


Alopecia is defined as loss of hair from the body. Hair loss is often a cause of great concern to the patient for cosmetic and psychologic reasons, but it can also be an important sign of systemic disease.
(See also Alopecia Areata.)
Pathophysiology of Alopecia
Growth cycle
Hair grows in cycles. Each cycle consists of phases:
Anagen: A long (2- to 6-year) growing phase
Catagen: A brief (3-week) transitional apoptotic phase
Telogen: A short (2- to 3-month) resting phase
At the end of the resting phase, the hair falls out (exogen). Normally, about 50 to 100 scalp hairs reach the end of resting phase each day and fall out. When a new hair starts growing in the follicle, the cycle begins again.
Disorders of the growth cycle include
Anagen effluvium—a disruption of the growing phase causing abnormal loss of anagen hairs
Telogen effluvium—significantly more than 100 hairs/day going into resting phase
Classification
Alopecia can be classified as focal or diffuse and by the presence or absence of scarring.
Scarring alopecia is the result of active destruction of the hair follicle. The follicle is irreparably damaged and replaced by fibrotic tissue. Several hair disorders show a biphasic pattern in which nonscarring alopecia occurs early in the course of the disease, and then scarring alopecia and permanent hair loss occurs as the disease progresses. Scarring alopecias can be subdivided further into primary forms, where the target of inflammation is the follicle itself, and secondary forms, where the follicle is destroyed as a result of nonspecific inflammation (see table Some Causes of Alopecia).
Nonscarring alopecia results from processes that reduce or slow hair growth without irreparably damaging the hair follicle. Disorders that primarily affect the hair shaft (trichodystrophies) also are considered nonscarring alopecia.
Etiology of Alopecia
The alopecias comprise a large group of disorders with multiple and varying etiologies (see table Some Causes of Alopecia).


The most common cause of alopecia is
Androgenetic alopecia (male-pattern or female-pattern hair loss)
Androgenetic alopecia is an androgen-dependent hereditary disorder in which dihydrotestosterone plays a major role. The prevalence of this form of alopecia increases with age, and it affects over 70% of men (male-pattern hair loss) and 57% of all women (female-pattern hair loss) over the age of 80 (1). The prevalence is lower in Asian and Black people than in White people.

Other common causes of hair loss are
Drugs (including chemotherapeutic agents)
Infection (eg, tinea capitis, kerion)
Systemic disorders (disorders that cause high fever, endocrine disorders)
Trauma
Traumatic causes include trichotillomania, traction alopecia, burns, radiation, and pressure-induced (eg, postoperative) hair loss.
Less common causes are
Primary hair shaft abnormalities
Autoimmune diseases
Lichen planopilaris/frontal fibrosing alopecia
Rare dermatologic conditions (eg, dissecting cellulitis of the scalp)
Etiology reference
1. Adil A, Godwin M: The effectiveness of treatments for androgenetic alopecia: A systematic review and meta-analysis. J Am Acad Dermatol 77(1):136–141.e5, 2017. doi: 10.1016/j.jaad.2017.02.054
Evaluation of Alopecia
History
History of present illness should cover the onset and duration of hair loss, whether hair shedding is increased, and whether hair loss is generalized or localized. Associated symptoms such as pruritus and scaling should be noted. Patients should be asked about typical hair care practices, including use of braids, rollers, and hair dryers, and whether they routinely pull or twist their hair.
Review of systems should include recent exposures to noxious stimuli (eg, drugs, toxins, radiation) and stressors (eg, surgery, chronic illness, fever, psychologic stressors). Symptoms of possible causes (eg, fatigue and cold intolerance [hypothyroidism] and, in women, hirsutism, deepening of the voice, and increased libido [virilization]) should be sought. Other features, including dramatic weight loss, dietary practices (including various restrictive diets), and obsessive-compulsive behavior, should be noted. In women, a hormonal/gynecologic/obstetric history should be obtained.
Past medical history should note known possible causes of hair loss, including endocrine and skin disorders. Current and recent drug use should be reviewed for offending agents (see table Some Causes of Alopecia). A family history of hair loss should be recorded.
Physical examination
Examination of the scalp should note the distribution of hair loss, the presence and characteristics of any skin lesions, and whether there is scarring. Part widths should be measured. Abnormalities of the hair shafts should be noted.
A full skin examination should be done to evaluate hair loss elsewhere on the body (eg, eyebrows, eyelashes, arms, legs), rashes that may be associated with certain types of alopecia (eg, discoid lupus lesions, signs of secondary syphilis or of other bacterial or fungal infections), and signs of virilization in women (eg, hirsutism, acne, deepening voice, clitoromegaly). Signs of potential underlying systemic disorders should be sought, and a thyroid examination should be done.
Red flags
The following findings are of particular concern:
Virilization in women
Signs of systemic illness or constellations of nonspecific findings possibly indicating poisoning
Interpretation of findings
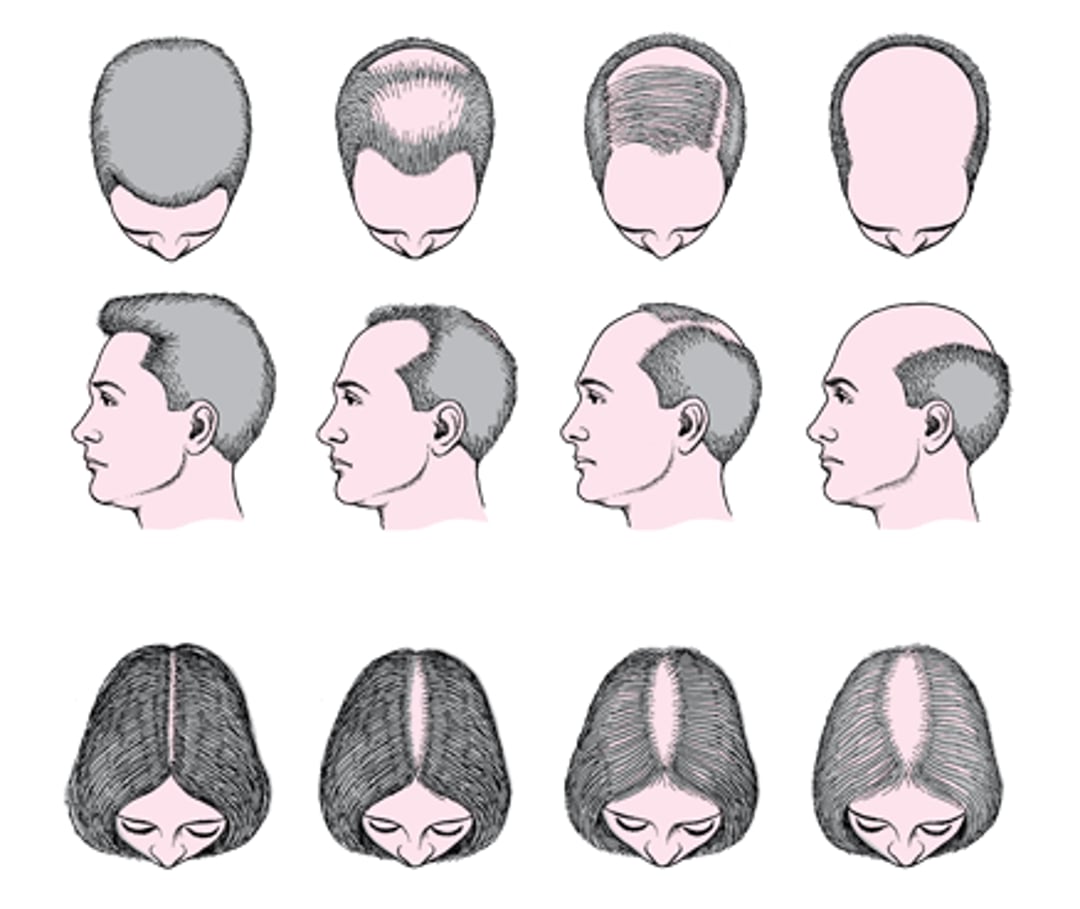
Hair loss that begins at the temples and/or crown (vertex) and spreads to diffuse thinning or nearly complete hair loss is typical of male-pattern hair loss. Hair thinning in the frontal, parietal, and crown regions is typical of female-pattern hair loss (see figure Male- and female-pattern hair loss (androgenetic alopecia)). In androgenetic alopecia, the central part width is wider on the crown of the scalp than it is on the occipital scalp.
Male- and female-pattern hair loss (androgenetic alopecia)

Hair loss that occurs 2 to 4 weeks after chemotherapy or radiation therapy (anagen effluvium) can typically be ascribed to those causes. Hair loss that occurs 3 to 4 months after a major stressor (pregnancy, major febrile illness, surgery, medication change, or severe psychologic stressor) suggests a diagnosis of telogen effluvium.
Other findings help suggest alternative diagnoses (see table Interpreting Physical Findings in Alopecia).

© Springer Science+Business Media

© Springer Science+Business Media

© Springer Science+Business Media


© Springer Science+Business Media


© Springer Science+Business Media


© Springer Science+Business Media
Other than hair loss, scalp symptoms (eg, itching, burning, tingling) are often absent and, when present, are not specific to any cause.
Signs of hair loss in patterns other than those described above are nondiagnostic and may require microscopic hair examination or scalp biopsy for definitive diagnosis.
Testing
Evaluation for causative disorders (eg, endocrinologic, autoimmune, toxic) should be done based on clinical suspicion.
Male-pattern hair loss usually requires no testing. Female-pattern hair loss is usually evaluated with thyroid function testing. When it occurs in young men with no family history, the physician should question the patient about use of anabolic steroids and other drugs. In addition to questions regarding prescription drug and illicit drug use, women with significant hair loss and evidence of virilization should have levels of appropriate hormones (eg, testosterone and dehydroepiandrosterone sulfate [DHEAS]) measured (see Hirsutism).
The pull test helps evaluate diffuse scalp hair loss. Gentle traction is exerted on a bunch of hairs (about 40) on at least 3 different areas of the scalp, and the number of extracted hairs is then counted and examined microscopically. Normally, < 3 telogen-phase hairs should come out with each pull. If > 4 to 6 hairs come out with each pull, the pull test is positive and is suggestive of telogen effluvium.
The pluck test involves sequentially pulling out about 50 individual hairs abruptly (“by the roots”). The roots of the plucked hairs are examined microscopically to determine the phase of growth and thus help diagnose a defect of telogen or anagen or an occult systemic disease. Anagen hairs have sheaths attached to their roots; telogen hairs have tiny bulbs without sheaths at their roots. Normally, 85 to 90% of hairs are in the anagen phase, about 10 to 15% are in telogen phase, and < 1% are in catagen phase. Telogen effluvium shows an increased percentage of telogen-phase hairs on microscopic examination (typically > 20%), whereas anagen effluvium shows a decrease in telogen-phase hairs and an increased number of broken hairs. Primary hair shaft abnormalities are usually obvious on microscopic examination of the hair shaft.
Scalp biopsy is indicated when alopecia persists and diagnosis is in doubt. Biopsy may differentiate scarring from nonscarring forms. Specimens should be taken from areas of active inflammation, ideally at the border of a bald patch. Fungal and bacterial cultures may be useful.
Daily hair counts can be done by the patient to quantify hair loss when the pull test is negative. Hairs lost during the first morning combing or during washing are collected in clear plastic bags daily for 14 days. The number of hairs in each bag is then recorded. Scalp hair counts of > 100/day are abnormal except after shampooing, when hair counts of up to 250 may be normal. Hairs may be brought in by the patient for microscopic examination.
Treatment of Alopecia
Drugs (including hormonal modulators)
Laser light therapy
Surgery
Androgenetic alopecia
alopecia areata. Hair regrowth can take 8 to 12 months. Treatment is continued indefinitely because, once treatment is stopped, hair loss resumes. The most frequent adverse effects are mild scalp irritation, allergic contact dermatitis1, 2).
inhibits the 5-alpha-reductase enzyme, blocking conversion of testosteroneMale Sexual Dysfunction); hypersensitivity reactions; gynecomastia; myopathy; and rarely symptoms of depression. There may be a decrease in prostate-specific antigen (PSA)
Hormonal modulators
Low-level laser light therapy is an alternate or additional treatment for androgenetic alopecia that has been shown to promote hair growth. Physician-dispensed and over-the-counter devices are available.
Autologous platelet-rich plasma injected into the scalp is thought to contain growth factors that promote hair follicle growth and maintenance (3).
Surgical options include follicle transplant, scalp flaps, and alopecia reduction. Few procedures have been subjected to scientific scrutiny, but patients who are self-conscious about their hair loss may consider them (4).
Hair loss due to other causes
Underlying disorders are treated.
Treatment for traction alopecia is elimination of physical traction or stress to the scalp.
Treatment for tinea capitis is oral antifungals.
Trichotillomaniaselective serotonin reuptake inhibitor
Hair loss due to chemotherapy (anagen effluvium) is temporary and is best treated with a wig; when hair regrows, it may be different in color and texture from the original hair. Hair loss due to telogen effluvium is usually temporary as well and abates after the precipitating agent is eliminated.
Treatment references
1. Randolph M, Tosti AJ Am Acad Dermatol 84(3):737–746, 2021. doi: 10.1016/j.jaad.2020.06.1009
2. Gupta AK, Venkataraman M, Talukder M, Bamimore MAJAMA Dermatol 158(3):266–274, 2022. doi: 10.1001/jamadermatol.2021.5743
3. Hesseler MJ, Shyam N: Platelet-rich plasma and its utilities in alopecia: A systematic review. Dermatol Surg 46(1):93–102, 2020. doi: 10.1097/DSS.0000000000001965
4. Adil A, Godwin M: The effectiveness of treatments for androgenetic alopecia: A systematic review and meta-analysis. J Am Acad Dermatol 77(1):136–141.e5, 2017. doi: 10.1016/j.jaad.2017.02.054
Key Points
Androgenetic alopecia (male-pattern and female-pattern hair loss) is the most common type of hair loss.
Concomitant virilization in women or scarring hair loss should prompt a thorough evaluation for an underlying disorder.
Microscopic hair examination or scalp biopsy may be required for definitive diagnosis.






