


Patients with multiple myeloma overproduce monoclonal Ig light chains (Bence Jones proteins); these light chains are filtered by glomeruli, are nephrotoxic, and, in their various forms (free, tubular casts, amyloid), can damage virtually all areas of the kidney parenchyma. Diagnosis is by urine tests (sulfosalicylic acid test or protein electrophoresis) or renal biopsy. Treatment focuses on the multiple myeloma and ensuring adequate urine flow. Myeloma-related kidney disease is rarely caused by Ig heavy chains.
(See also Overview of Tubulointerstitial Diseases.)
Tubulointerstitial disease and glomerular damage are the most common types of renal damage. Glomerular damage is usually the predominant mechanism. The mechanisms by which light chains damage nephrons directly are unknown. Hypercalcemia contributes to renal insufficiency by decreasing renal blood flow.
Tubulointerstitial disease
Types of tubulointerstitial renal disorders in multiple myeloma include
Myeloma kidney (myeloma cast nephropathy)
Acquired Fanconi syndrome (proximal tubular disease)
Interstitial light chain deposition, causing acute tubular necrosis
Light chains saturate the reabsorptive capacity of the proximal tubule, reach the distal nephron, and combine with filtered proteins and Tamm-Horsfall mucoprotein (secreted by cells of the thick ascending limb of Henle) to form obstructive casts. The term myeloma kidney or myeloma cast nephropathy generally refers to renal insufficiency caused by the tubulointerstitial damage that results. Factors that predispose to cast formation include the following:
Low urine flow
Radiocontrast agents
Hyperuricemia
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Increased intratubular calcium due to the hypercalcemia that often occurs secondary to bone lysis in multiple myeloma

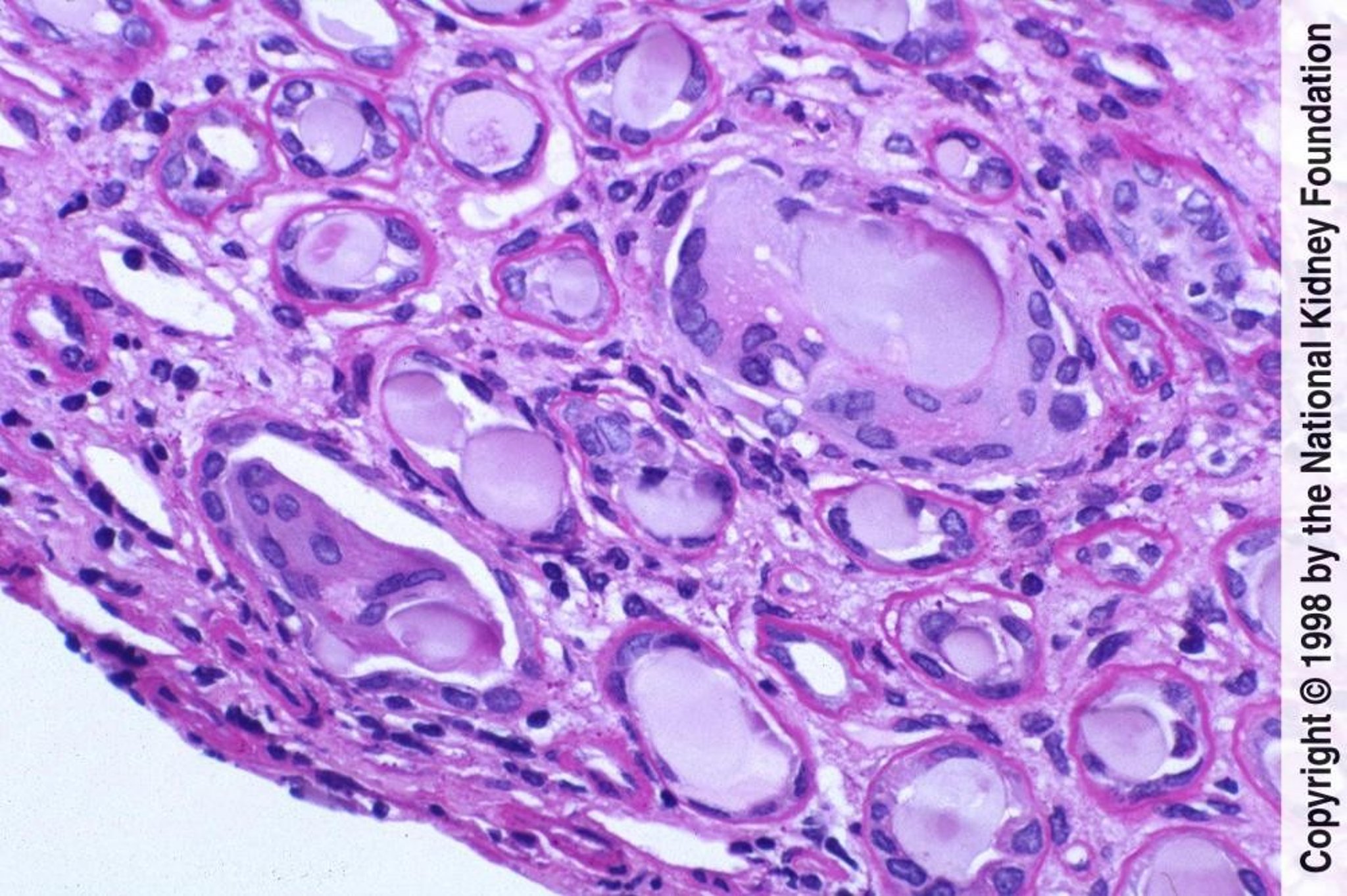
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Other types of tubulointerstitial lesions that occur with Bence Jones proteinuria include proximal tubular transport dysfunction, causing Fanconi syndrome, and light chain interstitial deposition with inflammatory infiltrates and active tubular damage, which can cause acute tubular necrosis.
Glomerulopathies
Types of glomerular renal disorders in multiple myeloma include
Light chain deposition disease
Heavy chain deposition, rarely
AL amyloidosis results in glomerular deposition of AL amyloid in the mesangial, subepithelial, or subendothelial areas or a combination. Amyloid deposition is with randomly oriented, nonbranching fibrils composed of the variable regions of lambda light chains. Light chain deposition disease, which also can occur with lymphoma and macroglobulinemia, is glomerular deposition of nonpolymerized light chains (ie, without fibrils), generally the constant regions of kappa chains.
Rarely, a nonproliferative, noninflammatory glomerulopathy that causes nephrotic-range proteinuria can develop in advanced myeloma-related renal disease. A proliferative glomerulonephritis occasionally develops as an early form of light chain deposition disease with progression to membranoproliferative glomerulonephritis and nodular glomerulopathy reminiscent of diabetic nephropathy; nephrotic-range proteinuria is common.
Symptoms and Signs of Myeloma-Related Kidney Disease
Symptoms and signs are predominantly those of the myeloma (eg, skeletal pain, pathologic fractures, diffuse osteoporosis, bacterial infections, hypercalcemia, normochromic-normocytic anemia out of proportion to the degree of renal failure).
Diagnosis of Myeloma-Related Kidney Disease
Urine protein electrophoresis (myeloma kidney)
Biopsy (glomerulopathy)
Diagnosis of myeloma-related kidney disease is suggested by the following combination of findings:
Renal insufficiency
Bland urine sediment
Negative or trace-positive dipstick for protein (unless urine albumin is elevated in a patient with an accompanying nephrotic syndrome)
Elevated total urinary protein
The diagnosis should be suspected even in patients without a history of or findings suggesting multiple myeloma, particularly if total urinary protein is elevated out of proportion to urinary albumin. Total urinary protein is measured over 24 hours (and is often elevated enough to suggest nephrotic syndrome); urinary albumin is measured by dipstick.
Diagnosis of light chain tubulointerstitial disease (myeloma kidney) is confirmed by urine protein electrophoresis (UPEP).
Diagnosis of glomerulopathy is confirmed by renal biopsy. Renal biopsy may demonstrate light chain deposition in 30 to 50% of patients with myeloma despite the absence of detectable serum or urine paraproteins by immunoelectrophoresis.
Treatment of Myeloma-Related Kidney Disease
Management of multiple myeloma
Prevention of volume depletion and maintenance of a high urine flow rate
Management of multiple myeloma and prevention of volume depletion (eg, using normal saline for volume expansion) to maintain a high urine flow rate are the primary treatments (1). In addition, factors that worsen renal function (eg, hypercalcemia, hyperuricemia, use of nephrotoxic medications) should be avoided or treated.
Several measures are often recommended but are of unproved efficacy. Plasma exchange
Treatment reference
1. Dimopoulos MA, Sonneveld P, Leung N, et al: International Myeloma Working Group Recommendations for the Diagnosis and Management of Myeloma-Related Renal Impairment. J Clin Oncol 34(13):1544-1557, 2016. doi: 10.1200/JCO.2015.65.0044
Prognosis for Myeloma-Related Kidney Disease
Kidney disease is a major predictor of overall prognosis in multiple myeloma. Prognosis is good for patients with tubulointerstitial and glomerular light chain deposition disease who receive treatment. Prognosis is worse for patients with AL amyloidosis, in whom amyloid deposition continues and progresses to renal failure in most cases. In either form without treatment, virtually all renal lesions progress to renal failure.
Key Points
Patients with multiple myeloma can sustain tubulointerstitial and glomerular damage by various mechanisms.
Suspect myeloma-related kidney disease if patients have unexplained renal insufficiency, bland urinary sediment, and/or increased nonalbumin urinary proteins.
Treat myeloma and maintain euvolemia.






