


Prenatal testing for genetic disorders and birth defects involves testing a pregnant woman or fetus before birth (prenatally) to determine whether the fetus has certain abnormalities, including certain hereditary or spontaneous genetic disorders. Noninvasive screening tests (such as ultrasonography or blood tests) are often done first, and if the results are abnormal, a pregnant woman can decide whether to have invasive testing. Invasive tests, such as chorionic villus sampling, amniocentesis, and percutaneous umbilical blood sampling, use a sample of the fetus's deoxyribonucleic acid (DNA) and are more accurate. However, they may involve a low risk of losing the pregnancy or harm to the fetus.
Ultrasonography is often part of routine prenatal care. For other noninvasive or invasive tests for fetal genetic abnormalities or birth defects, prospective parents should discuss the accuracy of the test and any risks with their health care professional. Noninvasive tests, such as ultrasonography, usually do not have direct risks, but if the result is falsely positive (test is abnormal but the baby does not have an abnormality), it may lead a parent to do invasive testing, which has some risk.
Parents should weigh the risks against the benefits of doing a test and of knowing if their baby has an abnormality. For example, they should think about whether not knowing the results of testing would cause anxiety. They should think about how they would use the information if they did find out their baby has an abnormality. They should consider whether they would pursue an abortion. If they would not, they should consider whether they still want to know of an abnormality before birth (for example, to prepare psychologically) or whether knowing would only cause distress. For some parents, the risks outweigh the benefits of knowing whether their baby has a chromosomal abnormality, so they choose not to be tested.
Noninvasive Prenatal Tests for Genetic Abnormalities
Several types of noninvasive tests have been developed to try to detect certain abnormalities in a fetus. Current tests or combinations of tests can assess for
Chromosomal abnormalities, including trisomy 21 (Down syndrome), trisomy 13, and trisomy 18
Neural tube defects, such as spina bifida
Sometimes more than 1 type of test needs to be done, because not all tests detect both chromosomal abnormalities and neural tube defects.
Noninvasive prenatal tests are screening tests, which means that an abnormal result raises concern that a fetus may have an abnormality, but the result does not give definitive information. If a test is abnormal, prospective parents may choose to have an invasive prenatal test to be certain about whether a fetus has an abnormality. Noninvasive tests do not pose any risk to the fetus or pregnancy and consist of one or more of the following:
Blood test (using the mother's blood) for fetal DNA
Blood tests (using the mother's blood) for certain substances (called serum markers), such as alpha-fetoprotein or human chorionic gonadotropin
Ultrasonography to measure a specific fetal part (such as a fluid-filled space near the back of the fetus’s neck, called fetal nuchal translucency)
During pregnancy, some substances pass from the fetus to the mother and can be tested by doing blood tests on the mother. This includes some fetal DNA. Also, for certain fetal abnormalities, the fetus produces abnormal levels of certain serum markers.
Doctors usually offer to do blood tests to screen for fetal abnormalities as part of routine prenatal care. However, some prospective parents decide not to have any testing done.
Sometimes prospective parents decide to skip these noninvasive tests and proceed directly to invasive prenatal genetic testing (such as chorionic villus sampling or amniocentesis), especially if the couple is at increased risk of having a baby with a genetic abnormality.
If pregnancy is to be achieved using in vitro fertilization, genetic disorders can sometimes be diagnosed before the fertilized egg is transferred from the culture dish to the uterus (called preimplantation genetic diagnosis). (See also Overview of Chromosome and Gene Disorders and Overview of Birth Defects.)
Prospective parents should remember that screening tests are not always accurate. Screening tests may miss abnormalities or may indicate abnormalities when none are present.
Cell-Free DNA Screening Test
A common method of screening for fetal chromosomal abnormalities, including Down syndrome, trisomy 18, and trisomy 13, is analysis of cell-free DNA (cfDNA) in the mother's blood, which can be done as early as 10 weeks of pregnancy. For this test, small fragments of the fetus's DNA, which are present in the mother's blood in tiny amounts, are analyzed. Detection rates using this technology are higher than most other noninvasive methods.
Serum Marker Screening Test
Serum marker testing of the mother's blood may test for chromosomal abnormalities, neural tube defects, or both.
The choice of which serum marker testing to use may depend on timing (getting test results early in pregnancy), other preferences of the prospective parents, or which test a clinic or hospital usually uses. Important markers include the following:
Alpha-fetoprotein: A protein produced by the fetus
Pregnancy-associated plasma protein A (PAPP-A): A protein produced by the placenta
Estriol: A hormone formed from substances produced by the fetus
Human chorionic gonadotropin: A hormone produced by the placenta
Inhibin A: A hormone produced by the placenta
Serum marker screening can consist of different combinations of tests. Markers are usually measured at 10 to 13 weeks of pregnancy (first-trimester screening). Other markers are measured at 16 to 18 weeks of pregnancy (second-trimester screening).
Sometimes serum testing is done along with a test that measures fetal nuchal translucency. With this test, doctors use ultrasonography to look at a fluid-filled space near the back of the fetus’s neck).
Testing for Neural Tube Defects
The alpha-fetoprotein level in blood is usually measured in all pregnant women, if other testing did not include this marker (eg, some first-trimester serum marker options, chorionic villus sampling, or amniocentesis). A high level may indicate an increased risk of having
A baby with a neural tube defect of the brain (such as anencephaly) or spinal cord (such as spina bifida)
The alpha-fetoprotein level may also be elevated for other reasons, including
A baby with a birth defect of the abdominal wall
Later pregnancy complications, such as miscarriage, or a newborn who is small for gestational age (small for how long the pregnancy has lasted), or death of the fetus
Ultrasonography is done if blood tests detect an abnormal alpha-fetoprotein level in a pregnant woman.
Amniocentesis is an invasive test done if further testing is needed. It enables doctors to measure the alpha-fetoprotein level in the fluid that surrounds the fetus (amniotic fluid), to analyze the fetus’s chromosomes, and to determine whether the amniotic fluid contains an enzyme called acetylcholinesterase. Knowing what the alpha-fetoprotein level is and whether acetylcholinesterase is present helps doctors better assess risk for a neural tube defect or other abnormality.
A high alpha-fetoprotein level or the presence of acetylcholinesterase in the amniotic fluid suggests
A neural tube defect
An abnormality in another structure, such as the esophagus, kidneys, or abdominal wall
A high alpha-fetoprotein level plus acetylcholinesterase in the amniotic fluid indicates a high risk of
A neural tube defect, such as anencephaly or spina bifida
Ultrasonography
Ultrasonography is commonly done as a routine test during pregnancy. It has no known risks for the woman or fetus. Ultrasonography can do the following:
Indicate whether the fetus is alive
Determine if more than one fetus is present
Confirm the age of the fetus (gestational age)
Locate the placenta
In the second trimester, detect certain obvious structural birth defects, including those of the brain, spinal cord, heart, kidneys, stomach, abdominal wall, and bones, some of which may indicate an increased risk of a chromosomal abnormality in the fetus

If a pregnant woman has abnormal results on a prenatal blood test or a family history of birth defects (such as heart birth defects or cleft lip and palate), ultrasonography can be done to evaluate the fetus. However, normal results do not guarantee the fetus has no abnormalities, because not all abnormalities can be detected. Certain conditions, such as neural tube defects, are still possible. Results of ultrasonography may suggest chromosomal abnormalities in the fetus, but ultrasonography cannot identify the specific problem. In such cases, amniocentesis may be recommended.
Targeted ultrasonography using high-resolution equipment can be done at some specialized centers. It provides more detail and may be more accurate than standard ultrasonography, particularly for small birth defects. Targeted ultrasonography done during the second trimester can help estimate the risk of a chromosomal abnormality. Targeted ultrasonography aims to identify certain structural birth defects that indicate an increased risk of a chromosomal abnormality. This test can also detect certain variations in organs that do not affect function but may indicate an increased risk of a chromosomal abnormality. However, normal results do not necessarily mean that there is no risk of a chromosomal abnormality.
Invasive Tests for Prenatal Diagnosis
Several procedures can be used to directly test fetal genetic material for genetic and chromosomal abnormalities. These tests are invasive (that is, they require insertion of an instrument into the body) and have a slight risk of miscarriage or harm to the fetus.
Amniocentesis
One of the most common procedures for detecting abnormalities before birth is amniocentesis. It is often offered to women over age 35 because they have a higher risk of having a fetus with chromosomal abnormalities than younger women. However, many doctors offer this test to all pregnant women, and any pregnant woman can request it, even if her risk is not higher than normal.
In this procedure, a sample of the fluid that surrounds the fetus (amniotic fluid) is removed and analyzed. Amniocentesis is usually done at 15 weeks of pregnancy or later. The fluid contains cells that have been shed by the fetus. These cells are grown in a laboratory so that the chromosomes in them can be analyzed. Amniocentesis enables doctors to measure the level of alpha-fetoprotein (a protein produced by the fetus) in the amniotic fluid. This measurement more reliably indicates whether the fetus has a brain or spinal cord defect than does measurement of this level in the woman’s blood.
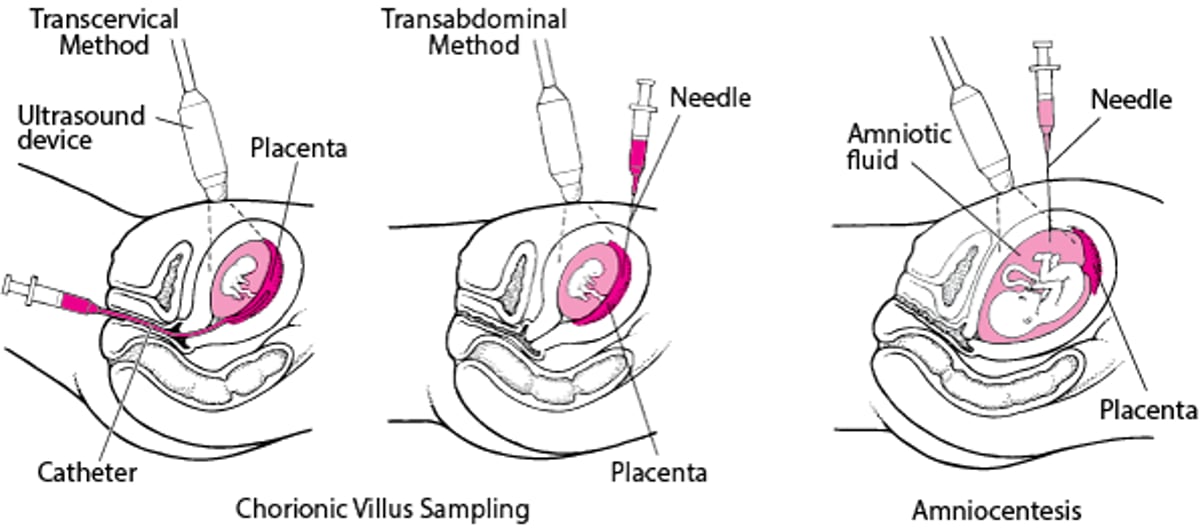
Detecting Abnormalities Before Birth
Chorionic villus sampling and amniocentesis are used to detect abnormalities in a fetus. During both procedures, ultrasonography is used for guidance. In chorionic villus sampling, a sample of chorionic villi (part of the placenta) is removed by one of two methods. In the transcervical method, a doctor inserts a thin, flexible tube (catheter) through the vagina and cervix into the placenta. In the transabdominal method, a doctor inserts a needle through the abdominal wall into the placenta. In both methods, a sample of the placenta is suctioned out with a syringe and analyzed. In amniocentesis, a doctor inserts a needle through the abdominal wall into the amniotic fluid. A sample of fluid is withdrawn for analysis. |

Before the procedure, ultrasonography is done to evaluate the heart of the fetus, to confirm the length of the pregnancy, to locate the placenta and amniotic fluid, and to determine how many fetuses are present.
A doctor inserts a needle through the abdominal wall into the amniotic fluid. Sometimes a local anesthetic is first used to numb the site. During the procedure, ultrasonography is done so that the fetus can be monitored and the needle can be guided into place. Fluid is withdrawn, and the needle is removed.
Occasionally, the amniotic fluid contains blood from the fetus. Such blood may increase the alpha-fetoprotein level, making the results hard to interpret.
If women have Rh-negative blood, they are given Rho(D) immune globulin after the procedure to prevent them from producing antibodies to Rh factor. When a woman with Rh-negative blood has a fetus with Rh-positive blood (called Rh incompatibility), she may produce these antibodies if the fetus's blood comes into contact with her blood, as it may during amniocentesis. These antibodies can cause problems in a fetus with Rh-positive blood. The injection is not needed if the father also has Rh-negative blood because in such cases, the fetus always has Rh-negative blood.
Amniocentesis rarely causes any problems for the woman or the fetus. The following may occur:
Soreness: Some women feel slightly sore for an hour or two afterward.
Spotting of blood or leakage of amniotic fluid from the vagina: About 1 to 2% of the women have these problems, but the problems do not last long and usually stop without treatment.
Miscarriage: The chance of miscarriage due to amniocentesis is about 1 in 500 to 1,000.
Needle injuries to the fetus: These injuries are very rare.
Amniocentesis can usually be done when a woman is pregnant with twins or even more fetuses.
Chorionic Villus Sampling
In chorionic villus sampling, a doctor removes a small sample of the chorionic villi, which are tiny projections that make up part of the placenta. This procedure is used to diagnose some disorders in the fetus, usually between 10 and 12 weeks of pregnancy.
Unlike amniocentesis, chorionic villus sampling does not enable doctors to obtain a sample of amniotic fluid. Consequently, doctors cannot measure the alpha-fetoprotein level in amniotic fluid to check for brain and spinal cord defects (neural tube defects). Doctors may suggest that amniocentesis or blood tests to measure alpha-fetoprotein be done later in the pregnancy to check for these defects.
The main advantage of chorionic villus sampling is that its results are available much earlier in the pregnancy than those of amniocentesis. Thus, if no abnormality is detected, the couple’s anxiety can be relieved earlier. If an abnormality is detected earlier and if the couple decides to terminate the pregnancy, simpler, safer methods can be used. Also, early detection of an abnormality may give the couple more time to prepare for the birth of a child with special medical needs.
Before chorionic villus sampling, ultrasonography is done to determine whether the fetus is alive, to confirm the length of the pregnancy, to check for obvious abnormalities, and to locate the placenta.
A sample of the chorionic villi can be removed through the cervix (transcervically) or the abdominal wall (transabdominally).
Through the cervix: The woman lies on her back with her hips and knees bent, usually supported by heel or knee stirrups, as for a pelvic examination. The doctor inserts a thin, flexible tube (catheter) through the vagina and cervix into the placenta. For most women, the procedure feels very similar to a Papanicolaou (Pap) test, but a few women find it more uncomfortable. This method cannot be used in women who have an active genital infection (such as genital herpes or gonorrhea).
Through the abdominal wall: The doctor anesthetizes an area of skin over the abdomen and inserts a needle through the abdominal wall into the placenta. Most women do not find this procedure painful. But for some women, the area over the abdomen feels slightly sore for an hour or two afterward.
For both procedures, doctors use ultrasonography to guide them as they insert the catheter or needle and suction out the tissue sample with a syringe. The sample is then sent for analysis. Many women have light spotting for a day or two after either of these procedures.
After chorionic villus sampling, women who have Rh-negative blood and who do not have antibodies to Rh factor are given an injection of Rho(D) immune globulin to prevent them from producing antibodies to Rh factor. When a woman with Rh-negative blood has a fetus with Rh-positive blood (called Rh incompatibility), she may produce these antibodies if the fetus's blood comes into contact with her blood, as it may during chorionic villus sampling. These antibodies can cause problems in the fetus. The injection is not needed if the father also has Rh-negative blood because in such cases, the fetus always has Rh-negative blood.
The risks of chorionic villus sampling are comparable to those of amniocentesis. The most common risk is that of miscarriage, which occurs in about 1 in 500 procedures.
Rarely, the genetic diagnosis is unclear after chorionic villus sampling, and amniocentesis may be necessary. In general, the accuracy of the two procedures is comparable.
Percutaneous Umbilical Blood Sampling
In percutaneous (through the skin) umbilical blood sampling, the doctor first anesthetizes an area of skin over the abdomen. Guided by ultrasonography, the doctor then inserts a needle through the abdominal wall and uterus into the umbilical cord. A sample of the fetus’s blood is withdrawn and analyzed, and the needle is removed. Percutaneous umbilical blood sampling is an invasive procedure. It may cause miscarriage in about 1 in 100 procedures.
In the past, percutaneous umbilical blood sampling was used when rapid chromosome analysis was needed, particularly toward the end of pregnancy when ultrasonography detected abnormalities in the fetus. However, this procedure is now rarely used for this purpose. Instead, doctors analyze the genes in amniotic fluid cells (obtained during amniocentesis), or they analyze part of the placenta (obtained during chorionic villus sampling). These tests are less dangerous and provide results more quickly.
Currently, percutaneous umbilical blood sampling is occasionally done when doctors suspect that a fetus has anemia. If the fetus has severe anemia, blood can be transfused to the fetus through the needle while it is still inserted in the umbilical cord.
Preimplantation Genetic Testing
If pregnancy is to be achieved using in vitro (test tube) fertilization, doctors can sometimes diagnose genetic disorders in the embryo before it is transferred to the woman’s uterus. Preimplantation genetic testing requires technical expertise and is expensive. These tests are used mainly for prospective parents with a high risk of having a baby with certain genetic disorders (such as cystic fibrosis) or chromosomal abnormalities. However, newer techniques may reduce costs and make the tests more widely available.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American College of Obstetricians and Gynecologists: Genetic Disorders: This website provides definitions of genes and chromosomes and basic information about inheritance, risk of having a baby with a birth defect, and testing for genetic and chromosomal abnormalities.






