


Erythropoietic protoporphyria (EPP) is due to an inherited deficiency in the activity of the enzyme ferrochelatase. X-linked protoporphyria (XLPP) is due to an inherited increase in the activity of delta-aminolevulinic acid synthase-2. Enzymes that cause both EPP and XLPP are in the heme biosynthetic pathway (see table
(See also Overview of Porphyrias and Overview of Cutaneous Porphyrias.)
Because XLPP is so similar to EPP, it is sometimes regarded as a variant of EPP.
Etiology
Erythropoietic protoporphyria, which comprises about 90% of EPP phenotypic presentations results from inherited deficiency of the enzyme ferrochelatase. The inheritance pattern is autosomal recessive; thus, clinical manifestations occur only in people with 2 defective FECH alleles, or more commonly, one defective and one low-expressing wild-type allele (1).
X-linked protoporphyria, which comprises the remaining 10% of cases, results from gain-of-function mutations that increase the activity of erythroid-specific delta-aminolevulinate synthase (ALAS 2) in the bone marrow; inheritance is X-linked. The phenotype of heterozygous females can vary from asymptomatic to that of affected males (1).
Prevalence of EPP phenotype is about 1/75,000. However, a study from the UK Biobank found that the prevalence of EPP was about 1/17,000 (2). The authors attributed this higher prevalence to under diagnosis. Protoporphyrin accumulates in bone marrow and red blood cells, enters the plasma, and is deposited in the skin or excreted by the liver into bile. About 10% of patients develop chronic liver disease; a few of these patients develop cirrhosis, which may progress to liver failure. A more common complication is pigment gallstones due to heavy protoporphyrin excretion.
Etiology references
1. Balwani M, Doheny D, Bishop DF, et al: Loss-of-function ferrochelatase and gain-of-function erythroid-specific 5-aminolevulinate synthase mutations causing erythropoietic protoporphyria and x-linked protoporphyria in North American patients reveal novel mutations and a high prevalence of X-linked protoporphyria. Mol Med 19(1):26–35, 2013. doi:10.2119/molmed.2012.00340
2. Dickey AK, Quick C, Ducamp S, et al: Evidence in the UK Biobank for the underdiagnosis of erythropoietic protoporphyria. Genet Med 23(1):140–148, 2021. doi:10.1038/s41436-020-00951-8
Symptoms and Signs
Symptom severity in erythropoietic protoporphyria and X-linked protoporphyria varies greatly, even among patients within a single family. One study suggests that higher levels of erythrocyte protoporphyrin are a major determinant of disease severity and risk of liver dysfunction in patients with EPP or XLPP (1).
Most patients develop symptoms in early childhood. Brief exposure to sunlight can cause severe pain, burning, erythema, and edema of the exposed skin. Usually, an infant or young child cries for hours after even short exposure to sun. Patients are often erroneously said to suffer from "sun allergy." Sometimes skin swelling and erythema may be subtle or absent, and EPP and XLPP may go undiagnosed longer than any other of the porphyrias.

© Springer Science+Business Media

By permission of the publisher. From Bloomer J, Risheg H. In Gastroenterology and Hepatology: Liver. Edited by M Feldman (series editor) and WC Maddrey. Philadelphia, Current Medicine, 2004.

Image courtesy of Karen McKoy, MD.
© Springer Science+Business Media


© Springer Science+Business Media


By permission of the publisher. From Bloomer J, Risheg H. In Gastroenterology and Hepatology: Liver. Edited by M Feldman (series editor) and WC Maddrey. Philadelphia, Current Medicine, 2004.

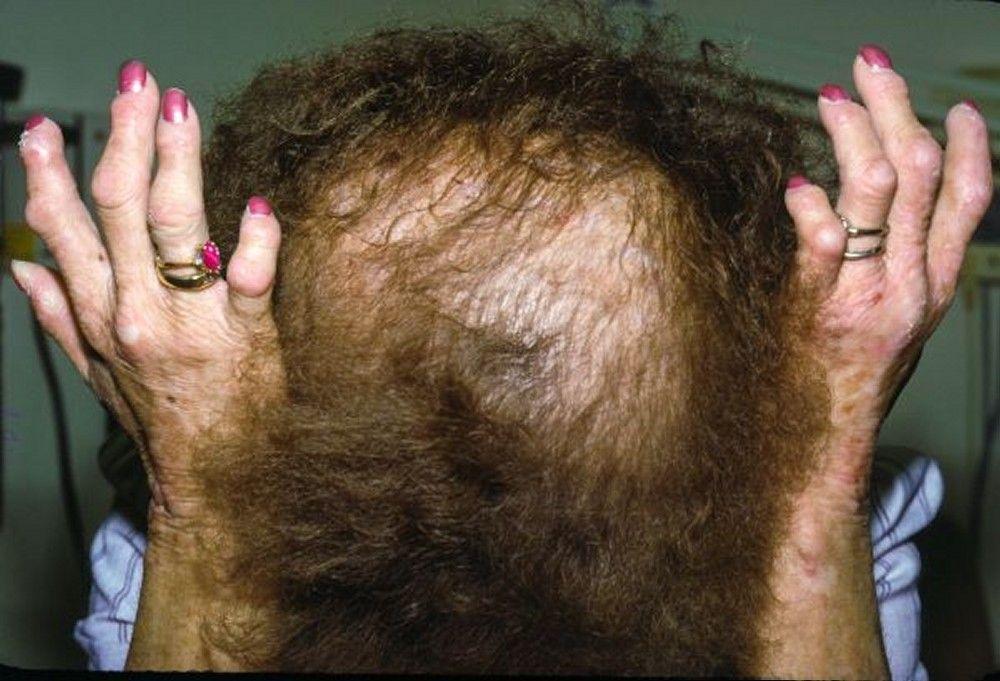
Image courtesy of Karen McKoy, MD.

© Springer Science+Business Media
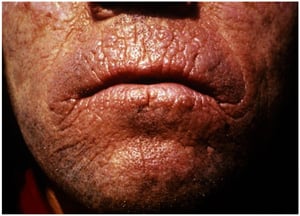
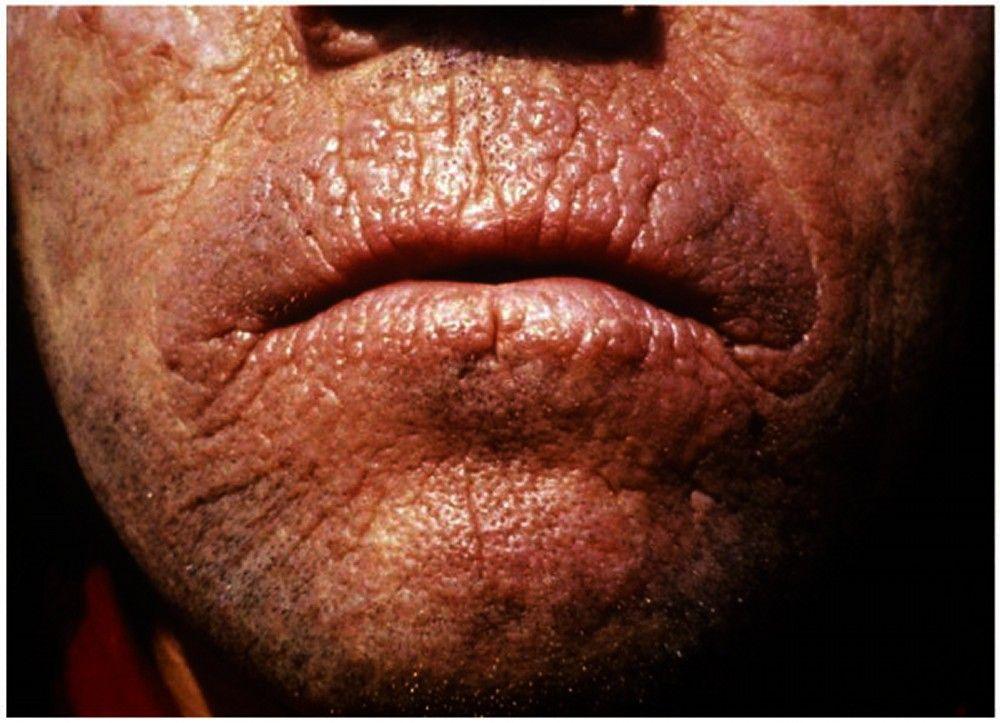
Crusting may develop around the lips and on the back of the hands after prolonged sun exposure. However, blistering and scarring, as are typical in porphyria cutanea tarda, variegate porphyria, and congenital erythropoietic porphyria (see table Some Less Common Porphyrias), do not occur.
If skin protection is chronically neglected, rough, thickened, and leathery skin (lichenification) may develop, especially over the knuckles. Linear perioral furrows (carp mouth) may develop. Patients with XLPP tend to have more severe photosensitivity and liver disease than those with EPP.
If unrecognized, erythropoietic protoporphyria and X-linked protoporphyria may cause psychosocial problems because children inexplicably refuse to go outdoors. The fear or anticipation of pain may be so distressing that children become nervous, tense, aggressive, or even develop feelings of detachment from the surroundings or suicidal thoughts.
Symptoms and signs reference
1. Balwani M, Naik H, Anderson KE, et al: Clinical, biochemical, and genetic characterization of North American patients with erythropoietic protoporphyria and X-linked protoporphyria. JAMA Dermatol 153(8):789–796, 2017. doi:10.1001/jamadermatol.2017.1557
Diagnosis
Red blood cell and plasma protoporphyrin measurement
Genetic testing for FECH or ALAS 2 gene mutations
Erythropoietic protoporphyria or X-linked protoporphyria should be suspected in children and adults with painful cutaneous photosensitivity who experience no blisters or scarring. Gallstones in children should prompt testing for EPP and XLPP. Family history is usually negative.
The diagnosis is confirmed by finding increased red blood cell and plasma protoporphyrin levels. The peak plasma fluorescence occurs at 634 nm, following excitation at 410 nm.
Red blood cell protoporphyrin should also be fractionated to determine the proportions of metal-free and zinc protoporphyrin. In EPP, the proportion of red blood cell protoporphyrin that is metal-free is almost always > 85%. The presence of > 15% zinc protoporphyrin suggests XLPP.
If measured, plasma coproporphyrin and urinary porphyrin levels are normal. Stool protoporphyrin may be elevated, but coproporphyrin level is normal.
Potential carriers among relatives can be identified by finding increased red blood cell protoporphyrin levels and by genetic testing if a mutation has been identified in the index case.
Treatment
Avoidance of sun exposure through use of protective clothing and opaque sunscreens
Symptomatic treatment for skin burning with cold compresses, nonsteroidal anti-inflammatory drugs (NSAIDs), and topical and/or oral corticosteroids
Management of hepatobiliary complications
1).
Oral beta-carotene, an antioxidant, reduces photosensitivity. However, patient adherence with beta-carotene is often poor because it is not very effective in controlling symptoms and also causes orange skin pigmentation; thus it is often tried but usually not continued. Beta-carotene dose depends on patient’s age (see table Doses of Beta-Carotene in Erythropoietic Protoporphyria).
Medications that trigger acute porphyrias need not be avoided (see the Drug Database for Acute Porphyria or the American Porphyria Foundation drug database).
In some patients, acute skin symptoms can be alleviated by cold baths or wet towels, analgesics, and topical and/or oral corticosteroids. However, many patients do not find such measures very effective. Symptoms can take up to a week to resolve.
If these measures are ineffective (eg, patients have increasing photosensitivity, rising porphyrin levels, progressive jaundice), giving hematin and/or red blood cell hypertransfusion (ie, to above-normal hemoglobin levels) may reduce protoporphyrin overproduction. Administration of bile acids may facilitate biliary excretion of protoporphyrin.
Patients who develop decompensated end-stage liver disease require liver transplantation. As with acute intermittent porphyria, patients with EPP are not eligible for standardized Model for End-Stage Liver Disease (MELD)-exception points. However, liver transplantation does not correct the underlying metabolic defect and EPP hepatopathy often develops in the transplanted liver.
Hematopoietic stem cell transplantation is curative for EPP but is not routinely done because the risk typically outweighs the benefits. The strategy of hematopoietic stem cell transplantation after liver transplantation cures EPP and prevents recurrent EPP from damaging the allograft, but the optimal timing of this strategy has not been established. Patients should be protected from operating room lights during liver transplantation or other prolonged surgery to avoid serious phototoxic injury to internal organs. Light sources should be covered with commercially available filters that block wavelengths ~380 to 420 nm. Endoscopy, laparoscopy, and brief (< 1.5 hour) abdominal surgery do not usually cause phototoxic damage.
Pearls & Pitfalls
|
Regular physician-patient consultations that provide information, discussion, and opportunities for genetic counseling together with physical checkups are important. Liver function and red blood cell and plasma protoporphyrin levels should be checked annually.
Patients with abnormal liver function test results should be evaluated by a hepatologist; a liver biopsy may be needed to stage the degree of fibrosis. Patients with known chronic liver disease should undergo screening liver ultrasonography, CT, or MRI every 6 months to check for hepatocellular carcinoma.
Vitamin D levels should be checked because deficiency is common (patients tend to avoid sun exposure); supplements are given if levels are low.
All patients with EPP and XLPP should receive and and be advised to avoid alcohol.
Treatment reference
1. Langendonk JG, Balwani M, Anderson KE, et al: Afamelanotide for erythropoietic protoporphyria. N Engl J Med 373:48–59, 2015. doi: 10.1056/NEJMoa1411481.
Key Points
Erythropoietic protoporphyria (EPP) causes severe pain, burning, erythema, and edema of exposed skin even after only brief exposure to sunlight; symptoms are not brought on by medications that trigger other porphyrias.
Cirrhosis develops in about 10% of patients, sometimes progressing to liver failure.
Measure red blood cell and plasma protoporphyrin levels.
Hematin and/or red blood cell hypertransfusion may reduce protoporphyrin overproduction.
X-linked protoporphyria (XLPP) is clinically similar to EPP, but photosensitivity and liver disease are more severe than in EPP.
A useful clue for XLPP is a high proportion of red blood cell protoporphyrin that is zinc protoporphyrin.
Management of XLPP is similar to that of EPP.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
American Porphyria Foundation: Aims to educate and support patients and families affected by porphyrias and to support research into treatment and prevention of porphyrias
American Porphyria Foundation: Safe/Unsafe Drug Database: Provides a list of medications available in the United States to assist physicians in prescribing for patients with porphyrias
European Porphyria Network: Promotes clinical research about porphyrias
The Drug Database for Acute Porphyrias: Provides an up-to-date list of medications available in Europe to assist physicians in prescribing for patients with porphyrias
United Porphyrias Association: Provides education and support to patients and their families; provides reliable information to health-care providers; fosters and supports clinical research to improve diagnosis and management of the porphyrias






