


(See also Overview of Adrenal Function.)
Addison disease develops in approximately 4/100,000 people annually (1). It occurs in all age groups, about equally in each sex, and tends to become clinically apparent during metabolic stress, infection, or trauma.
Adrenal crisis (onset of severe symptoms) may be precipitated by acute infection. Infection is a common cause, especially when there is septicemia. Other causes include trauma, surgery, and sodium loss due to excessive sweating. Even with treatment, Addison disease may cause a slight increase in mortality. It is not clear whether this increase is due to mistreated adrenal crises or long-term complications of inadvertent over-replacement.
General reference
1. Alexandraki KI, Sanpawithayakul K, Grossman A. Adrenal Insufficiency. [Updated 2022 Nov 7]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279083/
Etiology of Addison Disease
Approximately 70% of cases in the United States are due to idiopathic atrophy of the adrenal cortex, probably caused by autoimmune processes (1). The remainder result from destruction of the adrenal gland by granuloma (eg, tuberculosis, histoplasmosis), tumor, amyloidosis
Addison disease may coexist with diabetes mellitus or hypothyroidism in polyglandular deficiency syndrome. In children, the most common cause of primary adrenal insufficiency is congenital adrenal hyperplasia.
Etiology reference
1. Kemp WL, Koponen MA, Meyers SE. Addison Disease: The First Presentation of the Condition May be at Autopsy. Acad Forensic Pathol 2016;6(2):249-257. doi:10.23907/2016.026
Pathophysiology of Addison Disease
Both mineralocorticoids and glucocorticoids are deficient.
Mineralocorticoid deficiency
Because mineralocorticoids stimulate sodium reabsorption and potassium excretion, deficiency results in increased excretion of sodium and decreased excretion of potassium, chiefly in urine but also in sweat, saliva, and the gastrointestinal tract. A low serum concentration of sodium (hyponatremia) and a high concentration of potassium (hyperkalemia) result.
Urinary salt and water loss cause severe dehydration, plasma hypertonicity, acidosis, decreased circulatory volume, hypotension, and, eventually, circulatory collapse. However, when adrenal insufficiency is caused by inadequate adrenocorticotropic hormone (ACTH) production (secondary adrenal insufficiency), electrolyte levels are often normal or only mildly deranged, and the circulatory problems are less severe.
Glucocorticoid deficiency
Glucocorticoid deficiency contributes to hypotension and causes severe insulin sensitivity and disturbances in carbohydrate, fat, and protein metabolism. In the absence of cortisol, insufficient carbohydrate is formed from protein; hypoglycemia and decreased liver glycogen result. Weakness follows, due in part to deficient neuromuscular function. Resistance to infection, trauma, and other stress is decreased. Myocardial weakness and dehydration reduce cardiac output, and circulatory failure can occur.
A decreased blood cortisol level results in increased pituitary ACTH production and increased blood beta-lipotropin level. Beta-lipotropin has melanocyte-stimulating activity and, together with ACTH, causes the hyperpigmentation of skin and mucous membranes characteristic of Addison disease. Thus, adrenal insufficiency secondary to pituitary failure does not cause hyperpigmentation.
Symptoms and Signs of Addison Disease
Weakness, fatigue, and orthostatic hypotension are early symptoms and signs of Addison disease.
Hyperpigmentation is characterized by diffuse darkening of exposed and, to a lesser extent, unexposed portions of the body, especially on pressure points (bony prominences), skin folds, scars, and extensor surfaces. Black freckles are common on the forehead, face, neck, and shoulders. Bluish black discolorations of the areolae and mucous membranes of the lips, mouth, rectum, and vagina occur.

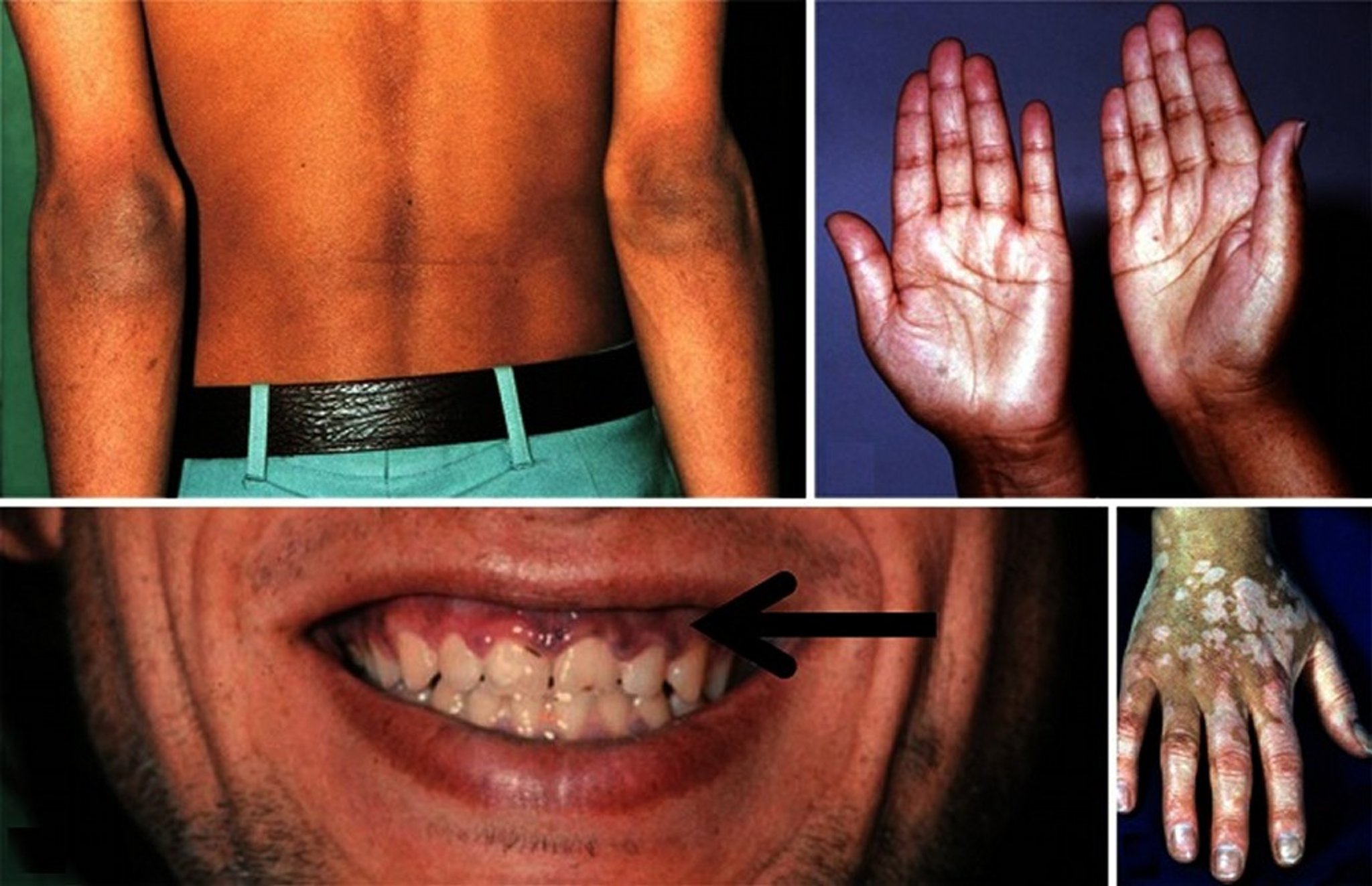
© Springer Science+Business Media
Anorexia, nausea, vomiting, and diarrhea often occur. Decreased tolerance to cold, with hypometabolism, may be noted. Dizziness and syncope may occur.
The gradual onset and nonspecific nature of early symptoms often lead to an incorrect initial diagnosis of neurosis.
Weight loss, dehydration, and hypotension are characteristic of the later stages of Addison disease.
Adrenal crisis
Adrenal crisis is characterized by
Profound asthenia (weakness)
Severe pain in the abdomen, lower back, or legs
Peripheral vascular collapse
Renal shutdown with azotemia
Body temperature may be low, although severe fever often occurs, particularly when crisis is precipitated by acute infection.
A significant number of patients with partial loss of adrenal function (limited adrenocortical reserve) appear well but experience adrenal crises when under physiologic stress (eg, surgery, infection, burns, critical illness). Shock and fever may be the only signs.
Diagnosis of Addison Disease
Electrolyte levels
Serum cortisol
Plasma adrenocorticotropic hormone (ACTH)
Sometimes ACTH stimulation testing
Clinical symptoms and signs suggest adrenal insufficiency. Sometimes the diagnosis is considered only on discovery of characteristic abnormalities of serum electrolytes, including low sodium, high potassium , low bicarbonate, and high BUN (blood urea nitrogen—see table Test Results That Suggest Addison Disease).
Test Results That Suggest Addison Disease
Test | Result |
|---|---|
Blood chemistry | |
Serum sodium | < 135 mEq/L (< 135 mmol/L) |
Serum potassium | > 5 mEq/L (> 5 mmol/L) |
Ratio of serum sodium:potassium | < 30:1 |
Plasma glucose, fasting | < 50 mg/dL (< 2.8 mmol/L) |
Plasma bicarbonate | < 15–20 mEq/L (< 15–20 mmol/L) |
BUN (blood urea nitrogen) | > 20 mg/dL (> 7.1 mmol/L) |
Hematology | |
Hematocrit | Elevated |
White blood cell count | Low |
Lymphocytes | Relative lymphocytosis |
Eosinophils | Increased |
Imaging | |
X-ray or CT of adrenals | Evidence of
|
Differential diagnosis
The varied manifestations of Addison disease can also be caused by numerous other disorders.
Hyperpigmentation can result from
Ingestion of heavy metals (eg, iron, silver)
Chronic skin conditions
Hemochromatosis (although the hyperpigmentation of iron overload may be partly due to adrenal insufficiency caused by iron deposition in the adrenals)
Peutz-Jeghers syndrome, which is characterized by pigmentation of the buccal and rectal mucosa
Vitiligo, although diseases other than Addison disease can cause vitiligo
Weakness resulting from Addison disease subsides with rest, unlike neuropsychiatric weakness, which is often worse in the morning than after activity. Most myopathies that cause weakness can be differentiated by their distribution, lack of abnormal pigmentation, and characteristic laboratory findings (see also Weakness).
Patients with adrenal insufficiency develop hypoglycemia after fasting because of decreased gluconeogenesis and often show weight loss, which is not fully understood, but due at least in part to extracellular volume deficiency. In contrast, patients with hypoglycemia due to oversecretion of insulin usually have increased appetite with weight gain, and have normal adrenal function.
Low serum sodium due to Addison disease must be differentiated from that of edematous patients with cardiac or liver disease (particularly those taking diuretics), the dilutional hyponatremia of the syndrome of inappropriate antidiuretic hormone secretion (SIADH), and salt-losing nephropathy. Unlike those with Addison disease, these patients are not likely to have hyperpigmentation, hyperkalemia, and increased BUN.
Testing
Laboratory tests, beginning with morning serum cortisol and plasma ACTH levels, confirm adrenal insufficiency (see table Confirmatory Serum Testing for Addison Disease). Elevated ACTH (≥ 50 pg/mL [≥ 11 pmol/L]) with low cortisol (< 5 mcg/dL [< 138 nmol/L]) is diagnostic, particularly in patients who are severely stressed or in shock. Low ACTH (< 5 pg/mL [< 1.1 pmol/L] ) and low cortisol suggest secondary adrenal insufficiency. It is important to note that ACTH levels within the normal range are inappropriate when cortisol levels are very low.
Provocative testing
Addison disease is diagnosed by showing failure of exogenous ACTH to increase serum cortisol. Secondary adrenal insufficiency is diagnosed by a prolonged ACTH stimulation test, glucagon stimulation test, or insulin tolerance test.
ACTH stimulation testingsecondary adrenal insufficiency
Normal preinjection serum cortisol levels vary somewhat depending on the laboratory assay in use but typically range from 5 to 25 mcg/dL (138 to 690 nmol/L) and double in 30 to 90 minutes, reaching at least 20 mcg/dL (552 nmol/L). Patients with Addison disease have low or low-normal preinjection values that do not rise above a peak value of 15 to 18 mcg/dL (414 to 497 nmol/L) at 30 minutes. However, the precise normal values depend on the specific cortisol assay used, and the normal range should be verified for each laboratory.
In the glucagon stimulation test, plasma ACTH and cortisol levels fail to rise in response to glucagon in patients with secondary adrenal insufficiency.
In the insulin tolerance test, ACTH and cortisol fail to rise in response to enough intravenous regular insulin to cause a reduction in blood glucose to a critical level. The tolerance test carries a risk for hypoglycemic seizure and is not recommended in patients suspected of having severe adrenal insufficiency.
Confirmatory Serum Testing for Addison Disease
Test | Result |
|---|---|
Plasma ACTH | High (≥ 50 pg/mL [≥ 11 pmol/L]) |
Serum cortisol | Low (< 5 mcg/dL [< 138 nmol/L]) |
ACTH stimulation test | Subnormal (ie, 30-minute cortisol should be < 15–18 mcg/dL [< 414–497 nmol/L], according to the assay) |
Prolonged (24-hour) ACTH stimulation test | Cortisol should be subnormal at 1 hour and should not rise further at 24 hours |
ACTH = adrenocorticotropic hormone. | |
A subnormal response to cosyntropin may occur in secondary adrenal insufficiency. However, because pituitary failure may cause adrenal atrophy (and hence failure to respond to ACTH), if pituitary disease is suspected, the patient may need to be primed with long-acting ACTH 1 mg IM once a day for 3 days before the ACTH stimulation test. After such priming, there should be a normal response to the test with a rise in serum cortisol to > 20 mcg/dL (> 552 nmol/L), although this threshold is assay dependent.
A prolonged ACTH stimulation test≥ 24 hours. Only in cases of prolonged adrenal atrophy is adrenal priming (with long-acting ACTH) necessary. The simple short test is usually done initially, because a normal response obviates the need for further investigation.
If adrenal crisis is suspected, confirmation of Addison disease by ACTH stimulation testing is deferred until the patient has recovered. If ACTH stimulation testing is done, elevated ACTH levels together with low cortisol levels confirm the diagnosis.
Testing for etiology
In areas where granulomatous causes are less likely, the cause is usually assumed to be autoimmune, unless there is evidence otherwise. Adrenal autoantibodies can be assessed. In autoimmune Addison disease, adrenal antibodies are often positive, at least initially.
Where granulomatous causes are more likely, tuberculosis is a common cause, so a chest x-ray should be done; if doubt exists, CT of the adrenals is helpful. In patients with autoimmune disease, the adrenals are atrophied, whereas in patients with tuberculosis or other granulomas, the adrenals are enlarged (initially) with frequent calcification. Bilateral adrenal hyperplasia, particularly in children and young adults, suggests a genetic enzyme defect. Adrenal hemorrhage is usually obvious on CT scanning.
Treatment of Addison Disease
Dose increase during intercurrent illness
aldosterone. The easiest way to adjust the fludrocortisone dosage is to titrate it to normalize blood pressure and serum potassium levels. Normal hydration and absence of orthostatic hypotension are evidence of adequate replacement therapy. In some patients, fludrocortisone causes hypertension, which is treated by reducing the dosage or starting a nondiuretic antihypertensive. Adequate doses of fludrocortisone should be given even if use requires the addition of antihypertensives.
hydrocortisone and taught to self-administer parenteral hydrocortisone for urgent situations. A preloaded syringe with 100 mg hydrocortisone should be available to the patient for intramuscular or subcutaneous administration. A bracelet or wallet card giving the diagnosis and corticosteroid dose may help in case of adrenal crisis that renders the patient unable to communicate.
> 30 mg/day. Higher doses of hydrocortisone increase insulin requirements.
Treatment of adrenal crisis
Therapy should be instituted immediately upon suspicion of adrenal crisis. (CAUTION: In adrenal crisis, a delay in instituting corticosteroid therapy, particularly if there is hypoglycemia and hypotension, may be fatal.) If the patient is acutely ill, confirmation by an ACTH stimulation test should be postponed until the patient has recovered.
hydrocortisone is given. Subsequently, hydrocortisone 50 or 100 mg IM every 6 hours can be given.
hydrocortisone per hour with measurement of serum cortisol. Restoration of blood pressure and general improvement should occur within 1 hour after the initial dose of hydrocortisone. Inotropic agents may be needed until the effects of hydrocortisone are achieved.
hydrocortisone
Recovery depends on treatment of the underlying cause (eg, infection, trauma, metabolic stress) and adequate hydrocortisone therapy.
Pearls & Pitfalls
|
Treatment of complications
Fever > 40.6° C occasionally accompanies the rehydration process. An oral antipyretic may be given.
Key Points
Addison disease is primary adrenal insufficiency.
Weakness, fatigue, and hyperpigmentation (generalized darkening or focal black spots involving skin and mucous membranes) are typical.
Low serum sodium, high serum potassium, and high BUN (blood urea nitrogen) occur.
Usually, plasma adrenocorticotropic hormone (ACTH) is high and serum cortisol levels are low.






