


The standard electrocardiogram (ECG) provides 12 different vector views of the heart’s electrical activity as reflected by electrical potential differences between positive and negative electrodes placed on the limbs and chest wall. Six of these views are vertical (using frontal leads I, II, and III and limb leads aVR, aVL, and aVF), and 6 are horizontal (using precordial leads V1, V2, V3, V4, V5, and V6). The 12-lead ECG is crucial for establishing many cardiac diagnoses (see table Interpretation of Abnormal ECGs), including
Atrial enlargement
Conditions that predispose to syncope or sudden death (eg, Brugada syndrome, long QT syndrome, Wolff-Parkinson-White syndrome)
Myocardial ischemia
Ventricular hypertrophy (see table Criteria for ECG Diagnosis of Left Ventricular Hypertrophy)
For more information on ECG interpretation, see Overview of Arrhythmias and ECG in Acute Coronary Syndromes. A useful ECG tutorial is available from the University of Utah.
Standard ECG Components
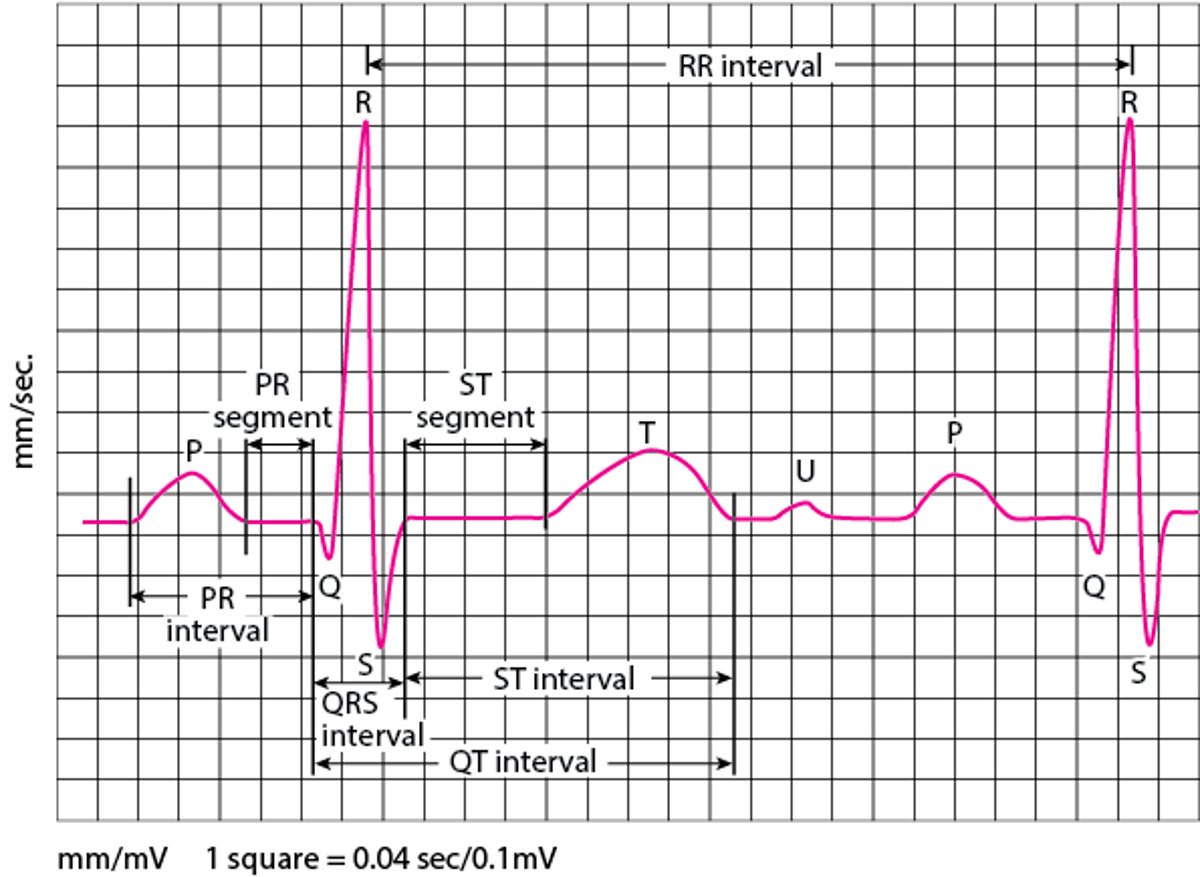
By convention, the ECG tracing is divided into the P wave, PR interval, QRS complex, QT interval, ST segment, T wave, and U wave (see figure ECG waves).
Electrocardiography (ECG) waves
P wave = activation (depolarization) of atria. PR interval =time interval between onset of atrial depolarization and onset of ventricular depolarization. QRS complex = depolarization of ventricles, consisting of the Q, R, and S waves. QT interval = time interval between onset of ventricular depolarization and end of ventricular repolarization. R-R interval = time interval between 2 QRS complexes. T wave = ventricular repolarization. ST segment plus T wave (ST-T) = ventricular repolarization. U wave = probably after-depolarization (relaxation) of ventricles. |

P wave
The P wave represents atrial depolarization. It is upright in most leads except aVR. It may be biphasic in leads II and V1; the initial component represents right atrial activity, and the 2nd component represents left atrial activity.
An increase in amplitude of either or both components occurs with atrial enlargement. Right atrial enlargement produces a P wave > 2 mm in leads II, III, and aVF (P pulmonale); left atrial enlargement produces a P wave that is broad and double-peaked in lead II (P mitrale). Normally, the P axis is between 0° and 75°.
PR interval
The PR interval is the time between onset of atrial depolarization and onset of ventricular depolarization. Normally, it is 0.10 to 0.20 second; prolongation defines 1st-degree atrioventricular block.
QRS complex
The QRS complex represents ventricular depolarization.
The Q wave is the initial downward deflection; normal Q waves last < 0.05 second in all leads except V1 to V3, in which any Q wave is considered abnormal, indicating past or current infarction.
The R wave is the first upward deflection; criteria for normal height or size are not absolute, but taller R waves may be caused by ventricular hypertrophy. A 2nd upward deflection in a QRS complex is designated R′.
The S wave is the 2nd downward deflection if there is a Q wave and the first downward deflection if not.
The QRS complex may be R alone, QS (no R), QR (no S), RS (no Q), or RSR′, depending on the ECG lead, vector, and presence of heart disorders.
Normally, the QRS interval is 0.07 to 0.10 second. An interval of 0.10 to 0.11 second is considered incomplete bundle branch block or a nonspecific intraventricular conduction delay, depending on QRS morphology. An interval ≥ 0.12 second is considered complete bundle branch block or an intraventricular conduction delay.
Normally, the QRS axis is 90° to −30°. An axis of −30° to −90° is considered left axis deviation and occurs in left anterior fascicular block (−60°) and inferior myocardial infarction.
An axis of 90° to 180° is considered right axis deviation; it occurs in any condition that increases pulmonary pressures and causes right ventricular hypertrophy (cor pulmonale, acute pulmonary embolism, pulmonary hypertension), and it sometimes occurs in right bundle branch block or left posterior fascicular block.
QT interval
The QT interval is the time between onset of ventricular depolarization and end of ventricular repolarization. The QT interval must be corrected for heart rate using the formula:


where QTc is the corrected QT interval and R-R interval is the time between 2 QRS complexes. All intervals are recorded in seconds. Normal range of QTc in adults is 350 to 450 msec in men and 360 to 460 msec in women. QTc prolongation is strongly implicated in development of torsades de pointe ventricular tachycardia. QTc is often difficult to calculate because the end of the T wave is often unclear or followed by a U wave with which it merges. Numerous drugs are implicated in prolonging the QT interval (see CredibleMeds).
ST segment
The ST segment represents completed ventricular myocardial depolarization. Normally, it is horizontal along the baseline of the PR (or TP) intervals or slightly off baseline.
ST segment elevation can be caused by
Early repolarization
Left ventricular hypertrophy
Myocardial ischemia and infarction
Left ventricular aneurysm
Pericarditis
Hyperkalemia
Hypothermia
Pulmonary embolism
ST segment depression can be caused by
Hypokalemia
Subendocardial ischemia
Reciprocal changes in acute myocardial infarction
T wave
The T wave reflects ventricular repolarization. It usually takes the same direction as the QRS complex (concordance); opposite polarity (discordance) may indicate past or current infarction. The T wave is usually smooth and rounded but may be of low amplitude in hypokalemia and hypomagnesemia and may be tall and peaked in hyperkalemia, hypocalcemia, and left ventricular hypertrophy.
U wave
The U wave appears commonly in patients who have hypokalemia, hypomagnesemia, or ischemia. It is often present in healthy people.
Specialized ECG Tests
A standard 12-lead ECG represents only a single brief period of cardiac activity; enhanced techniques can provide additional information.
Additional precordial leads
Additional precordial leads are used to help diagnose
Right ventricular infarction
Posterior wall infarction
Right-sided leads are placed across the right side of the chest to mirror standard left-sided leads. They are labeled V1R to V6R; sometimes only V4R is used, because it is the most sensitive for right ventricular myocardial infarction.
Additional left-sided leads can be placed in the 5th intercostal space, with V7 at the posterior axillary line, V8 at the midscapular line, and V9 at the left border of the spine. These leads are rarely used but may help diagnose a true posterior myocardial infarction.
Esophageal lead
An esophageal lead is much closer to the atria than surface leads; it is an option when the presence of P waves on a standard recording is uncertain and when detecting atrial electrical activity is important, as when atrial or ventricular origin of wide-complex tachycardia must be differentiated or when atrioventricular dissociation is suspected. An esophageal lead may also be used to monitor intraoperative myocardial ischemia or to detect atrial activity during cardioplegia. The lead is placed by having the patient swallow an electrode, which is then connected to a standard ECG machine, often in the lead II port.
Signal averaging
Signal averaging of QRS waveforms creates a digital composite of several hundred cardiac cycles to detect high-frequency, low-amplitude potentials and microcurrents at the terminal part of the QRS complex. These findings represent areas of slow conduction through abnormal myocardium, indicating increased risk of reentrant ventricular tachycardia.
Signal-averaged ECG is still largely a research technique but is occasionally used to assess risk of sudden cardiac death (eg, in patients with known significant heart disease). It seems most useful in identifying patients at low risk of sudden death. Its value for identifying patients at high risk of sudden death has not been established.
Signal averaging is also being investigated in various other cardiac disorders, ranging from the post-myocardial infarction state and cardiomyopathies to Brugada syndrome and ventricular aneurysms, and to assess efficacy of surgery to correct the arrhythmia. This technique may also be useful for assessing the proarrhythmic effects of antiarrhythmic drugs and for detecting rejection of heart transplants.
Signal averaging of P waves is being studied as a way to identify patients at risk of atrial fibrillation.
Continuous ST-segment monitoring
This type of monitoring is used for early detection of ischemia and serious arrhythmias. Monitoring can be automated (dedicated electronic monitoring units are available) or done clinically using serial ECGs. Applications include emergency department monitoring of patients with crescendo angina, evaluation after percutaneous intervention, intraoperative monitoring, and postoperative care.
QT dispersion
QT dispersion (the difference between the longest and shortest QT intervals on a 12-lead ECG) has been proposed as a measure of myocardial repolarization heterogeneity. Increased dispersion (≥ 100 millisecond) suggests electrically heterogeneous myocardium caused by ischemia or fibrosis, with increased risk of reentrant arrhythmias and sudden death. QT dispersion predicts mortality risk but is not widely measured because measurement error is common, values in patients with and without disease overlap substantially, there is no reference standard, and other validated risk predictors are available.
Heart rate variability
This measurement reflects the balance between sympathetic and parasympathetic (vagal) input to the heart. Decreased variability suggests decreased vagal input and increased sympathetic input, which predict increased risk of arrhythmias and mortality. The most common measure of variability is the mean of the standard deviations of all normal R-R intervals in a 24-hour ECG recording.
Heart rate variability is used primarily in research. Evidence suggests that it provides useful information about left ventricular dysfunction after myocardial infarction, heart failure, and hypertrophic cardiomyopathy. Most Holter monitors have software that measures and analyzes heart rate variability, but clinical utility is currently uncertain.
Holter monitor
Holter monitoring is continuous monitoring and recording of the ECG for 24 to 48 hours. It is useful for evaluating intermittent arrhythmias and, secondarily, for detecting hypertension. The Holter monitor is portable, enabling patients to participate in normal daily activities; it may also be used for sedentary hospitalized patients if automated monitoring is unavailable. Patients are asked to record symptoms and activities so that they may be correlated with events on the monitor. The Holter monitor does not automatically analyze the ECG data; a physician does so at a later date.
Event recorder
Event recorders are worn for up to 30 days and can detect infrequent rhythm disturbances that 24-hour Holter monitoring may miss. The recorder may operate continuously or also be activated by the patient when symptoms occur. A memory loop enables information to be stored for seconds or minutes before and after activation. The patient can transmit ECG data by telephone or satellite to be read by a physician; some recorders automatically transmit serious events. If patients have serious events (eg, syncope) at intervals of > 30 days, an event recorder may be placed subcutaneously (implantable loop recorder); it can be activated by a small magnet. Battery life for subcutaneous recorders is several years.
Wireless adhesive monitor
Another option for single-channel rhythm monitoring is a small, adhesive, water-resistant, wireless, and disposable device worn on the chest. One type of this device continuously records cardiac rhythms for up to 2 weeks. Another similar device functions as an event recorder; a patient pushes a button on the device when experiencing any potential arrhythmia-related symptoms (eg, palpitations, dizziness) to record stored ECG data 45 seconds before the event plus 15 seconds after the event. However, unlike with event recorders, automated, real-time reporting is not available.
Smartwatches with ECG capability
Several consumer smartwatches take ECG measurements from the wrist. Smartwatches have the potential to detect arrhythmias in real time, and their usefulness in this area is under investigation.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
University of Utah ECG Learning Center: Provides an interactive tutorial on clinical electrocardiography
CredibleMeds QTDrugs List: Provides information on drugs that are known or suspected to increase the risk of ventricular arrhythmias






