


An extensive language has been developed to standardize the description of skin lesions, including
Lesion type (sometimes called primary morphology)
Lesion configuration (sometimes called secondary morphology)
Rash is a general term for a temporary skin eruption.
(See also Evaluation of the Dermatologic Patient and Diagnostic Tests for Skin Disorders.)
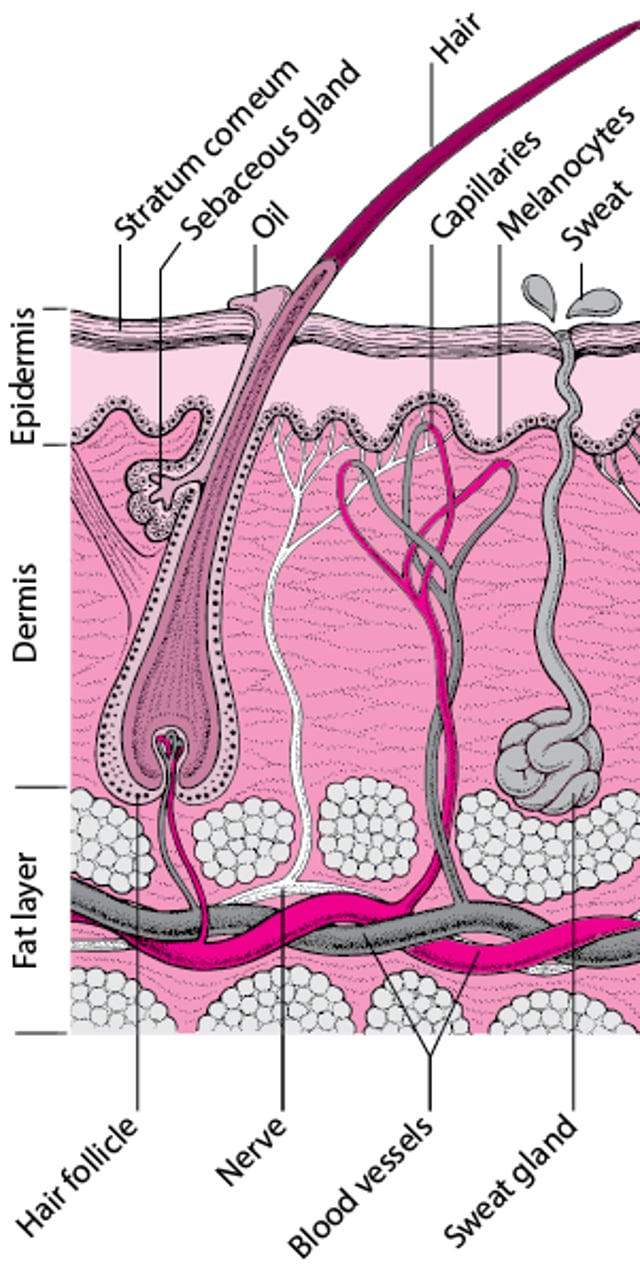
Cross-Section of the Skin and Skin Structures

Lesion Type (Primary Morphology)
Macules are flat, nonpalpable lesions usually < 10 mm in diameter. Macules represent a change in color and are not raised or depressed compared to the skin surface. A patch is a large macule. Examples include freckles, flat moles, tattoos, and port-wine stains, and the rashes of rickettsial infections, rubella, measles (can also have papules and plaques), and some allergic drug eruptions.


Papules are elevated lesions usually < 10 mm in diameter that can be felt or palpated. Examples include nevi, warts, lichen planus, insect bites, seborrheic keratoses, actinic keratoses, some lesions of acne, and skin cancers. The term maculopapular is often loosely and improperly used to describe many erythematous rashes; because this term is nonspecific and easily misused, it should be avoided.


Plaques are palpable lesions > 10 mm in diameter that are elevated or depressed compared to the skin surface. Plaques may be flat topped or rounded. Lesions of psoriasis and granuloma annulare commonly form plaques.


Nodules are firm papules or lesions that extend into the dermis or subcutaneous tissue. Examples include cysts, lipomas, and fibromas.
Vesicles are small, fluid-filled blisters < 10 mm in diameter. Vesicles are characteristic of herpes infections, acute allergic contact dermatitis, and some autoimmune blistering disorders (eg, dermatitis herpetiformis).


Bullae are fluid-filled blisters > 10 mm in diameter. These may be caused by burns, bites, irritant contact dermatitis or allergic contact dermatitis, and drug reactions. Classic autoimmune bullous diseases include pemphigus vulgaris and bullous pemphigoid. Bullae also may occur in inherited disorders of skin fragility.


Pustules are vesicles that contain pus. Pustules are common in bacterial infections and folliculitis and may arise in some inflammatory disorders including pustular psoriasis.


Urticaria (wheals or hives) is characterized by elevated lesions caused by localized edema. Wheals are pruritic and erythematous. Wheals are a common manifestation of hypersensitivity to medications, stings or bites, autoimmunity, and, less commonly, physical stimuli including temperature, pressure, and sunlight. The typical wheal lasts < 24 hours.


Scale is heaped-up accumulations of horny epithelium (stratum corneum) that occur in disorders such as psoriasis, seborrheic dermatitis, and fungal infections. Pityriasis rosea and chronic dermatitis of any type may be scaly.

Crusts (scabs) consist of dried serum, blood, or pus. Crusting can occur in inflammatory or infectious skin diseases (eg, impetigo).
Erosions are open areas of skin that result from loss of part or all of the epidermis. Erosions can be traumatic or can occur with various inflammatory or infectious skin diseases. An excoriation is a linear erosion caused by scratching, rubbing, or picking.
Ulcers result from loss of the epidermis and at least part of the dermis. Causes include venous stasis dermatitis, physical trauma with or without vascular compromise (eg, caused by decubitus ulcers or peripheral arterial disease), infections, and vasculitis.
Petechiae are nonblanchable punctate foci of hemorrhage. Causes include platelet abnormalities (eg, thrombocytopenia, platelet dysfunction), vasculitis, and infections (eg, meningococcemia, Rocky Mountain spotted fever, other rickettsioses).
Purpura is a larger area of hemorrhage that may be palpable. Purpura does not blanch. Palpable purpura is considered the hallmark of leukocytoclastic vasculitis. Purpura may indicate a coagulopathy. Large areas of purpura may be called ecchymoses or, colloquially, bruises.
Atrophy is thinning of the skin, which may appear dry and wrinkled, resembling cigarette paper. Atrophy may be caused by chronic sun exposure, aging, and some inflammatory and neoplastic skin diseases, including cutaneous T-cell lymphoma and lupus erythematosus. Atrophy also may result from long-term use of potent topical corticosteroids.
Scars are areas of fibrosis that replace normal skin after injury. Some scars become hypertrophic or thickened and raised. Keloids are hypertrophic scars that extend beyond the original wound margin.
Telangiectases are foci of small, permanently dilated blood vessels that may occur in areas of sun damage, rosacea, systemic diseases (especially systemic sclerosis), or inherited diseases (eg, ataxia-telangiectasia, hereditary hemorrhagic telangiectasia) or after long-term therapy with topical fluorinated corticosteroids.


Lesion Configuration (Secondary Morphology)
Configuration is the shape of single lesions and the arrangement of clusters of lesions.
Linear lesions take on the shape of a straight line and are suggestive of some forms of contact dermatitis, linear epidermal nevi, and lichen striatus. Excoriations resulting from scratching are typically linear.
Annular lesions are rings with central clearing. Examples include granuloma annulare, some drug eruptions, some dermatophyte infections (eg, tinea [ringworm]), and secondary syphilis.

Nummular lesions are circular or coin-shaped; an example is nummular dermatitis (nummular eczema).


MION/PHANIE/SCIENCE PHOTO LIBRARY
Target (bull’s-eye or iris) lesions appear as rings with central duskiness and are classic for erythema multiforme.


Serpiginous lesions have linear, branched, and curving elements. Examples include some fungal and parasitic infections (eg, cutaneous larva migrans).
Reticulated lesions have a lacy or networked pattern. Examples include cutis marmorata and livedo reticularis.


Herpetiform describes grouped papules or vesicles arranged like those of a herpes simplex infection.


Zosteriform describes lesions clustered in a dermatomal distribution similar to those of herpes zoster.
Texture of Skin Lesions
Some skin lesions have a visible or palpable texture that suggests a diagnosis.
Verrucous lesions have an irregular, pebbly, or rough surface. Examples include warts and seborrheic keratoses.
Lichenification is thickening of the skin with accentuation of normal skin markings; it results from repeated scratching or rubbing.

Induration, or deep thickening of the skin, can result from edema, inflammation, or infiltration, including by cancer. Indurated skin has a hard, resistant feeling. Induration is characteristic of panniculitis, some skin infections, and cutaneous metastatic cancers.
Umbilicated lesions have a central indentation and are usually viral. Examples include molluscum contagiosum and herpes simplex.
Xanthomas, which are yellowish, waxy lesions, may be idiopathic or may occur in patients who have lipid disorders.

Location and Distribution of Skin Lesions
It is important to note whether
Lesions are single or multiple.
Particular body parts are affected (eg, palms or soles, scalp, mucosal membranes).
Distribution is random or patterned, symmetric or asymmetric.
Lesions are on sun-exposed or protected skin.
Although few patterns are pathognomonic, some are consistent with certain diseases.
Psoriasis frequently affects the scalp, extensor surfaces of the elbows and knees, umbilicus, and the gluteal cleft.
Lichen planus frequently arises on the wrists, forearms, genitals, and lower legs.
Vitiligo may be patchy and isolated or may group around the distal extremities and face, particularly around the eyes and mouth.
Discoid lupus erythematosus has characteristic lesions on sun-exposed skin of the face, especially the forehead, nose, and the conchal bowl of the ear.
Hidradenitis suppurativa involves skin containing a high density of apocrine glands, including the axillae, groin, and under the breasts.
Color of Skin Lesions
When examining the color of skin, health care professionals should note that the natural color of a patient's skin can change the appearance of colors.
Red skin (erythema) can result from many different inflammatory or infectious diseases. Cutaneous tumors are often pink or red. Superficial vascular lesions such as port-wine stains may appear red.
Orange skin is most often seen in hypercarotenemia, a usually benign condition of carotene deposition after excess dietary ingestion of beta-carotene.
Yellow skin is typical of jaundice, xanthelasmas and xanthomas, and pseudoxanthoma elasticum.
Green fingernails suggest Pseudomonas aeruginosa infection.
Violet skin may result from cutaneous hemorrhage or vasculitis. Vascular lesions or tumors, such as Kaposi sarcoma and hemangiomas, can appear purple. A lilac color of the eyelids or heliotrope eruption is characteristic of dermatomyositis.
Shades of blue, silver, and gray
Black skin lesions may be melanocytic, including nevi and melanoma. Black eschars are collections of dead skin that can arise from infarction, which may be caused by infection (eg, anthrax, angioinvasive fungi including Rhizopus, meningococcemia), calciphylaxis, arterial insufficiency, or vasculitis.
Other Clinical Signs of Skin Lesions
Dermatographism (dermographism) is the appearance of an urticarial wheal after focal pressure (eg, stroking or scratching the skin) in the distribution of the pressure. Up to 5% of patients may exhibit this sign, which is a form of physical urticaria.


Darier sign refers to rapid swelling of a lesion when stroked. It occurs in patients with urticaria pigmentosa or mastocytosis.


© Springer Science+Business Media
Nikolsky sign is epidermal shearing that occurs with gentle lateral pressure on seemingly uninvolved skin in patients with toxic epidermal necrolysis and some autoimmune bullous diseases.
Auspitz sign is the appearance of pinpoint bleeding after scale is removed from plaques in psoriasis.
Koebner phenomenon describes the development of lesions within areas of trauma (eg, caused by scratching, rubbing, or injury). Psoriasis frequently exhibits this phenomenon, as may lichen planus, often resulting in linear lesions.






