


Fibrillary and immunotactoid glomerulopathies are rare conditions defined pathologically by organized deposition of nonamyloid microfibrillar or microtubular structures within the renal mesangium and basement membrane.
Fibrillary and immunotactoid glomerulopathies are thought by some experts to be related disorders. They are found in about 0.6% of renal biopsy specimens, occur equally in men and women, and have been described in patients ≥ 10 years. Average age at diagnosis is about 45. Mechanism is unknown, although deposition of immunoglobulin, particularly IgG kappa and lambda light chains and complement (C3), suggests immune system dysfunction. Patients may have accompanying cancer, paraproteinemia, cryoglobulinemia, plasma cell dyscrasia, hepatitis C infection, or systemic lupus erythematous, or they may have a primary renal disease without evidence of systemic disease. Immunotactoid glomerulonephritis in particular is commonly associated with chronic lymphocytic leukemia and B cell lymphoma.
All patients have proteinuria, > 60% in the nephrotic range. Microscopic hematuria is present in about 60%; hypertension, in about 70%. Slightly > 50% have renal insufficiency at presentation.
(See also Overview of Nephrotic Syndrome.)
Diagnosis of Fibrillary and Immunotactoid Glomerulopathies
Renal biopsy
Diagnosis is suggested by laboratory data and confirmed by renal biopsy. If nephrotic syndrome is present, testing is done as for other cases of nephrotic syndrome.
Urinalysis usually shows features of nephritic syndrome and nephrotic syndrome.
Serum C3 and C4 are usually measured and are occasionally decreased.
Light microscopy of a biopsy specimen shows mesangial expansion by amorphous eosinophilic deposits and mild mesangial hypercellularity. Various other changes may be present on light microscopy (eg, crescent formation, membranoproliferative patterns). Congo red staining is negative for amyloid. Immunostaining reveals IgG and C3 and sometimes kappa and lambda light chains in the area of the deposits.
Electron microscopy shows glomerular deposits consisting of extracellular, elongated, nonbranching microfibrils or microtubules. In fibrillary glomerulonephritis, the diameter of the microfibrils and microtubules varies from 20 to 30 nm. In immunotactoid glomerulonephritis, the diameter of the microfibrils and microtubules varies from 30 to 50 nm. In contrast, in amyloidosis, fibrils are 8 to 12 nm.

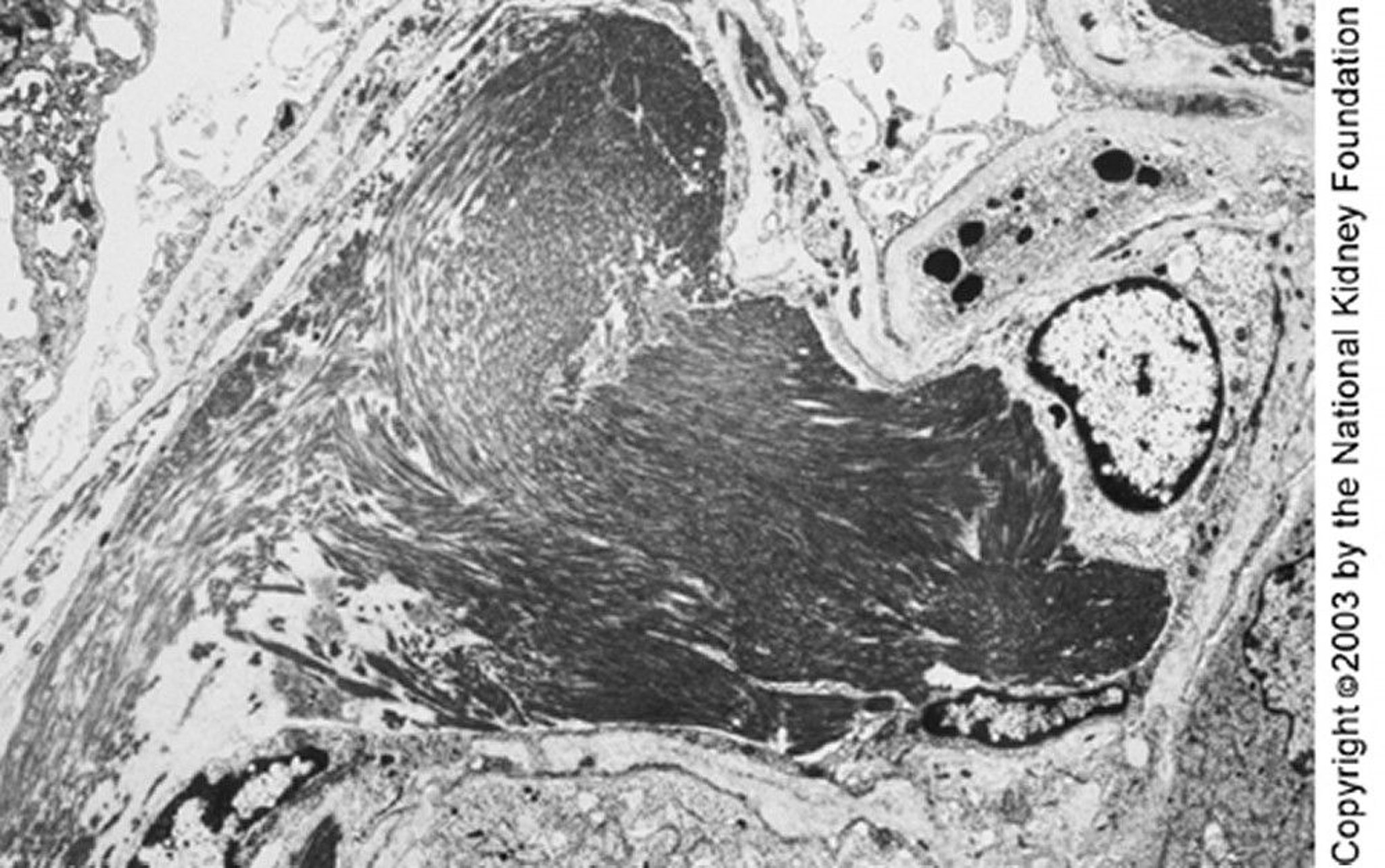
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Some experts distinguish immunotactoid from fibrillary glomerulopathy by the presence of microtubular (as opposed to smaller microfibrillar) structures in the deposits; others distinguish them by the presence of a related systemic illness. For example, a lymphoproliferative disorder, monoclonal gammopathy, cryoglobulinemia, or systemic lupus erythematosus may suggest immunotactoid glomerulonephritis.
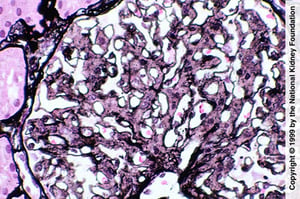
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
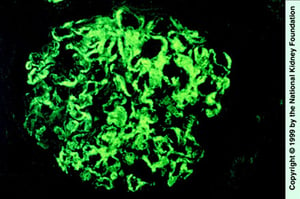
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).

Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).

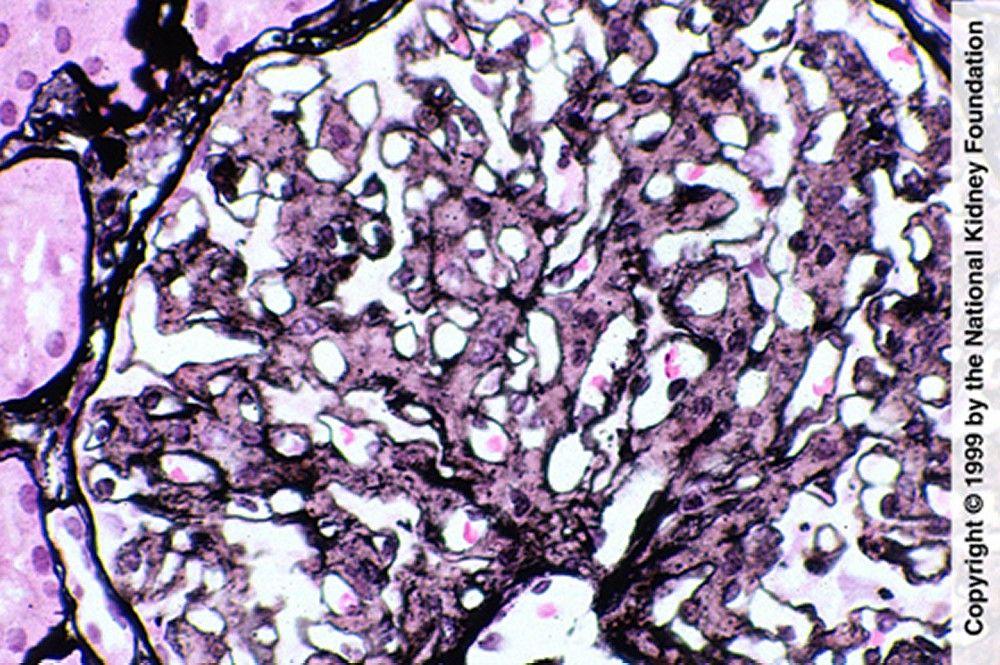
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
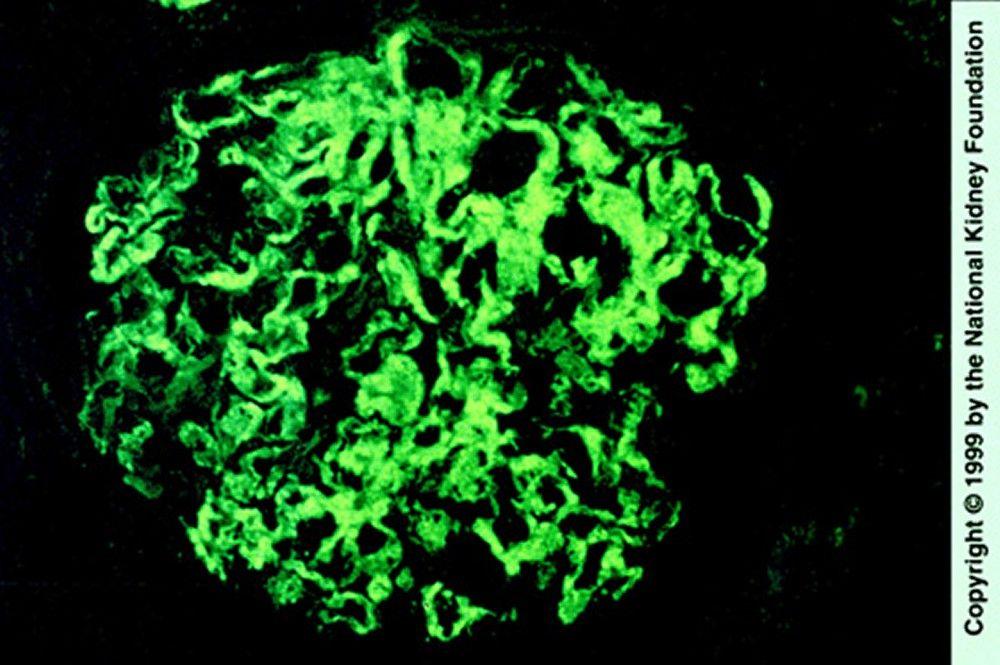
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).

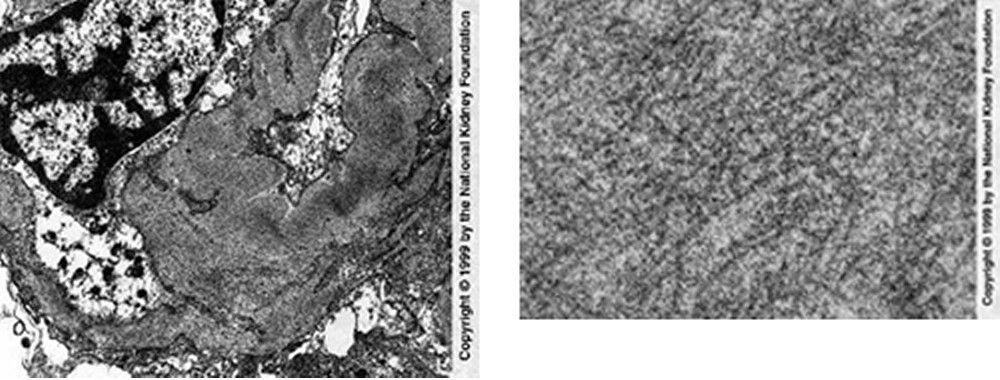
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Treatment of Fibrillary and Immunotactoid Glomerulopathies
Evidence to support specific treatments is lacking although ACE inhibitors and ARBs may be used to reduce proteinuria. Immunosuppressants have been used based on anecdotal evidence but are not a mainstay of therapy; success may be greater with corticosteroids when serum complement is decreased. The disorder may recur after transplantation.
Prognosis for Fibrillary and Immunotactoid Glomerulopathies
The conditions are usually slowly progressive with renal insufficiency, progressing to end-stage kidney disease in 50% of patients within 2 to 4 years. A more rapid decline is predicted by the presence of hypertension, nephrotic-range proteinuria, and renal insufficiency at presentation.






