


In patients with renal disorders, symptoms and signs may be nonspecific, absent until the disorder is severe, or both. Findings can be local (eg, reflecting kidney inflammation or mass), result from the systemic effects of kidney dysfunction, or affect urination (eg, changes in urine itself or in urine production). (See also Evaluation of the Urologic Patient.)
History in the Renal Patient
History plays a limited role because symptoms are nonspecific.
Hematuria is relatively specific for a genitourinary disorder, but patients who report red urine may instead have one of the following:
Myoglobinuria
Hemoglobinuria
Porphyrinuria
Porphobilinuria
Food-induced urine coloring (some foods, eg, beets, rhubarb, sometimes food coloring, may make urine appear red)
High concentrations of urinary protein cause frothy or sudsy urine. Urinary frequency (voiding more often) should be distinguished from polyuria (voiding a larger amount than normal) in patients who report excessive urination. Nocturia may be a feature of either but is often the result of excess fluid intake too close to bedtime, prostate enlargement, or chronic kidney disease. Family history is useful for identifying inheritance patterns and risk of polycystic kidney disease or other hereditary nephropathies (eg, hereditary nephritis, thin basement membrane disease, nail-patella syndrome, cystinuria, hyperoxaluria). Flank pain can be secondary to pyelonephritis or obstruction due to renal calculi.
Physical Examination of the Renal Patient
Patients with moderate or severe chronic kidney disease sometimes appear pale, wasted, or ill. Deep (Kussmaul) respiration suggests hyperventilation in response to metabolic acidosis with acidemia. Patients with nephrotic syndrome and fluid overload can present with periorbital swelling and edema of extremities.
Chest examination
Pericardial and pleuritic friction rubs may be signs of uremia. Patients can present with lung crackles secondary to pulmonary edema from fluid retention in acute or chronic kidney disease.
Abdominal examination
Visible fullness of the upper abdomen is an unusual, nonspecific finding of polycystic kidney disease. It may also indicate a kidney or abdominal mass. A soft, lateralizing bruit is occasionally audible in the epigastrium or the flank in renal artery stenosis; presence of a diastolic component increases the probability of renovascular hypertension.
Pain elicited by mild striking of the back, flanks, and angle formed by the 12th rib and lumbar spine with a fist (costovertebral tenderness) may indicate pyelonephritis or urinary tract obstruction (eg, due to calculi). Normal kidneys are not usually palpable. However, in some women, the lower pole of the right kidney can occasionally be felt with palpation during deep inspiration, and large kidneys or masses can sometimes be felt without special maneuvers. In neonates, the kidneys can be felt with the thumbs when the thumbs are placed anterior and the fingers posterior to the costovertebral angle.
Transillumination can distinguish solid from cystic renal masses in some children < 1 year old if the kidney and mass are manipulated against the abdominal wall.
Skin examination
Chronic kidney disease can cause any of the following:
Xerosis due to sebaceous and eccrine sweat gland atrophy
Pallor due to anemia
Hyperpigmentation due to melanin deposition
Sallow or yellow-brown skin due to urochrome deposition
Petechiae or ecchymoses due to platelet dysfunction
Excoriation due to itching caused by hyperphosphatemia or uremia


© Springer Science+Business Media
Neurologic examination
Patients with acute renal failure may be drowsy, confused, or inattentive; speech may be slurred. Asterixis can be detected in handwriting or by observation of outstretched hands maximally extended at the wrists; after several seconds in this position, a hand flap in the flexor direction is asterixis. Asterixis suggests one of the following:
Chronic liver failure
Carbon dioxide narcosis
Toxic encephalopathy
Testing of the Renal Patient
The initial steps in evaluation of renal disorders are:
Urinalysis
Serum creatinine level
Other urine, blood, and imaging tests (eg, ultrasonography, CT, MRI) are done in specific circumstances. Ideally, after the urethral meatus is cleaned, the urine specimen is collected midstream (clean-catch specimen) during the first void of the morning; the urine should be examined immediately because delays can lead to changes in test results. Bladder catheterization or suprapubic aspiration can be used for collection when urine cannot be obtained by spontaneous voiding or when vaginal material contaminates the urine specimen. However, the trauma of catheterization may falsely increase the number of red blood cells (RBCs) in the specimen, so catheterization is usually avoided if the outcome of interest is microscopic hematuria. A specimen from a catheter collection bag is not acceptable for microscopic or bacteriologic tests.
Urinalysis
A complete urinalysis includes the following:
Inspection for color, appearance, and odor
Measurement of pH, specific gravity, protein, glucose, hemoglobin (suggesting RBCs), nitrites, and white blood cell (WBC) esterase by dipstick reagents
Microscopic analysis for casts, crystals, and cells (urine sediment)
Bilirubin and urobilinogen, although standard parts of many dipstick tests, no longer play significant roles in evaluation of renal or hepatic disorders.
Color is the most obvious of urine attributes, and observation of color is an integral part of urinalysis (see table Causes of Urine Color Changes). Urine color may suggest possible causes and help direct additional testing.
Odor, often unintentionally noted during visual inspection, conveys useful information only in rare cases of inherited disorders of amino acid metabolism when urine has a distinctive smell (eg, maple syrup in maple syrup urine disease, sweaty feet in isovaleric acidemia, tomcat urine in multiple carboxylase deficiency [see table Branched-Chain Amino Acid Metabolism Disorders]).
pH is normally 5.0 to 6.0 (range 4.5 to 8.0). Measuring with a glass pH electrode is recommended when precise values are necessary for decision making, as when diagnosing renal tubular acidosis
Specific gravity provides a rough measure of urine concentration (osmolality). Normal range is 1.001 to 1.035; values may be low in older patients or in those with impaired renal function, who are less able to concentrate urine. It is measured by hydrometer or refractometer or estimated with a dipstick. Accuracy of the dipstick test is controversial, but the test may be sufficient for patients who have calculi and are advised to self-monitor urine concentration to maintain dilute urine. Specific gravity by dipstick may be spuriously elevated when urine pH is < 6 or low when pH is >
Protein< 10 mg/dL), trace (15 to 30 mg/dL), or 1+ (30 to 100 mg/dL) through 4+ (> 500 mg/dL). Moderately increased albuminuria (formerly known as microalbuminuria), an important marker for renal complications in patients with diabetes, is not detected by standard dipsticks, but special microalbumin dipsticks are available. Light-chain proteins (eg, due to multiple myeloma) also are not detected. Significance of proteinuria depends on total protein excretion rather than protein concentration estimated by dipstick; thus, when proteinuria is detected with dipstick testing, quantitative measures of urinary protein should be done. False-negative results can be caused by dilute urine. False-positive results can be caused by any of the following:
High pH (> 9)
Presence of cells
Radiopaque contrast agents
Concentrated urine
Glucose usually appears in the urine when serum glucose increases to > 180 mg/dL (> 10.0 mmol/L) and renal function is normal. Threshold for detection by urine dipstick is 50 mg/dL (2.8 mmol/L). Any amount is abnormal. Falsely low or negative results can result from any of the following:
Ketones
Very high urine pH
Dilute urine
Glucose can appear in the urine despite normal plasma glucose levels in Fanconi syndrome (proximal tubule defect), renal glucosuria, and with use of sodium-glucose co-transporter 2 (SGLT2) inhibitor.
Hematuria is detected when RBCs lyse on a dipstick test strip, releasing hemoglobin (Hb) and causing a color change. Range is from negative (0) to 4+. Trace blood (corresponding to 3 to 5 RBCs/high-power field [HPF]) is normal under some circumstances (eg, exercise) in some people. Because the test strip reagent reacts with Hb, free Hb (eg, due to intravascular hemolysis) or myoglobin (eg, due to rhabdomyolysis
Nitrites are produced when bacteria reduce urinary nitrates derived from amino acid metabolism. Nitrites are not normally present and signify bacteriuria. The test is either positive or negative. False-negative results may occur with any of the following:
Infection with certain pathogens that cannot convert nitrate to nitrite (eg, Enterococcus faecalis, Neisseria gonorrhoeae, Mycobacterium tuberculosis)
Urine that has not stayed long enough (< 4 hours) in the bladder
Low urinary excretion of nitrate
Enzymes (of certain bacteria) that reduce nitrates to nitrogen
High urine urobilinogen level
Urine pH < 6.0
Nitrites are used mainly with WBC esterase testing to monitor patients with recurrent urine infections, particularly children with vesicoureteral reflux, and sometimes to confirm the diagnosis of uncomplicated urinary tract infection (UTI) in women of childbearing age.
WBC esterase is released by lysed neutrophils. Its presence in urine reflects acute inflammation, most commonly due to bacterial infection but sometimes due to interstitial nephritis, nephrolithiasis, or renal tuberculosis. Threshold for detection is about 5 WBCs/HPF, and test results range from negative to 4+. The test is not very sensitive for detection of infection. Contamination of a urine specimen with vaginal flora is the most common cause of false-positive results. False-negative results may result from any of the following:
Very dilute urine
Glycosuria
Urobilinogen
WBC esterase is used mainly with nitrite testing to monitor patients with recurrent urine infections and sometimes to diagnose uncomplicated UTI in women of childbearing age. If both tests are negative, the likelihood of a positive urine culture is small.
Microscopic urine analysis
Detection of solid elements (cells, casts, crystals) requires microscopic analysis, ideally done immediately after voiding, and dipstick testing. The specimen is prepared by centrifuging 10 to 15 mL of urine at 1500 to 2500 rpm for 5 minutes. The supernatant is fully decanted; a small amount of urine remains with the residue at the bottom of the centrifuge tube. The residue can be mixed back into solution by gently agitating the tube or tapping the bottom. A single drop is pipetted onto a slide and covered with a coverslip. For routine microscopic analysis, staining is optional. The specimen is examined under reduced light with the low-power objective and under full-intensity light with the high-power objective; the latter is typically used for semiquantitative estimates (eg, 10 to 15 WBCs/high power field [HPF]). Polarized light is used to identify some crystals and lipids in the urine. Phase-contrast microscopy enhances identification of cells and casts.
Epithelial cells (renal tubular, transitional, squamous cells) frequently are found in urine; most common are squamous cells lining the end of the urethra and contaminants from the vagina. Only renal tubular cells are diagnostically important; however, except when found in casts, they are difficult to distinguish from transitional cells. A few renal tubular cell casts appear in normal urine, but a large number suggests tubular injury (eg, acute tubular necrosis, tubulointerstitial nephritis, nephrotoxins, nephrotic syndrome).
RBCs < 3/HPF may be normal (< 5/HPF is sometimes normal, eg, after exercise), and any isolated hematuria should be interpreted in clinical context. On microscopic analysis, glomerular RBCs are smaller and dysmorphic, with spicules, folding, and blebs; nonglomerular RBCs retain their normal shape and size.
WBCs < 5/HPF may be normal; special staining can distinguish eosinophils from neutrophils (see Other urine tests). Pyuria is defined as > 5 WBCs /HPF in a sample of centrifuged urine.
Lipiduria is most characteristic of the nephrotic syndrome; renal tubular cells absorb filtered lipids, which appear microscopically as oval fat bodies, and cholesterol, which produces a Maltese cross pattern under polarized light. Lipids and cholesterol can also be free floating or incorporated into casts.
Crystals in urine are common and usually clinically insignificant (see table Common Types of Urinary Crystals). Crystal formation depends on all of the following:
Urine concentration of crystal constituents
pH
Absence of crystallization inhibitors
Drugs are an underrecognized cause of crystals (see table Drugs That Cause Crystal Formation).
Casts are made up of glycoprotein of unknown function (Tamm-Horsfall protein) secreted from the thick ascending loop of Henle. Casts are cylindrical and have regular margins. Their presence indicates renal origin, which may be helpful diagnostically. Types of casts differ in constituents and appearance (see table Urinary Casts).
Other urine tests
Other tests are useful in specific instances.
Total protein excretion can be measured in a 24-hour collection or can be estimated by the protein/creatinine ratio, which, in a random urine sample, correlates well with values in g/1.73 m2 BSA (body surface area) from a 24-hour collection (eg, 400 mg/dL protein and 100 mg/dL creatinine in a random sample equal 4 g/1.73 m2 in a 24-hour collection). The protein/creatinine ratio is less accurate when creatinine excretion is significantly increased (eg, in muscular athletes) or decreased (eg, in cachexia).
Moderately increased albuminuria (formerly known as microalbuminuria)> 300 mg/day (>> 30 mg/g (> 0.03 mg/mg) suggests moderately increased albuminuria. The reliability of the test is best when a midmorning specimen is used, vigorous exercise is avoided before the test (because vigorous exercise can cause transient dipstick positivity for protein), and unusual creatinine production (in cachectic or very muscular patients) is not present. Moderately increased albuminuria can occur in all of the following:
Moderately increased albuminuria is an early stage of diabetic kidney disease in both type 1 and 2 diabetes; the progression of renal disease is more predictable in type 1 than 2 disease. moderately increased albuminuria is a risk factor for cardiovascular disorders and early cardiovascular mortality independent of diabetes or hypertension.
Sulfosalicylic acid+ (flocculent precipitates). Readings are falsely elevated by radiopaque contrast agents.
KetonesN
Osmolality, the total number of solute particles per unit mass (mOsm/kg [mmol/kg]), can be measured directly by osmometer. Normally, osmolality is 50 to 1200 mOsm/kg (or 50 to 1200 mmol/kg). Measurement is most useful for evaluating hypernatremia, hyponatremia, syndrome of inappropriate antidiuretic hormone secretion (SIADH), and diabetes insipidus.
Electrolyte measurements help diagnose specific disorders. Sodium (Na) level can help distinguish whether volume depletion (urine Na < 10 mEq/L [10 mmol/L]) or acute tubular necrosis (urine Na > 40 mEq/L [40 mmol/L]) is the cause of acute renal insufficiency or failure. The fractional excretion of Na (FENa) is the percentage of filtered Na that is excreted. It is calculated as the ratio of excreted to filtered Na, which can be simplified to the following:

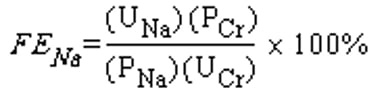
where UNa is urine Na, PNa is plasma Na, PCr is plasma creatinine, and UCr is urine creatinine.
This ratio is a more reliable measure than UNa alone because UNa levels between 10 and 40 mEq/L (or 10 and 40 mmol/L) are nonspecific. FENa < 1% suggests prerenal causes, such as volume depletion; however, acute glomerulonephritis or certain types of acute tubular necrosis (eg, rhabdomyolysis, radiocontrast-induced renal failure) and acute partial obstruction can result in FENa < 1%. A value > 2% suggests intrarenal causes such as acute tubular necrosis or acute interstitial nephritis. Values between 1 and 2 are indeterminate and can result, for example, from early acute tubular necrosis or from prerenal causes in patients who are taking diuretics or who have chronic kidney disease.
Other useful measurements include the following:
Fractional excretion of bicarbonate (HCO3) in evaluation of renal tubular acidosis
Chloride (Cl) levels for diagnosis of metabolic alkalosis
Urine anion gap in evaluation of metabolic acidosis
Potassium (K) levels in determining the cause of hypokalemia or hyperkalemia
Levels of sodium, calcium, magnesium, uric acid, oxalate, citrate, and cystine in evaluation of calculi
Eosinophils, cells that stain bright red or pink-white with Wright or Hansel staining, most commonly indicate one of the following:
Acute prostatitis
Cytology is used for the following:
To screen for cancer in high-risk populations (eg, petrochemical workers)
To evaluate persistent painless hematuria of unclear etiology after cystoscopy in the absence of glomerular disease (suggested by the absence of dysmorphic RBCs, proteinuria, and renal failure) in patients with irritative voiding symptoms
Sensitivity is about 90% for carcinoma in situ; however, sensitivity is considerably lower for low-grade transitional cell carcinomas. Inflammatory or reactive hyperplastic lesions or cytotoxic drugs for carcinoma may produce false-positive results. Accuracy for detecting bladder tumors may be increased by vigorous bladder lavage with a small volume of 0.9% saline solution (50 mL pushed in and then aspirated by syringe through a catheter). Cells collected in the saline are concentrated and examined.
Gram stain and cultures with susceptibility testing are indicated when genitourinary tract infections are suspected; a positive result must be interpreted in the clinical context (see Introduction to Urinary Tract Infections [UTIs]).
Amino acids are normally filtered and reabsorbed by the proximal tubules. They may appear in urine when a hereditary or acquired tubular transport defect (eg, Fanconi syndrome, cystinuria) is present. Measuring type and amount of amino acids may help in the diagnosis of certain types of calculi, renal tubular acidosis, and inherited disorders of metabolism.
Blood tests
Blood tests are useful in evaluation of renal disorders.
Serum creatinine values > 1.3 mg/dL (> 114 micromol/L) in men and > 1 mg/dL (> 88.4 micromol/L) in women are usually abnormal. Serum creatinine depends on creatinine generation as well as renal creatinine excretion. Because creatinine turnover increases with higher muscle mass, muscular people have higher serum creatinine levels and older and undernourished people have lower levels.
Serum creatinine may also be increased in the following conditions:
Use of angiotensin-converting enzyme (ACE) inhibitors and (ARBs)
Consumption of large amounts of meat
ACE inhibitors and ARBs reversibly decrease glomerular filtration rate (GFR) and increase serum creatinine because they vasodilate efferent more than afferent glomerular arterioles, mainly in people who are dehydrated or are receiving diuretics. In general, serum creatinine alone is not a good indicator of kidney function. The Cockcroft-Gault formula and the Modification of Diet in Renal Disease (MDRD) formula estimate GFR based on serum creatinine and other parameters and more reliably evaluate kidney function.
is used to distinguish prerenal from renal or postrenal (obstructive) azotemia; a value > 15 is considered abnormal and may occur in prerenal and postrenal azotemia. However, BUN is affected by protein intake and by several nonrenal processes (eg, trauma, infection, gastrointestinal [GI] bleeding, corticosteroid use) and, although suggestive, is generally inconclusive as evidence of renal dysfunction.
Cystatin C, a serine proteinase inhibitor that is produced by all nucleated cells and filtered by the kidneys, can also be used to evaluate kidney function. Its plasma concentration is independent of sex, age, and body weight. Testing is not always available, and values are not standardized across laboratories. Measurement of cystatin C is used to confirm chronic kidney disease in specific circumstances when eGFR calculations based on serum creatinine are less accurate and/or when eGFR is 45 to 59 mL/min with no markers of kidney damage present.
Serum electrolytes (eg, sodium [Na], potassium [K], bicarbonate [HCO3]) may become abnormal and the anion gap (Na – [Cl +HCO3]) may increase in acute kidney injury and chronic kidney disease. Serum electrolytes should be monitored periodically in patients with renal disorders.
Complete blood count (CBC) may detect anemia in chronic kidney disease or, rarely, polycythemia in renal cell carcinoma or polycystic kidney disease. Anemia is often multifactorial (mainly due to erythropoietin deficiency and sometimes worsened or caused by blood loss in dialysis circuits or the GI tract); it may be microcytic or normocytic, and may be hypochromic or normochromic.
Renin, a proteolytic enzyme, is stored in the juxtaglomerular cells of the kidneys. Renin secretion is stimulated by reduced blood volume and renal blood flow and is inhibited by sodium and water retention. Plasma renin is assayed by measuring renin activity as the amount of angiotensin I generated per hour. Specimens should be drawn from well-hydrated, sodium- and potassium-replete patients. Plasma renin, aldosterone, cortisol, and adrenocorticotropic hormone (ACTH) should be measured in evaluation of all of the following:
The plasma aldosterone/renin ratio calculated from measurements obtained with the patient in an upright posture is the best screening test for hyperaldosteronism, provided that plasma renin activity is < 0.5 ng/mL/h (< 0.5 mcg/L/h) and aldosterone is > 12 to 15 ng/dL (333 to 416 pmol/L).
Evaluating Kidney Function
Kidney function is evaluated using values calculated from formulas based on results of blood and urine tests.
GFR
Glomerular filtration rate (GFR), the volume of blood filtered through the kidney per minute, is the best overall measure of kidney function; it is expressed in mL/min. Because normal GFR increases with increasing body size, a correction factor using body surface area (BSA) typically is applied. This correction is necessary to compare a patient’s GFR to normal and to define different stages of chronic kidney disease. Given the mean normal BSA of 1.73 m2, the correction factor is 1.73/patient BSA; adjusted GFR results are then expressed as mL/min/1.73 m2.
Normal GFR in young, healthy adults is about 120 to 130 mL/min/1.73 m2 and declines with age to about 75 mL/min/1.73 m2 at age 70. Chronic kidney disease is defined by a GFR < 60 mL/min/1.73 m2 for > 3 months. The standard for GFR measurement is inulin clearance. Inulin is neither absorbed nor secreted by the renal tubule and therefore it is the ideal marker for evaluation of kidney function. However, its measurement is cumbersome and, therefore, is mostly used in research settings. GFR is more accurately estimated by combining CKD-EPI equations based on creatinine and cystatin C than by equations that use creatinine or cystatin C alone (1).
Creatinine clearance
Creatinine is produced at a constant rate by muscle metabolism and is freely filtered by the glomeruli and also is secreted by the renal tubules. Because creatinine is secreted, creatinine clearance (CrCl) overestimates GFR by about 10 to 20% in people with normal kidney function and by up to 50% in patients with advanced renal failure; thus, use of CrCl to estimate GFR in chronic kidney disease is discouraged.
Using a timed (usually 24-hour) urine collection, CrCl can be calculated as


where UCr is urine creatinine in mg/mL, UVol is urine volume in mL/min of collection (1440 minutes for a full 24-hour collection), and PCr is plasma creatinine in mg/mL.
Estimating creatinine clearance
Because serum creatinine by itself is inadequate for evaluation of kidney function, several formulas have been devised to estimate CrCl using serum creatinine and other factors.
The Cockcroft-Gault formula can be used to estimate CrCl. It uses age, lean body weight, and serum creatinine level. It is based on the premise that daily creatinine production is 28 mg/kg/day with a decrease of 0.2 mg/year of age.


The Modification of Diet in Renal Disease (MDRD) study formula (current 4-factor formula) can also be used, although it requires a calculator or computer:


The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula provides a lower sensitivity but a higher specificity for detecting a GFR less than 60 mL/min per 1.73 m2, and may be more useful in evaluating patients with normal or near-normal kidney function. Like the Cockcroft-Gault and MDRD equations, it is also based on the serum creatinine level. Estimating GFR using the 2021 CKD-EPI creatinine equation without race is now recommended (2, 3).


where SCr is serum creatinine in mg/dL, kappa (κ) is 0.7 for females and 0.9 for males, α is -0.241 for females and -0.302 for males, min indicates the minimum of SCr /κ or 1, and max indicates the maximum of SCr /κ or 1.
A calculator is available from the National Kidney Foundation.
Evaluation references
1. Inker LA, Schmid CH, Tighiouart H, et al: Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med 5;367(1):20-29, 2012. doi:10.1056/NEJMoa1114248
2. Delgado C, Bawega M, Burrows NR, et al: Reassessing the inclusion of race in diagnosing kidney diseases: An interim report from the NKF-ASN task force. Am J Kidney Dis 78(1):103-115, 2021. doi: 10.1053/j.ajkd.2021.03.008
3. Delgado C, Bawega M, Crews DC, et al: A unifying approach for CFR estimation: Recommendations of the NKF-ASN Task Force on reassessing the inclusion of race in diagnosis kidney disease. Am J Kidney Dis 79(2):268-288.e1, 2022. doi: 10.1053/j.ajkd.2021.08.003






