


Mechanical ventilation can be
Noninvasive, involving various types of face masks
Invasive, involving endotracheal intubation
Selection and use of appropriate techniques require an understanding of respiratory mechanics.
Indications
There are numerous indications for endotracheal intubation and mechanical ventilation (see table Situations Requiring Airway Control ), but, in general, mechanical ventilation should be considered when there are clinical or laboratory signs that the patient cannot maintain an airway or adequate oxygenation or ventilation.
Concerning findings include
Respiratory rate > 30/minute
Inability to maintain arterial oxygen saturation > 90% with fractional inspired oxygen (FIO2) > 0.60
pH < 7.25
Partial pressure of carbon dioxide (PaCO2) > 50 mm Hg (unless chronic and stable)
The decision to initiate mechanical ventilation should be based on clinical judgment that considers the entire clinical situation and not simple numeric criteria. However, mechanical ventilation should not be delayed until the patient is in extremis.
Respiratory Mechanics
Normal inspiration generates negative intrapleural pressure, which creates a pressure gradient between the atmosphere and the alveoli, resulting in air inflow. In mechanical ventilation, the pressure gradient results from increased (positive) pressure of the air source.
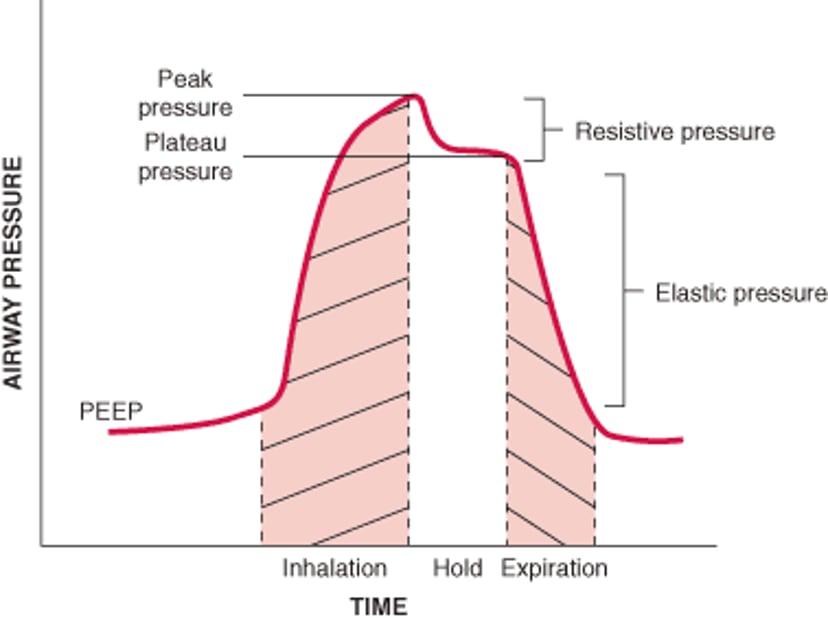
Peak airway pressure is measured at the airway opening (Pao) and is routinely displayed by mechanical ventilators. It represents the total pressure needed to push a volume of gas into the lung and is composed of pressures resulting from inspiratory flow resistance (resistive pressure), the elastic recoil of the lung and chest wall (elastic pressure), and the alveolar pressure present at the beginning of the breath (positive end-expiratory pressure [PEEP]—see figure Components of airway pressure). Thus,

Resistive pressure is the product of circuit resistance and airflow. In the mechanically ventilated patient, resistance to airflow occurs in the ventilator circuit, the endotracheal tube, and, most importantly, the patient’s airways. (NOTE: Even when these factors are constant, an increase in airflow increases resistive pressure.)
Components of airway pressure during mechanical ventilation, illustrated by an inspiratory-hold maneuver
PEEP = positive end-expiratory pressure. |

Elastic pressure is the product of the elastic recoil of the lungs and chest wall (elastance) and the volume of gas delivered. For a given volume, elastic pressure is increased by increased lung stiffness (as in pulmonary fibrosis) or restricted excursion of the chest wall or diaphragm (as in tense ascites or massive obesity). Because elastance is the inverse of compliance, high elastance is the same as low compliance.
End-expiratory pressure in the alveoli is normally the same as atmospheric pressure. However, when the alveoli fail to empty completely because of airway obstruction, airflow limitation, or shortened expiratory time, end-expiratory pressure may be positive relative to the atmosphere. This pressure is called intrinsic PEEP or autoPEEP to differentiate it from externally applied (therapeutic) PEEP, which is created by adjusting the mechanical ventilator or by placing a tight-fitting mask that applies positive pressure throughout the respiratory cycle.
Any elevation in peak airway pressure (eg, > 25 cm H2O) should prompt measurement of the end-inspiratory pressure (plateau pressure) by an end-inspiratory hold maneuver to determine the relative contributions of resistive and elastic pressures. The maneuver keeps the exhalation valve closed for an additional 0.3 to 0.5 second after inspiration, delaying exhalation. During this time, airway pressure falls from its peak value as airflow ceases. The resulting end-inspiratory pressure represents the elastic pressure once PEEP is subtracted (assuming the patient is not making active inspiratory or expiratory muscle contractions at the time of measurement). The difference between peak and plateau pressure is the resistive pressure.
Elevated resistive pressure (eg, > 10 cm H2O) suggests that the endotracheal tube has been kinked or plugged with secretions or that an intraluminal mass or bronchospasm is present.
Increased elastic pressure (eg, > 10 cm H2O) suggests decreased lung compliance due to
Edema, fibrosis, or lobar atelectasis
Large pleural effusions, pneumothorax, or fibrothorax
Extrapulmonary restriction as may result from circumferential burns or another chest wall deformity, ascites, pregnancy, or massive obesity
A tidal volume too large for the amount of lung being ventilated (eg, a normal tidal volume being delivered to a single lung because the endotracheal tube is malpositioned)
Intrinsic PEEP (auto PEEP) can be measured in the passive patient through an end-expiratory hold maneuver. Immediately before a breath, the expiratory port is closed for 2 seconds. Flow ceases, eliminating resistive pressure; the resulting pressure reflects alveolar pressure at the end of expiration (intrinsic PEEP). Although accurate measurement depends on the patient being completely passive on the ventilator, it is unwarranted to use neuromuscular blockade solely for the purpose of measuring intrinsic PEEP. A nonquantitative method of identifying intrinsic PEEP is to inspect the expiratory flow tracing. If expiratory flow continues until the next breath or the patient’s chest fails to come to rest before the next breath, intrinsic PEEP is present. The consequences of elevated intrinsic PEEP include increased inspiratory work of breathing and decreased venous return, which may result in decreased cardiac output and hypotension.
The demonstration of intrinsic PEEP should prompt a search for causes of airflow obstruction (eg, airway secretions, decreased elastic recoil, bronchospasm); however, a high minute ventilation (> 20 L/minute) alone can result in intrinsic PEEP in a patient with no airflow obstruction. If the cause is airflow limitation, intrinsic PEEP can be reduced by shortening inspiratory time (ie, increasing inspiratory flow) or reducing the respiratory rate, thereby allowing a greater fraction of the respiratory cycle to be spent in exhalation.
Means and Modes of Mechanical Ventilation
Mechanical ventilators are
Volume cycled: Delivering a constant volume with each breath (pressures may vary)
Pressure cycled: Delivering constant pressure during each breath (volume delivered may vary)
A combination of volume and pressure cycled
Assist-control (A/C) modes of ventilation are modes that maintain a minimum respiratory rate regardless of whether or not the patient initiates a spontaneous breath. Because pressures and volumes are directly linked by the pressure-volume curve, any given volume will correspond to a specific pressure, and vice versa, regardless of whether the ventilator is pressure cycled or volume cycled.
Adjustable ventilator settings differ with mode but include
Respiratory rate
Tidal volume
Trigger sensitivity
Flow rate
Waveform
Inspiratory/expiratory (I/E) ratio
Volume-cycled ventilation
Volume-cycled ventilation delivers a set tidal volume. This mode includes
Volume-control (V/C)
Synchronized intermittent mandatory ventilation (SIMV)
The resultant airway pressure is not fixed but varies with the resistance and elastance of the respiratory system and with the flow rate selected.
V/C ventilation is the simplest and most effective means of providing full mechanical ventilation. In this mode, each inspiratory effort beyond the set sensitivity threshold triggers delivery of the fixed tidal volume. If the patient does not trigger the ventilator frequently enough, the ventilator initiates a breath, ensuring the desired minimum respiratory rate.
SIMV also delivers breaths at a set rate and volume that is synchronized to the patient’s efforts. In contrast to V/C, patient efforts above the set respiratory rate are unassisted, although the intake valve opens to allow the breath. This mode remains popular, despite studies indicating that it does not provide full ventilator support as does V/C, does not facilitate liberation of the patient from mechanical ventilation, and does not improve patient comfort.
Pressure-cycled ventilation
Pressure-cycled ventilation delivers a set inspiratory pressure. This mode includes
Pressure control ventilation (PCV)
Pressure support ventilation (PSV)
Noninvasive modalities applied via a tight-fitting face mask (several types available)
Hence, tidal volume varies depending on the resistance and elastance of the respiratory system. In this mode, changes in respiratory system mechanics can result in unrecognized changes in alveolar ventilation. Because it limits the distending pressure of the lungs, this mode can theoretically benefit patients with acute respiratory distress syndrome (ARDS); however, no clear clinical advantage over V/C has been shown, and, if the volume delivered by PCV is the same as that delivered by V/C, the distending pressures will be the same.
Pressure control ventilation is a pressure-cycled form of A/C. Each inspiratory effort beyond the set sensitivity threshold delivers full pressure support maintained for a fixed inspiratory time. A minimum respiratory rate is maintained.
In pressure support ventilation, a minimum rate is not set; all breaths are triggered by the patient. The ventilator assists the patient by delivering a pressure that continues at a constant level until the patient's inspiratory flow falls below a preset level determined by an algorithm. Thus, a longer or deeper inspiratory effort by the patient results in a larger tidal volume. This mode is commonly used to liberate patients from mechanical ventilation by letting them assume more of the work of breathing. However, no studies indicate that this approach is more successful than others in discontinuing mechanical ventilation.
Noninvasive positive pressure ventilation (NIPPV)
NIPPV is the delivery of positive pressure ventilation via a tight-fitting mask that covers the nose or both the nose and mouth. Helmets that deliver NIPPV are an alternative for patients who cannot tolerate the standard tight-fitting face masks. Because of its use in spontaneously breathing patients, NIPPV is primarily applied as a form of pressure support ventilation or to deliver end-expiratory pressure, although volume control can be used. (See also How To Do Noninvasive Positive Pressure Ventilation.)
NIPPV can be given as
Continuous positive airway pressure (CPAP)
Bilevel positive airway pressure (BiPAP)
In CPAP, constant pressure is maintained throughout the respiratory cycle with no additional inspiratory support.
With BiPAP, the physician sets both the expiratory positive airway pressure (EPAP) and the inspiratory positive airway pressure (IPAP), with respirations triggered by the patient.
In either mode, because the airway is unprotected, aspiration is possible, so patients must have adequate mentation and airway protective reflexes and no imminent indication for surgery or transport off the floor for prolonged procedures. Obtunded patients and patients with copious secretions are not good candidates. NIPPV also should be avoided in patients who are hemodynamically unstable and in those with evidence of impaired gastric emptying, as occurs with ileus, bowel obstruction, or pregnancy. In such circumstances, swallowing large quantities of air may result in vomiting and life-threatening aspiration. Also, IPAP must be set below esophageal opening pressure (20 cm H2O) to avoid gastric insufflation.
Indications for conversion to endotracheal intubation and conventional mechanical ventilation include the development of shock or frequent arrhythmias, myocardial ischemia, and transport to a cardiac catheterization laboratory or surgical suite where control of the airway and full ventilatory support are desired.
NIPPV can be used in the outpatient setting. For example, CPAP is often used for patients with obstructive sleep apnea, whereas BiPAP can be used for those with concomitant obesity-hypoventilation syndrome or for chronic ventilation in patients with neuromuscular or chest wall diseases.
Ventilator settings
Ventilator settings are tailored to the underlying condition, but the basic principles are as follows.
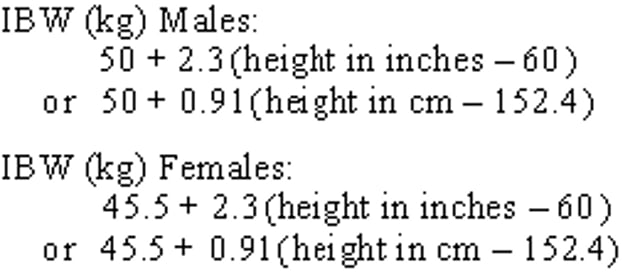
Tidal volume and respiratory rate set the minute ventilation. Too high a volume risks overinflation; too low a volume allows for atelectasis. Too high a rate risks hyperventilation and respiratory alkalosis along with inadequate expiratory time and autoPEEP; too low a rate risks inadequate minute ventilation and respiratory acidosis. A low tidal volume of 6 to 8 mL/kg ideal body weight (IBW) was initially recommended for patients with acute respiratory distress syndrome (ARDS—see sidebar Initial Ventilator Management in ARDS); however, such low tidal volume is usually also appropriate in certain patients who have normal lung mechanics (1, 2, 3), such as those who are on mechanical ventilation during surgery (4, 5). Other patients (eg, those with trauma, obtundation, severe acidosis) may be started at slightly higher tidal volume (eg, 8 to 10 mL/kg). IBW rather than actual body weight is used to determine the appropriate tidal volume for patients who have lung disease and who are receiving mechanical ventilation:

Sensitivity adjusts the level of negative pressure required to trigger the ventilator. A typical setting is –2 cm H2O. Too high a setting (eg, more negative than –2 cm H2O) causes weak patients to be unable to trigger a breath. Too low a setting (eg, less negative than –2 cm H2O) may lead to overventilation by causing the machine to auto-cycle. Patients with high levels of autoPEEP (eg, those with COPD, asthma) may have difficulty inhaling deeply enough to achieve a sufficiently negative intra-airway pressure.
The I:E ratio (inspiratory:expiratory ratio) is the ratio of time spent in inhalation versus that spent in exhalation. The I:E ratio can be adjusted in some modes of ventilation. A normal setting for patients with normal mechanics is 1:3. Patients with asthma or exacerbations of COPD (chronic obstructive pulmonary disease) should have ratios of 1:4 or even more to limit the degree of autoPEEP.
The inspiratory flow rate can be adjusted in some modes of ventilation (ie, either the flow rate or the I:E ratio can be adjusted, not both). The inspiratory flow should generally be set at about 60 L/minute but can be increased up to 120 L/minute for patients with airflow limitation to facilitate having more time in exhalation, thereby limiting autoPEEP.
FIO2 (fraction of inspired oxygen) is initially set at 1.0 (100% oxygen) and is subsequently decreased to the lowest level necessary to maintain adequate oxygenation.
PEEP can be applied in any ventilator mode. PEEP increases end-expired lung volume and reduces airspace closure at the end of expiration. Most patients undergoing mechanical ventilation may benefit from the application of PEEP at 5 cm H2O to limit the atelectasis that frequently accompanies endotracheal intubation, sedation, paralysis, and/or supine positioning. Higher levels of PEEP improve oxygenation in disorders such as cardiogenic pulmonary edema and ARDS. PEEP permits use of lower levels of FIO2 while preserving adequate arterial oxygenation. This effect may be important in limiting the lung injury that may result from prolonged exposure to a high FIO2 (≥ 0.6). However, if PEEP increases intrathoracic pressure and if too high may impede venous return, provoking hypotension in a hypovolemic patient, may reduce left ventricular afterload, and may overdistend portions of the lung, thereby causing ventilator-associated lung injury (VALI). By contrast, if PEEP is too low, it may result in cyclic airspace opening and closing, which in turn may also cause VALI due to the resultant repetitive shear forces. It is important to keep in mind that the pressure-volume curve varies for different regions of the lung. This variation means that, for a given PEEP, the increase in volume will be lower for dependent regions compared to nondependent regions of the lung.
Ventilator settings references
1. Serpa Neto A, Cardoso SO, Manetta JA, et al: Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: A meta-analysis. JAMA 308:1651–1659, 2012. doi: 10.1001/jama.2012.13730
2. Guay J, Ochroch EA, Kopp S: Intraoperative use of low volume ventilation to decrease postoperative mortality, mechanical ventilation, lengths of stay and lung injury in adults without acute lung injury. Cochrane Database Syst Rev Jul; 2018(7): CD011151, 2018. doi: 10.1002/14651858.CD011151.pub3
3. Neto AS, Simonis FD, Barbas CS, et al: Lung-protective ventilation with low tidal volumes and the occurrence of pulmonary complications in patients without acute respiratory distress syndrome: A systematic review and individual patient data analysis. Crit Care Med 43:2155–2163, 2015. doi: 10.1097/CCM.0000000000001189
4. Futier E, Constantin JM, Paugam-Burtz C, et al: A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med 369:428–437, 2013. doi: 10.1056/NEJMoa1301082
5. Yang M, Ahn HJ, Kim K, et al: Does a protective ventilation strategy reduce the risk of pulmonary complications after lung cancer surgery? A randomized controlled trial. Chest 139:530–537, 2011. doi: 10.1378/chest.09-2293
Patient positioning
Mechanical ventilation is typically done with the patient in the supine, semiupright position. However, in patients with ARDS, prone positioning may result in better oxygenation, primarily by creating more uniform ventilation. Uniform ventilation reduces the amount of lung that has no ventilation (ie, the amount of shunt), which is generally greatest in the dorsal and caudal lung regions, while having minimal effects on perfusion distribution.
Although many investigators advocate a trial of prone positioning in patients with ARDS who require high levels of PEEP (eg, > 12 cm H2O) and FIO2 (eg, > 0.6), initial trials did not show any decrease in mortality with this strategy (however, these trials were underpowered and had other study design issues). A subsequent large, multicenter, prospective trial (1) assessed patients who had moderately severe ARDS (PaO2:FIO2 < 150 mm Hg on an FIO2 ≥ 0.6, PEEP > 5 cm H2O) and who were on a tidal volume of about 6 mL/kg. These patients were randomized to undergo ≥ 16 hours of prone positioning or be left in the supine position during ventilation. The study, which included a total of 466 patients, identified lower 28- and 90-day mortality in the prone-positioning group without a significant incidence of associated complications. Improvements in patient selection and management protocols are thought to account for the better results compared to earlier studies (2).
Prone positioning in awake, spontaneously breathing, hypoxemic patients with COVID-19 on high-flow nasal cannula oxygen decreased hypoxemia and in one large clinical trial reduced the risk of treatment failure defined as need for intubation or death within 28 days (3).
Prone positioning is contraindicated in patients with spinal instability or increased intracranial pressure. This position also requires careful attention by the intensive care unit staff to avoid complications, such as dislodgement of the endotracheal tube or intravascular catheters.
Patient positioning references
1. Guérin C, Reignier J, Richard JC, et al: Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 368(23):2159–2168, 2013. doi: 10.1056/NEJMoa1214103.
2. Scholten EL, Beitler JR, Prisk GK, et al: Treatment of ARDS with prone positioning. Chest 151:215–224, 2017. doi: 10.1016/j.chest.2016.06.032. Epub 2016 Jul 8
3. Ehrmann S, Li J, Ibarra-Estrada M, et al: Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial. Lancet Respir Med 9(12):1387–1395, 2021. doi: 10.1016/S2213-2600(21)00356-8
Sedation and comfort
Richmond Agitation Sedation Scale, Riker Sedation-Agitation Scale
Neuromuscular blocking agents are not used routinely in patients undergoing mechanical ventilation because of the risk of prolonged neuromuscular weakness and the need for continuous heavy sedation; however, one study did show reduced mortality at 90 days in patients with early, severe ARDS who received 48 hours of neuromuscular blockade (1). Unfortunately, these findings were not replicated in a larger follow-up study of early neuromuscular blockade in ARDS, comparing it to lighter sedation without neuromuscular blockade (2). Therefore, routine paralysis for severe ARDS is not recommended. Exceptions who may benefit from neuromuscular blockade include patients who fail to tolerate some of the more sophisticated and complicated modes of mechanical ventilation and to prevent shivering when cooling is used after cardiac arrest.
Sedation and comfort references
1. Papazian L, Forel JM, Gacouin A, et al: Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med 363:1107–1116, 2010. doi: 10.1056/NEJMoa1005372
2. National Heart, Lung, and Blood Institute PETAL Clinical Trials Network, Moss M, Huang DT, Brower RG, et al: Early neuromuscular blockade in the acute respiratory distress syndrome. N Engl J Med 380(21):1997–2008, 2019. doi:10.1056/NEJMoa1901686
Complications of mechanical ventilation and safeguards
Complications of mechanical ventilation can be divided into those resulting from
Endotracheal intubation
Mechanical ventilation itself
Prolonged immobility and inability to eat normally
The presence of an endotracheal tube causes risk of sinusitis (which is rarely of clinical importance), ventilator-associated pneumonia, tracheal stenosis, vocal cord injury, and, very rarely, tracheal-esophageal or tracheal-vascular fistula. Purulent tracheal aspirate in a febrile patient who has an elevated white blood cell count > 48 hours after ventilation has begun suggests ventilator-associated pneumonia.
Complications of ongoing mechanical ventilation itself include pneumothorax and pneumatoceles, oxygen toxicity, hypotension, and ventilator-associated lung injury.
Oxygen toxicity refers to inflammatory changes, alveolar infiltration, and, eventually, pulmonary fibrosis that can develop following prolonged exposure to high FIO2 (eg, > 0.6). Toxicity is both concentration- and time-dependent. An FIO2 > 0.6 should be avoided unless necessary for survival. An FIO2 < 0.6 is well tolerated for long periods.
Ventilator-associated lung injury (VALI), sometimes termed ventilator-induced lung injury, is alveolar and/or small airway injury related to mechanical ventilation. Possible mechanisms include alveolar overdistention (ie, volutrauma) and the shear forces created by repetitive opening and collapse of alveoli (ie, atelectotrauma), leading to release of inflammatory mediators resulting in increased alveolar permeability, fluid accumulation, and loss of surfactant.
If acute hypotension develops in a mechanically ventilated patient, particularly when it is accompanied by tachycardia and/or a sudden increase in peak inspiratory pressure, tension pneumothorax must always be considered; patients with such findings should immediately have a chest examination and a chest x-ray (or immediate treatment if examination is confirmatory). More commonly, however, hypotension is a result of sympathetic lysis caused by sedatives or opioids used to facilitate intubation and ventilation. Hypotension can also be caused by decreased venous return due to high intrathoracic pressure in patients receiving high levels of PEEP or in those with high levels of intrinsic PEEP due to asthma or COPD. If there are no physical findings suggesting tension pneumothorax, and if ventilation-related causes of hypotension are a possible etiology, pending a portable chest x-ray, the patient may be disconnected from the ventilator and gently bagged manually at 2 to 3 breaths/minute with 100% oxygen while fluids are infused (eg, 500 to 1000 mL of 0.9% saline in adults, 20 mL/kg in children). An immediate improvement suggests a ventilation-related cause, and ventilator settings should be adjusted accordingly.
Relative immobility increases the risk of venous thromboembolic disease (eg, deep venous thrombosis, pulmonary embolism), skin breakdown, and atelectasis.
Most hospitals have standardized protocols to reduce complications. Elevating the head of the bed to > 30° decreases risk of ventilator-associated pneumonia, and routine turning of the patient every 2 hours decreases the risk of skin breakdown (see prevention of pressure ulcers
The most effective way to reduce complications of mechanical ventilation is to limit its duration. Daily “sedation vacations” and spontaneous breathing trials help determine the earliest point at which the patient may be liberated from mechanical support.






