


Bullous keratopathy is the presence of corneal epithelial bullae, resulting from corneal endothelial disease.
Etiology of Bullous Keratopathy
Bullous keratopathy is caused by edema of the cornea, resulting from failure of the corneal endothelium to maintain the normally transparent, dehydrated state of the cornea. Most frequently, it is due to Fuchs corneal endothelial dystrophy or corneal endothelial trauma.
Fuchs dystrophy is a genetic disorder that causes bilateral, progressive corneal endothelial cell loss, sometimes leading to symptomatic bullous keratopathy by age 50 to 60. Fuchs dystrophy may be autosomal dominant with incomplete penetrance.
Corneal endothelial trauma can occur during intraocular surgery (eg, cataract removal) or after placement of a poorly designed or malpositioned intraocular lens implant. Bullous keratopathy after cataract removal is called pseudophakic (if an intraocular lens implant is present) or aphakic (if no intraocular lens implant is present) bullous keratopathy.

© Springer Science+Business Media
Symptoms and Signs of Bullous Keratopathy
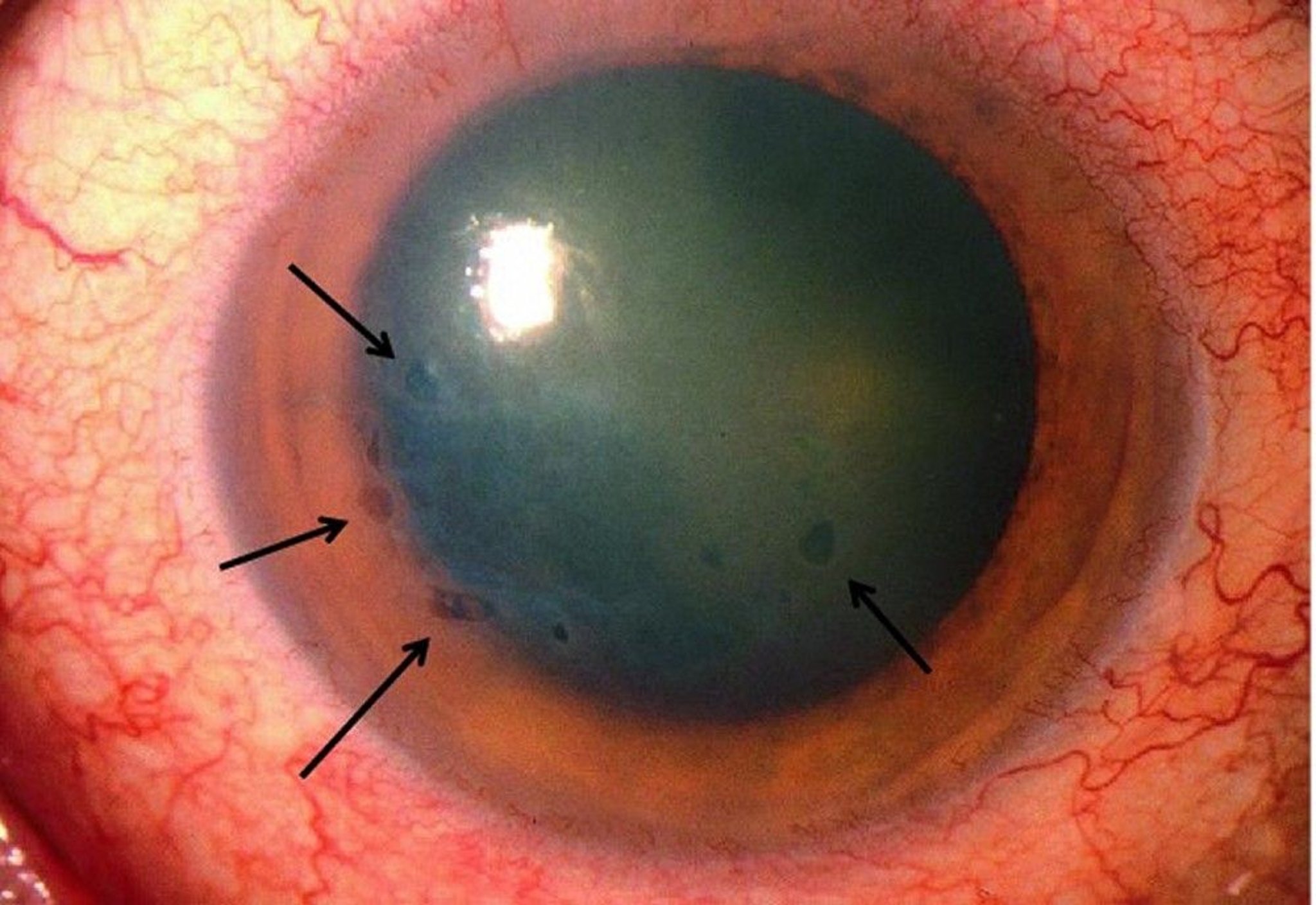
Subepithelial fluid-filled bullae form on the corneal surface as the corneal stroma (the deeper dense connective tissue layer of the cornea) swells, leading to decreased visual acuity, loss of contrast, glare, and photophobia. Sometimes bullae rupture, causing pain and foreign body sensation. Bacteria can invade a ruptured bulla, leading to a corneal ulcer.
Diagnosis of Bullous Keratopathy
Slit-lamp examination
Ultrasonic pachymetry
Slit-lamp examination of all types of bullous keratopathy reveals corneal epithelial bullae and swelling of the corneal stroma. Fuchs dystrophy also demonstrates multiple minute excrescences (guttata) on the endothelial surface and/or thickening of Descemet's membrane, giving a “beaten metal” appearance to the back surface of the cornea. All the symptoms and findings are characteristically worse when patients first wake up and improve throughout the day. This is because moisture accumulates—and edema worsens—when the eyes are closed during sleep and progressively dries by evaporation when the eyes are open.
Also required for diagnosis of all types of bullous keratopathy is increased corneal thickness as measured by ultrasonic pachymetry.
Treatment of Bullous Keratopathy
Topical hypertonic agents, drugs to lower intraocular pressure, and corneal transplantation
corneal transplantation is usually curative.
Key Points
Bullous keratopathy is caused by edema of the cornea, most frequently due to Fuchs corneal endothelial dystrophy or corneal endothelial trauma.
Subepithelial fluid-filled bullae form, leading to decreased visual acuity, loss of contrast, glare, and photophobia.
Slit-lamp examination reveals corneal epithelial bullae and swelling of the corneal stroma.
Treatment by an ophthalmologist is required.






