadequate growth of the fetus (When atenolol, propranolol, and some other beta-blockers are taken during pregnancy, a slowed heart rate, a low blood sugar level, and possibly inadequate growth of the fetus (growth restriction) and preterm birth Low blood pressure in the mother | |
Nifedipine and nicardipine are the preferred calcium channel blockers during pregnancyNifedipine and nicardipine are the preferred calcium channel blockers during pregnancy | |
A decrease in the levels of oxygen, sodium, and potassium and in the number of platelets in the fetus's blood Inadequate growth of the fetus | |
Antipsychotic medications | |
AripiprazoleAripiprazole | When taken during the third trimester, increased risk of abnormal muscle movements (extrapyramidal symptoms) and/or withdrawal symptoms in newborns following delivery |
HaloperidolHaloperidol | Harmful effects in animals When taken during the first trimester, possible birth defects in the limbs When taken during the third trimester, increased risk of the following:
|
LurasidoneLurasidone | No evidence of harmful effects in animals When taken during the third trimester, increased risk of the following:
|
OlanzapineOlanzapine | Harmful effects in animals When taken during the third trimester, increased risk of the following:
|
CarbamazepineCarbamazepine | Increased risk of birth defects, including neural tube defects (such as spina bifida) Bleeding problems in the newborn (hemorrhagic disease of the newborn), which can be prevented if pregnant women take vitamin K by mouth every day for a month before delivery or if the newborn is given an injection of vitamin K soon after birth |
LamotrigineLamotrigine | No substantial increased risk of birth defects |
LacosamideLacosamide | Additional data regarding effects required |
LevetiracetamLevetiracetam | Minor bone abnormalities seen in animals No substantial increased risk in people |
PhenobarbitalPhenobarbital | Increased risk of birth defects, including neural tube defects (such as spina bifida) Bleeding problems in the newborn |
PhenytoinPhenytoin | Increased risk of birth defects (such as cleft lip and heart defects) Bleeding problems in the newborn |
Trimethadione | High risk of birth defects (such as cleft palate and defects of the heart, skull, face, hands, and abdomen) Risk of a miscarriage |
Valproate | Increased risk of birth defects, including cleft palate, neural tube defects (such as a meningomyelocele), and defects of the heart, face, skull, spine, and limbs |
Chemotherapy drugs | |
Actinomycin | Possibility of birth defects (seen only in animals) |
BusulfanBusulfan | Birth defects such as underdevelopment of the lower jaw, cleft palate, abnormal development of the skull bones, spinal defects, ear defects, and clubfoot Inadequate growth of the fetus (growth restriction) |
ChlorambucilChlorambucil | Birth defects such as underdevelopment of the lower jaw, cleft palate, abnormal development of the skull bones, spinal defects, ear defects, and clubfoot Inadequate growth of the fetus (growth restriction) |
ColchicineColchicine | Possibility of birth defects (seen in animals) Abnormalities in sperm in male children |
CyclophosphamideCyclophosphamide | Birth defects such as underdevelopment of the lower jaw, cleft palate, abnormal development of the skull bones, spinal defects, ear defects, and clubfoot Inadequate growth of the fetus (growth restriction) |
DoxorubicinDoxorubicin | Heart problems for the mother, depending on the dose taken Birth defects |
MercaptopurineMercaptopurine | Birth defects such as underdevelopment of the lower jaw, cleft palate, abnormal development of the skull bones, spinal defects, ear defects, and clubfoot Inadequate growth of the fetus (growth restriction) |
MethotrexateMethotrexate | Birth defects such as underdevelopment of the lower jaw, cleft palate, abnormal development of the skull bones, spinal defects, ear defects, and clubfoot Inadequate growth of the fetus (growth restriction) |
VinblastineVinblastine | Possibility of birth defects (seen only in animals) |
VincristineVincristine | Possibility of birth defects (seen only in animals) |
Mood-stabilizing medication | |
AripiprazoleAripiprazole | When taken during the third trimester, increased risk of abnormal muscle movements (extrapyramidal symptoms) and/or withdrawal symptoms in newborns following delivery |
When taken during the first trimester, increased risk of birth defects (mainly of the heart) When taken later in pregnancy, lethargy, reduced muscle tone, poor feeding, underactivity of the thyroid gland, and nephrogenic diabetes insipidus in the newborn | |
RisperidoneRisperidone | Harmful effects in animals No evidence of increased risk of birth defects, but no well-designed studies done in pregnant women When taken during the third trimester, increased risk of the following:
|
Chlorpropamide GlyburideGlyburide MetforminMetformin Tolbutamide | A very low blood sugar level in the newborn |
Nonsteroidal anti-inflammatory drugs (NSAIDs) | |
Aspirin and other salicylatesAspirin and other salicylates IbuprofenIbuprofen NaproxenNaproxen | When taken in large doses, possibly miscarriage during the first trimester, a delay in the start of labor, premature closing of the connection between the aorta and artery to the lungs (ductus arteriosus), jaundice, necrotizing enterocolitis (damage to the lining of the intestine), and (occasionally) brain damage in the fetus (kernicterus) and bleeding problems in a woman during and after delivery and/or in the newborn When taken late in pregnancy, a reduction in the amount of fluid around the developing fetus When low doses of aspirin are taken, no significant risk of birth defectsWhen low doses of aspirin are taken, no significant risk of birth defects |
BuprenorphineBuprenorphine | No evidence of increased risk of birth defects but may have other harmful effects on the fetus or newborn Restlessness, irritability, shaking, difficulty breathing, and feeding problems (symptoms of opioid withdrawal) in the newborn because, at birth, passage of the medication from the mother through the placenta stops |
CodeineCodeine HydrocodoneHydrocodone HydromorphoneHydromorphone MeperidineMeperidine MorphineMorphine | Restlessness, irritability, shaking, difficulty breathing, and feeding problems (symptoms of opioid withdrawal) in the newborn, possibly occurring 6 hours to 8 days after birth If high doses are given in the hour before delivery, possibly drowsiness and a slowed heart rate in the newborn |
MethadoneMethadone | Restlessness, irritability, shaking, difficulty breathing, and feeding problems (symptoms of opioid withdrawal) in the newborn |
Sex hormones | |
DanazolDanazol | When taken very early in pregnancy, masculinization of a female fetus’s genitals, sometimes requiring surgery for correction |
Hormonal contraceptives (birth control pills, patches, or rings; contraceptive injections or implants; hormonal intrauterine devices [IUDs]) | Exposure to estrogen-progestin contraceptives prior to conception or during pregnancy does not appear to be associated with an increased risk of major birth defects Exposure to medroxyprogesterone acetate does not appear to increase risk of major birth defectsExposure to medroxyprogesterone acetate does not appear to increase risk of major birth defects |
17-hydroxyprogesterone caproate17-hydroxyprogesterone caproate | Safe in second or third trimester of pregnancy |
Progesterone (oral or vaginal)Progesterone (oral or vaginal) | Exposure during pregnancy not associated with increased risk of major birth defects |
Skin treatment | |
IsotretinoinIsotretinoin | Birth defects, such as heart defects, small ears, and hydrocephalus (sometimes called water on the brain) Intellectual disability Risk of miscarriage |
Thyroid medications | |
LevothyroxineLevothyroxine | Preferred treatment of hypothyroidism during pregnancy; safe in pregnancy |
MethimazoleMethimazole | An enlarged or underactive thyroid gland in the fetus Facial and scalp defects in the newborn Other potential abnormalities |
PropylthiouracilPropylthiouracil | An enlarged or underactive thyroid gland in the fetus Liver damage in the mother |
Radioactive iodine | Destruction of the thyroid gland in the fetus When given near the end of the first trimester, a very overactive and enlarged thyroid gland in the fetus Increased risk of childhood cancer |
Triiodothyronine | An overactive and enlarged thyroid gland in the fetus |
Vaccines | |
No known safety concerns for pregnant people or for their fetuses or newborns | |
No safety concerns for pregnant people or for fetuses or newborns | |
Tetanus, reduced diphtheria toxoid, acellular pertussis (Tdap) vaccine | No safety concerns for pregnant people or for fetuses or newborns |
Live-virus vaccines such as those formeasles, mumps, and rubella; chickenpox (varicella); polio; and yellow fever | With rubella and varicella vaccines, potential infection of the placenta and developing fetus With other live vaccines, potential but unknown risks |
Other medications | |
Corticosteroids | Possibly a cleft lip when taken during the first trimester |
HydroxychloroquineHydroxychloroquine | No increased risks at the doses usually used |
IsoniazidIsoniazid | Possible harmful effects on the liver or damage to the peripheral nerves (causing abnormal sensations and/or weakness) |
Pseudoephedrine (a decongestant)Pseudoephedrine (a decongestant) | Narrowing of the blood vessels in the placenta, possibly reducing the amount of oxygen and nutrients the fetus receives and thus resulting in inadequate growth before birth Possible risk of a defect in the wall of the abdomen that allows the intestines to protrude outside the body (called gastroschisis) |
Vitamin K | In women or fetuses with G6PD deficiency, destruction of red blood cells (hemolysis) |
* Women who are pregnant or are planning to become pregnancy should talk with their doctor about the risks and benefits of medications before stopping or starting any medication. Unless medically necessary, medications should not be used during pregnancy. However, some medications are essential to maintain the health of the pregnant woman or the fetus, and women should not stop taking these before consulting their doctor. | |
† Opioids are used to relieve pain. However, they also cause an exaggerated sense of well-being, and if used too much, they can cause dependence and addiction. | |
‡ Insulin is usually preferred during pregnancy.‡ Insulin is usually preferred during pregnancy. | |
G6PD = glucose-6-phosphate dehydrogenase. | |
Vaccines During Pregnancy
Immunization is as effective in women who are pregnant as in those who are not. (See also Centers for Disease Control and Prevention (CDC): Pregnancy and Vaccination.)
Vaccines made with a live virus (such as the rubella vaccine and varicella vaccine) are not given to women who are or might be pregnant.
Other vaccines (such as those for cholera, hepatitis A, hepatitis B, plague, rabies, and typhoid) are given to pregnant women only if they are at substantial risk of developing that particular infection and if the risk of side effects from the vaccine is low.
Some vaccines that are considered safe in pregnant women and are recommended during pregnancy include
Influenza (flu) vaccine for all women who will be or are pregnant during the flu season
Tetanus-diphtheria-pertussis (Tdap) vaccine (protects against pertussis [whooping cough]) during the third trimester of each pregnancy
COVID-19 vaccination for people who are pregnant, breastfeeding, trying to get pregnant, or might become pregnant in the future
Evidence about the safety and effectiveness of COVID-19 vaccination during pregnancy has been growing. These data suggest that the benefits of receiving a COVID-19 vaccine outweigh any known or potential risks of vaccination during pregnancy. (See also CDC: COVID-19 Vaccines While Pregnant or Breastfeeding.)
In August 2023, the US Food and Drug Administration (FDA) approved use of a respiratory syncytial virus (RSV) vaccine in pregnant individuals between 32 to 36 weeks of pregnancy, with a warning to avoid use prior to 32 weeks (see FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants).
Medications Used to Treat Heart and Blood Vessel Disorders During Pregnancy
Medications to lower high blood pressure (antihypertensives) may be needed by pregnant women who have had high blood pressure before pregnancy or who develop it during pregnancy. Either type of high blood pressure increases the risk of problems for a woman (such as preeclampsia) and for the fetus (see High Blood Pressure During Pregnancy). However, antihypertensives can reduce blood flow to the placenta if they lower blood pressure too rapidly in pregnant women. Pregnant women who have to take these medications are closely monitored.
Several types of antihypertensives, such as angiotensin-converting enzyme (ACE) inhibitors and thiazide diuretics, are usually not given to pregnant women. These medications can cause serious problems in the fetus, such as kidney damage, inadequate growth before birth (growth restriction), and birth defects. Spironolactone is also not given to pregnant women. This medication may cause the development of feminine characteristics (feminization) in a male fetus.), and birth defects. Spironolactone is also not given to pregnant women. This medication may cause the development of feminine characteristics (feminization) in a male fetus.
Digoxin, used to treat Digoxin, used to treatheart failure and some abnormal heart rhythms, readily crosses the placenta. But at the usual doses, digoxin typically has little effect on the baby before or after birth.
Antidepressants During Pregnancy
Clinical depression is common during pregnancy and, therefore, antidepressants, particularly certain selective serotonin reuptake inhibitors (SSRIs) such as sertraline, are commonly used during pregnancy. For pregnant women, the benefits of treating depression usually outweigh the risks., particularly certain selective serotonin reuptake inhibitors (SSRIs) such as sertraline, are commonly used during pregnancy. For pregnant women, the benefits of treating depression usually outweigh the risks.
Paroxetine appears to increase the risk of heart birth defects. So if a pregnant woman takes paroxetine, echocardiography should be done to evaluate the fetus's heart. However, other SSRIs do not increase this risk.
If a pregnant woman takes antidepressants, the newborn may have withdrawal symptoms (such as irritability and shaking) after delivery. To prevent these symptoms, doctors may gradually reduce the dose of the antidepressant during the third trimester and stop the medication before the baby is born. However, if a woman has significant signs of depression or if symptoms worsen as the dose is reduced, antidepressants should be continued. Depression during pregnancy can lead to postpartum depression, which involves a serious change in mood and requires treatment.
Medications Used During Labor and Delivery
Medications used to relieve pain during pregnancy (such as local anesthetics and opioids) usually cross the placenta and can affect the newborn. For example, they can weaken the newborn's urge to breathe. Therefore, if these medications are needed during labor, they are given in the smallest effective doses.
Drug Information for the Topic





