


Hyperthyroidism is characterized by hypermetabolism and elevated serum levels of free thyroid hormones. Symptoms include palpitations, fatigue, weight loss, heat intolerance, anxiety, and tremor. Diagnosis is clinical and with thyroid function tests. Treatment depends on cause.
(See also Overview of Thyroid Function.)
Hyperthyroidism affects about 1% of people in the United States. It can occur at any age but is more common in females between the ages of 20 and 50 years (1).
Hyperthyroidism can be classified on the basis of thyroid radioactive iodine uptake and the level of circulating thyroid hormones (see table Results of Thyroid Function Tests in Various Clinical Situations).
General reference
1. Lee SY, Pearce EN. Hyperthyroidism: A Review. JAMA 2023;330(15):1472-1483. doi:10.1001/jama.2023.19052
Etiology of Hyperthyroidism
Hyperthyroidism may result from increased synthesis and secretion of thyroid hormones (thyroxine [T4] and triiodothyronine [T3]) from the thyroid, caused by thyroid-stimulating immunoglobulin (TSI) or by autonomous thyroid hyperfunction. It can also result from excessive release of thyroid hormone from the thyroid without increased synthesis. Such release is commonly caused by the destructive changes of various types of thyroiditis.
The most common causes of hyperthyroidism include
Graves disease
Multinodular goiter
Single, autonomous, hyperfunctioning "hot" nodule
Thyroiditis
Graves disease (toxic diffuse goiter), the most common cause of hyperthyroidism, is characterized by hyperthyroidism and one or more of the following:
Goiter
Infiltrative dermopathy
Graves disease is caused by an autoantibody (TSI) against the thyroid receptor for thyroid-stimulating hormone (TSH); unlike most autoantibodies, which are inhibitory, this autoantibody is stimulatory, thus causing continuous synthesis and secretion of excess T4 and T3. Graves disease (like Hashimoto thyroiditis) sometimes occurs with other autoimmune disorders, including type 1 diabetes mellitus, vitiligo, premature graying of hair, pernicious anemia, connective tissue disorders, and polyglandular deficiency syndrome. Heredity increases the risk of Graves disease, although the genes involved are unknown.
The pathogenesis of infiltrative ophthalmopathy (responsible for the exophthalmos in Graves disease) is poorly understood but may result from immunoglobulins directed to the TSH receptors in the orbital fibroblasts and fat that result in release of proinflammatory cytokines, inflammation, and accumulation of glycosaminoglycans. Ophthalmopathy may also occur before the onset of hyperthyroidism or as late as 20 years afterward and frequently worsens or abates independently of the clinical course of hyperthyroidism. Typical ophthalmopathy in the presence of normal thyroid function is called euthyroid Graves disease (see photo Eye Manifestations of Graves Disease—Exophthalmos).
Toxic solitary or multinodular goiter (Plummer disease) sometimes results from TSH receptor gene mutations causing continuous thyroid activation. Patients with toxic nodular goiter have none of the autoimmune manifestations or circulating antibodies observed in patients with Graves disease. Also, in contrast to Graves disease, toxic solitary and multinodular goiters usually do not remit.
Inflammatory thyroid disease (thyroiditis) includes subacute granulomatous thyroiditis, Hashimoto thyroiditis, and silent lymphocytic thyroiditis, a variant of Hashimoto thyroiditis. Hyperthyroidism is more common in subacute granulomatous thyroiditis and results from destructive changes in the gland and release of stored hormone, not from increased synthesis. Hypothyroidism may follow.
Inappropriate TSH secretion is a rare cause. Patients with primary hyperthyroidism have undetectable TSH levels. However, TSH levels are detectable in patients with a TSH-secreting anterior pituitary adenoma or with pituitary resistance to thyroid hormone, in whom TSH levels are high. The TSH produced in both of these pituitary disorders is biologically more active than normal TSH. An increase in the alpha-subunit of TSH in the blood (helpful in differential diagnosis) occurs in patients with a TSH-secreting pituitary adenoma.
Medication-induced hyperthyroidism
Thyrotoxicosis factitia is hyperthyroidism resulting from intentional or accidental overingestion of thyroid hormone.
Excess iodine ingestion
Hydatidiform mole (molar pregnancy) and choriocarcinoma produce high levels of serum human chorionic gonadotropin (hCG), a weak thyroid stimulator. Levels of hCG are highest during the first trimester of pregnancy and result in the decrease in serum TSH and mild increase in serum free T4 sometimes observed at that time. The increased thyroid stimulation may be caused by increased levels of partially desialated hCG, an hCG variant that appears to be a more potent thyroid stimulator than more sialated hCG. Hyperthyroidism in molar pregnancy, choriocarcinoma, and hyperemesis gravidarum is transient; normal thyroid function resumes when the molar pregnancy is evacuated, the choriocarcinoma is appropriately treated, or the hyperemesis gravidarum abates.
Nonautoimmune autosomal dominant hyperthyroidism manifests during infancy. It results from mutations in the TSH receptor gene that produce continuous thyroid stimulation.
Metastatic thyroid cancer is a possible cause. Overproduction of thyroid hormone occurs rarely from functioning metastatic follicular carcinoma, especially in pulmonary metastases.
Struma ovarii develops when ovarian teratomas contain enough thyroid tissue to cause true hyperthyroidism. Radioactive iodine uptake occurs in the pelvis, and uptake by the thyroid is usually suppressed.
Pathophysiology of Hyperthyroidism
In hyperthyroidism, serum T3 usually increases more than does T4, probably because of increased secretion of T3 as well as conversion of T4 to T3 in peripheral tissues. In some patients, only T3 is elevated (T3 toxicosis).
T3 toxicosis may occur in any of the common disorders that cause hyperthyroidism, including Graves disease, multinodular goiter, and the autonomously functioning solitary thyroid nodule. If T3 toxicosis is untreated, the patient usually also develops laboratory abnormalities typical of hyperthyroidism (ie, elevated T4 and increased iodine-123 uptake). The various forms of thyroiditis commonly have a hyperthyroid phase followed by a hypothyroid phase.
Symptoms and Signs of Hyperthyroidism
Most symptoms and signs are the same regardless of the cause. Exceptions include infiltrative ophthalmopathy and infiltrative dermopathy, which occur only in Graves disease.
Pearls & Pitfalls
|
The clinical presentation may be dramatic or subtle. A goiter or nodule may be present.
Many common symptoms of hyperthyroidism are due to enhanced sensitivity to adrenergic hormones, such as nervousness, palpitations, hyperactivity, increased sweating, heat hypersensitivity, fatigue, increased appetite, weight loss, insomnia, weakness, and frequent bowel movements (occasionally diarrhea). Hypomenorrhea may be present.
Signs may include warm, moist skin, tremor, tachycardia, widened pulse pressure, and atrial fibrillation.


© Springer Science+Business Media
Older patients, particularly those with toxic nodular goiter, may present atypically (apathetic or masked hyperthyroidism) with symptoms more akin to depression or dementia. Most do not have exophthalmos or tremor. Atrial fibrillation, syncope, altered sensorium, heart failure, and weakness are more likely. Symptoms and signs may involve only a single organ system.
Eye signs
Eye signs of hyperthyroidism include stare, eyelid lag, eyelid retraction, and mild conjunctival injection and are largely due to excessive adrenergic stimulation. They usually remit with successful treatment to normalize thyroid hormone levels.
Infiltrative ophthalmopathy, also called thyroid eye disease, is a more serious development and is specific to Graves disease. It can occur years before or after hyperthyroidism. It is characterized by orbital pain, lacrimation, irritation, photophobia, increased retro-orbital tissue, exophthalmos, and lymphocytic infiltration of the extraocular muscles, causing ocular muscle weakness that frequently leads to double vision.

By permission of the publisher. From Mulligan M, Cousins M. In Atlas of Anesthesia: Preoperative Preparation and Intraoperative Monitoring. Edited by R Miller (series editor) and JL Lichtor. Philadelphia, Current Medicine, 1998.

© Springer Science+Business Media

© Springer Science+Business Media

© Springer Science+Business Media

© Springer Science+Business Media


By permission of the publisher. From Mulligan M, Cousins M. In Atlas of Anesthesia: Preoperative Preparation and Intraoperative Monitoring. Edited by R Miller (series editor) and JL Lichtor. Philadelphia, Current Medicine, 1998.


© Springer Science+Business Media


© Springer Science+Business Media


© Springer Science+Business Media


© Springer Science+Business Media
Infiltrative dermopathy
Infiltrative dermopathy, also called pretibial myxedema (a confusing term, because myxedema suggests hypothyroidism), is characterized by nonpitting infiltration by proteinaceous ground substance, usually in the pretibial area. It rarely occurs in the absence of Graves ophthalmopathy. The lesion is often pruritic and erythematous in its early stages and subsequently becomes brawny. Infiltrative dermopathy may appear years before or after hyperthyroidism.

Photo courtesy of Karen McKoy, MD.

© Springer Science+Business Media

By permission of the publisher. From Burman K, Becker K, Cytryn A, et al. In Atlas of Clinical Endocrinology: Thyroid Diseases . Edited by SG Korenman (series editor) and MI Surks. Philadelphia, Current Medicine, 1999.

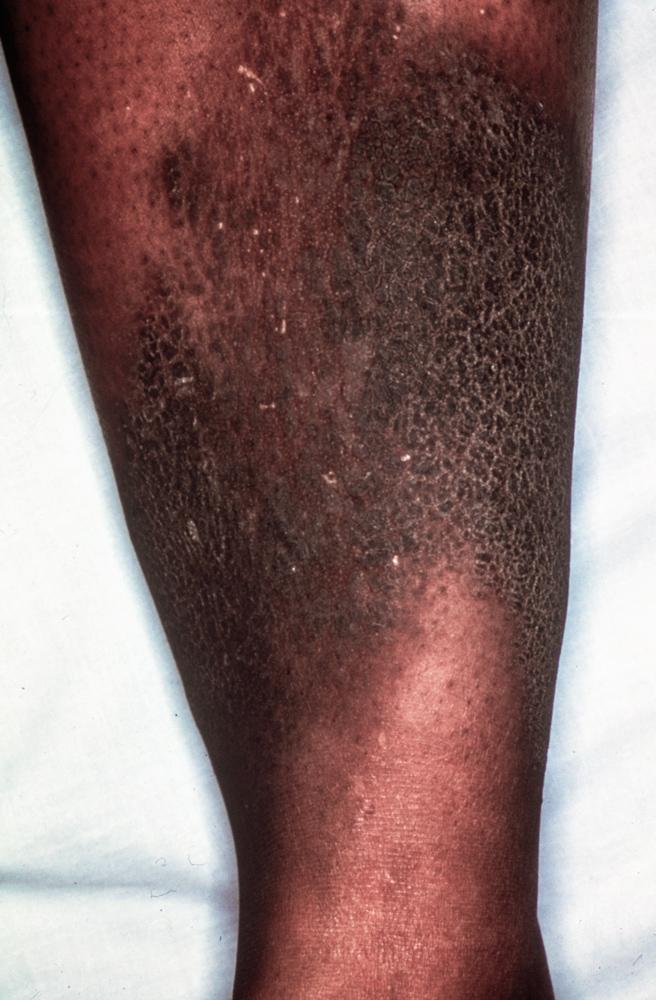
Photo courtesy of Karen McKoy, MD.


© Springer Science+Business Media


By permission of the publisher. From Burman K, Becker K, Cytryn A, et al. In Atlas of Clinical Endocrinology: Thyroid Diseases . Edited by SG Korenman (series editor) and MI Surks. Philadelphia, Current Medicine, 1999.
Thyroid storm
Thyroid storm is an acute form of hyperthyroidism that results from untreated or inadequately treated severe hyperthyroidism. It is rare, occurring in patients with Graves disease or toxic multinodular goiter (a solitary toxic nodule is a less common cause and generally causes less severe manifestations). It may be precipitated by infection, trauma, surgery, embolism, diabetic ketoacidosis, or preeclampsia.
Thyroid storm causes abrupt florid symptoms of hyperthyroidism with one or more of the following: fever, marked weakness and muscle wasting, extreme restlessness with wide emotional swings, confusion, psychosis, coma, nausea, vomiting, diarrhea, and hepatomegaly with mild jaundice. The patient may present with tachycardia or cardiovascular collapse and shock. Thyroid storm is a life-threatening emergency requiring prompt treatment.
Diagnosis of Hyperthyroidism
TSH measurement
Free T4, plus either free T3 or total T3 measurement
Sometimes radioactive iodine uptake
Diagnosis of hyperthyroidism is based on history, physical examination, and thyroid function tests. Serum TSH measurement is the best test because TSH is suppressed in patients with hyperthyroidism except in the rare instance when the etiology is a TSH-secreting pituitary adenoma or pituitary resistance to the normal inhibition by thyroid hormone.
Free T4 is increased in hyperthyroidism. However, T4 can be falsely normal in true hyperthyroidism in patients with a severe systemic illness (similar to the falsely low levels that occur in euthyroid sick syndrome) and in T3 toxicosis. If free T4 level is normal and TSH is low in a patient with subtle symptoms and signs of hyperthyroidism, then serum T3 should be measured to detect T3 toxicosis; an elevated level confirms that diagnosis.
The cause can often be diagnosed clinically (eg, the presence of signs specific to Graves disease). If not, radioactive iodine uptake by the thyroid may be measured by using iodine-123. When hyperthyroidism is due to hormone overproduction, radioactive iodine uptake by the thyroid is usually elevated (diffusely in Graves disease, focally in uninodular or multinodular goiter). When hyperthyroidism is due to thyroiditis, iodine ingestion, or overtreatment with thyroid hormones, radioactive iodine uptake is low.
TSH receptor antibodies can be measured to evaluate for Graves disease. Measurement is done in pregnant women with a history of Graves disease during the third trimester of pregnancy to assess the risk of neonatal Graves disease; TSH receptor antibodies readily cross the placenta to stimulate the fetal thyroid. Most patients with Graves disease have circulating antithyroid peroxidase antibodies, and fewer have antithyroglobulin antibodies.
Inappropriate TSH secretion is uncommon. The diagnosis is confirmed when hyperthyroidism occurs with elevated circulating free T4 and T3 concentrations and normal or elevated serum TSH.
If thyrotoxicosis factitia is suspected, serum thyroglobulin can be measured; it is usually low or low-normal—unlike in all other causes of hyperthyroidism.
Subclinical hyperthyroidism
Subclinical hyperthyroidism is low serum TSH in patients with normal serum free T4 and T3 and absent or minimal symptoms of hyperthyroidism.
Subclinical hyperthyroidism is far less common than subclinical hypothyroidism.
Patients with serum TSH < 0.1 microU/mL (0.1 mU/L) have an increased incidence of atrial fibrillation (particularly older patients), reduced bone mineral density, increased fractures, and increased mortality. Patients with serum TSH that is only slightly below normal are less likely to have these complications.
Treatment of Hyperthyroidism
Treatment of hyperthyroidism depends on the cause (1) but may include
Radioactive iodine
Beta-blockers
Iodine
Surgery
Radioactive sodium iodine (iodine-131, radioiodine)
In the United States, iodine-131 is the most common treatment for hyperthyroidism. Radioiodine is often recommended as the treatment of choice for Graves disease and toxic nodular goiter in all patients, including children. Epidemiologic studies report a very small increased risk of secondary malignancies with I-131 treatment, depending on the type of cancer and length of follow-up (2), so some clinicians use antithyroid medications instead. Dosage of iodine-131 is difficult to adjust because the response of the gland cannot be predicted; some clinicians give a standard dose of 8 to 15 millicurie. Others adjust the dose based on estimated thyroid size and the 24-hour uptake to provide a dose of 80 to 120 microcurie/g thyroid tissue.
When sufficient iodine-131 is given to cause euthyroidism, approximately 25 to 50% of patients become hypothyroid 1 year later, and the incidence continues to increase yearly. Thus, most patients eventually become hypothyroid and require thyroid hormone replacement. However, if smaller doses are used, incidence of recurrence is higher. Larger doses, such as 10 to 20 millicurie, often cause hypothyroidism within 6 months.
Radioactive iodine is not used during lactation because it can enter breast milk and cause hypothyroidism in the infant. It is not used during pregnancy because it crosses the placenta and can cause severe fetal hypothyroidism. There is no proof that radioiodine increases the incidence of tumors, leukemia, thyroid cancer, or birth defects in children born to previously hyperthyroid women who become pregnant after treatment was completed.
Methimazole and propylthiouracil
methimazole is 5 to 20 mg orally 1 to 3 times a day. Normalization of TSH lags normalization of T4 and T3 levels by weeks. Therefore, when T4 and T3 levels normalize, the dosage is decreased to the lowest effective amount, usually methimazole 2.5 to 10 mg once a day in order to avoid inducing hypothyroidism. Control generally is achieved in 2 to 3 months. Maintenance doses of methimazole may be continued for ≥ 1 years depending on the clinical circumstances. Carbimazole, which is used widely in Europe but is unavailable in the United States, is rapidly converted to methimazole. The usual starting dose is similar to that of methimazole; maintenance dosage is 2.5 to 10 mg orally once a day or 2.5 to 5 mg twice a day.
Because of severe liver failure in some patients <propylthiouracil is 100 to 150 mg orally every 8 hours. Rapid control can be achieved by increasing the dosage of propylthiouracil to 150 to 200 mg every 8 hours. Such dosages or higher ones (up to 400 mg every 8 hours) are generally reserved for severely ill patients, including those with thyroid storm, to block the conversion of T4 to T3. Maintenance dosing with propylthiouracil is 50 mg twice a day or 3 times a day
Approximately 20 to 50% of patients with Graves disease remain in remission after a 1- to 2-year course of either methimazole or propylthiouracil
% of patients, reversible agranulocytosis. Patients allergic to one medication can be switched to the other, but cross-sensitivity may occur. If agranulocytosis occurs, the patient cannot be switched to the other medication; other therapy (eg, radioiodine, surgery) should be used.
Pearls & Pitfalls
|
methimazole is used in dosages of <
methimazole
Beta-blockers
Manifestations that typically respond to beta-blockers include
Tachycardia
Tremor
Some mental symptoms (eg, anxiety)
Eyelid lag
Occasionally heat intolerance and sweating, diarrhea, and proximal myopathy also respond to beta-blockers.
Manifestations that typically do not respond to beta-blockers include
Goiter
Exophthalmos
Weight loss
Bruit
Increased oxygen consumption
Increased circulating thyroxine levels
Calcium channel blockers may control tachyarrhythmias in patients in whom beta-blockers are contraindicated.
Iodine
Complications of iodine therapy include inflammation of the salivary glands, conjunctivitis, and rash.
Surgery
Surgery is indicated for patients with Graves disease whose hyperthyroidism has recurred after courses of antithyroid medications and who refuse iodine-131 therapy, patients who cannot tolerate antithyroid medications, patients with very large goiters, and in some younger patients with toxic adenoma and multinodular goiter. Surgery may be done in older patients with giant nodular goiters.
Surgery usually restores normal function. Postoperative recurrences vary between 2 and 16%
Treatment of thyroid storm
A treatment regimen for thyroid storm is shown in the table Treatment of Thyroid Storm. The precipitating cause should also be addressed.
Treatment of infiltrative dermopathy
In infiltrative dermopathy (in Graves disease), topical corticosteroids or corticosteroid injections into the lesions may decrease the dermopathy. Dermopathy sometimes remits spontaneously after months or years.
Treatment of infiltrative ophthalmopathy
insulin-like growth factor 1 (IGF-1) receptor inhibitor, is very effective therapy for moderately severe ophthalmopathy (3). Radioiodine therapy may accelerate progression of ophthalmopathy when ophthalmopathy is active, and is thus contraindicated in this active phase.
Management of subclinical hyperthyroidism
Therapy is indicated for patients with endogenous subclinical hyperthyroidism (serum TSH < 0.1 mIU/L [ <
Treatment references
1. Ross DS, Burch HB, Cooper DS, et al: 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid 26(10):1343–1421, 2016. doi: 10.1089/thy.2016.0229
2. Shim SR, Kitahara CM, Cha ES, Kim SJ, Bang YJ, Lee WJ: Cancer Risk After Radioactive Iodine Treatment for Hyperthyroidism: A Systematic Review and Meta-analysis. JAMA Netw Open 4(9):e2125072, 2021. doi:10.1001/jamanetworkopen.2021.25072
3. Douglas RS, Kahaly GJ, Patel A, et al: Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med 382(4):341–352. 2020. doi: 10.1056/NEJMoa1910434
Key Points
The most common etiology of hyperthyroidism is Graves disease, caused by autoimmune-stimulated excessive hormone synthesis by the thyroid gland.
Other causes of hyperthyroidism include excessive stimulation of a normal thyroid gland (eg, by thyroid-stimulating hormone [TSH], human chorionic gonadotrophin [hCG], ingestion of iodine or iodine-containing drugs), excessive hormone synthesis by an abnormal thyroid (eg, toxic nodular goiter), excessive release of thyroid hormones (eg, due to thyroiditis), or ingestion of excessive quantities of thyroid hormone.
Symptoms and signs include tachycardia, fatigue, weight loss, nervousness, and tremor; patients with Graves disease may also have exophthalmos and infiltrative dermopathy.
Free thyroxine (T4), and/or free or total triiodothyronine (T3) are elevated, and TSH is suppressed (except in rarer cases of pituitary causes of hyperthyroidism).
Thyroid storm—resulting from untreated or inadequately treated severe hyperthyroidism—is a life-threatening emergency that presents with severe symptoms of hyperthyroidism and may result in cardiovascular collapse or shock; it is treated with a regimen of antithyroid medications, iodine, beta-blockers, corticosteroids, and hemodynamic support.






