


Periodontitis is a chronic inflammatory oral disease that progressively destroys the tooth-supporting apparatus. It usually manifests as a worsening of gingivitis and then, if untreated, with loosening and loss of teeth. Other symptoms are rare except in patients with HIV infection or in whom abscesses develop, in which case pain and swelling are common. Diagnosis is based on inspection, periodontal probing, and x-rays. Treatment involves dental cleaning that extends under the gingival (gum) tissues and a vigorous home hygiene program. Advanced cases may require antibiotics and surgery.
Pathophysiology of Periodontitis
Periodontitis usually develops when gingivitis, usually with abundant plaque and calculus (a concretion of bacteria, food residue, saliva, and mucus with calcium and phosphate salts) beneath the gingival margin, has not been adequately treated. In periodontitis, deep pockets form in the periodontal tissue and can harbor anaerobic organisms that do more damage than those usually present in simple gingivitis. Colonizing organisms include Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Eikenella corrodens, and many gram-negative bacilli.
The organisms trigger chronic release of inflammatory mediators, including cytokines, prostaglandins, and enzymes from neutrophils and monocytes. The resulting inflammation affects the periodontal ligament, gingiva, cementum, and alveolar bone. The gingiva progressively loses its attachment to the teeth, bone loss begins, and periodontal pockets deepen. With progressive bone loss, teeth may loosen, and gingiva recedes. Tooth migration is common in later stages, and tooth loss can occur.
Risk Factors for Periodontitis
Modifiable risk factors that contribute to periodontitis include
Plaque
Diabetes (especially type 1)
Emotional stress
Vitamin C deficiency (scurvy)
Addressing these conditions can improve the treatment outcomes of periodontitis.
Classification of Periodontitis
The American Academy of Periodontology's (AAP, 2017) classification of periodontal diseases and conditions distinguishes 3 forms of periodontitis:
Necrotizing periodontitis
Periodontitis as a direct manifestation of systemic disease
Periodontitis
Other periodontal conditions included in the AAP designations are periodontal abscesses, periodontitis associated with endodontic lesions, developmental or acquired deformities and conditions, and peri-implant diseases.
Periodontal abscesses are accumulations of pus that usually occur in pre-existing pockets, sometimes related to impacted foreign material. Tissue may be rapidly destroyed, risking tooth loss.
Periodontitis associated with endodontic lesions involves a communication between the pulp and periodontal tissues.
In developmental or acquired deformities and conditions, faulty occlusion, causing an excessive functional load on teeth, plus the requisite plaque and gingivitis may contribute to progression of a particular type of periodontitis characterized by angular bony defects.
Necrotizing periodontitis
Necrotizing periodontitis is a particularly virulent, rapidly progressing disease characterized by
Necrosis or ulceration of the interdental papillae
Bleeding gingiva
Pain
Necrotizing periodontitis typically occurs in patients with an impaired immune system and thus is often called HIV-associated periodontitis because HIV is a common cause. Clinically, it resembles acute necrotizing ulcerative gingivitis combined with generalized aggressive periodontitis. Patients may lose 9 to 12 mm of attachment in as little as 6 months.
In some patients, inflammation also involves the oral cavity, causing necrotizing stomatitis or a life-threatening variant, noma (cancrum oris).
Periodontitis as a direct manifestation of systemic disease
Periodontitis as a direct manifestation of systemic disease is considered in patients who have inflammation disproportionate to plaque or other local factors and who also have a systemic disease. However, distinguishing whether a disease is causing periodontitis or contributing to plaque-induced periodontitis is often difficult.
Systemic diseases associated with hematologic disease that can manifest as periodontitis include
Acquired neutropenia
Lazy leukocyte syndrome
Systemic diseases associated with genetic disorders that can manifest as periodontitis include
Familial and cyclic neutropenia
Leukocyte adhesion deficiency syndromes
Papillon-Lefèvre syndrome
Histiocytosis syndromes
Infantile genetic agranulocytosis
Ehlers-Danlos syndrome (types IV and VIII)
Cohen syndrome
Periodontitis
The previous (AAP, 1999) classification distinguished between chronic and aggressive periodontitis. However, although the age, rate of onset, and severity of periodontitis vary significantly, the underlying pathophysiology is now recognized to be similar and current evidence does not support such a distinction. Disease severity is now classified as stage I through IV, and rate of progression as grade A through C.
Periodontitis can begin anywhere between early childhood and older adulthood. About 85% of the population is affected to a mild degree, but the most advanced cases are seen in < 5% of the population.
Important severity factors include
Amount of loss of attachment (of soft tissue to teeth)
Depth of pockets
Amount of bone loss seen on x-ray
Symptoms and Signs of Periodontitis
Pain is usually absent unless an acute infection forms in one or more periodontal pockets or if HIV-associated periodontitis is present. Impaction of food in the pockets can cause pain at meals. Abundant plaque along with redness, swelling, and exudate are characteristic. Gums may be tender and bleed easily, and breath may be foul. As teeth loosen, particularly when only one third of the root is in the bone, chewing becomes painful.

Dr. W. GREEN/CNRI/SCIENCE PHOTO LIBRARY
CNRI/SCIENCE PHOTO LIBRARY

Image provided by Jonathan A. Ship, DMD.


Dr. W. GREEN/CNRI/SCIENCE PHOTO LIBRARY

CNRI/SCIENCE PHOTO LIBRARY

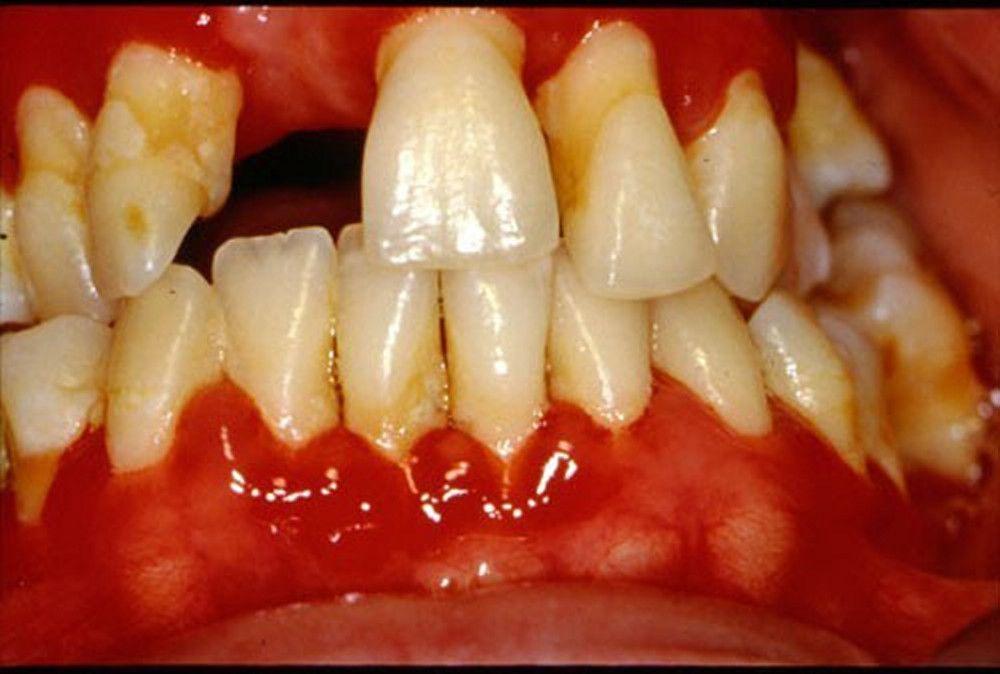
Image provided by Jonathan A. Ship, DMD.
Diagnosis of Periodontitis
Clinical evaluation
Sometimes dental x-rays
Inspection of the teeth and gingiva combined with probing of the pockets and measurement of their depth are usually sufficient for diagnosis. Pockets deeper than 4 mm indicate periodontitis.
Dental x-rays reveal alveolar bone loss adjacent to the periodontal pockets.
Treatment of Periodontitis
Treatment of risk factors
Scaling and root planing
Sometimes oral antibiotics, antibiotic packs, or both
Surgery or extraction
Treatment of modifiable risk factors such as poor oral hygiene, diabetes, and smoking improves outcomes.
Another approach is to surgically eliminate the pocket and recontour the bone (pocket reduction/elimination surgery) so that the patient can clean the depth of the normal crevice (sulcus) between the tooth and gingiva. In certain patients, regenerative surgery and bone grafting are done to encourage alveolar bone growth. Splinting of loose teeth and selective reshaping of tooth surfaces to eliminate traumatic occlusion may be necessary. Extractions are often necessary in advanced disease. Contributing systemic factors should be controlled before initiating periodontal therapy.
Key Points
Periodontitis is an inflammatory reaction triggered by bacteria in dental plaque.
There is loss of alveolar bone, formation of deep gum pockets, and eventually loosening of teeth.
Treatment involves scaling and root planing and sometimes antibiotics and/or surgery.






