


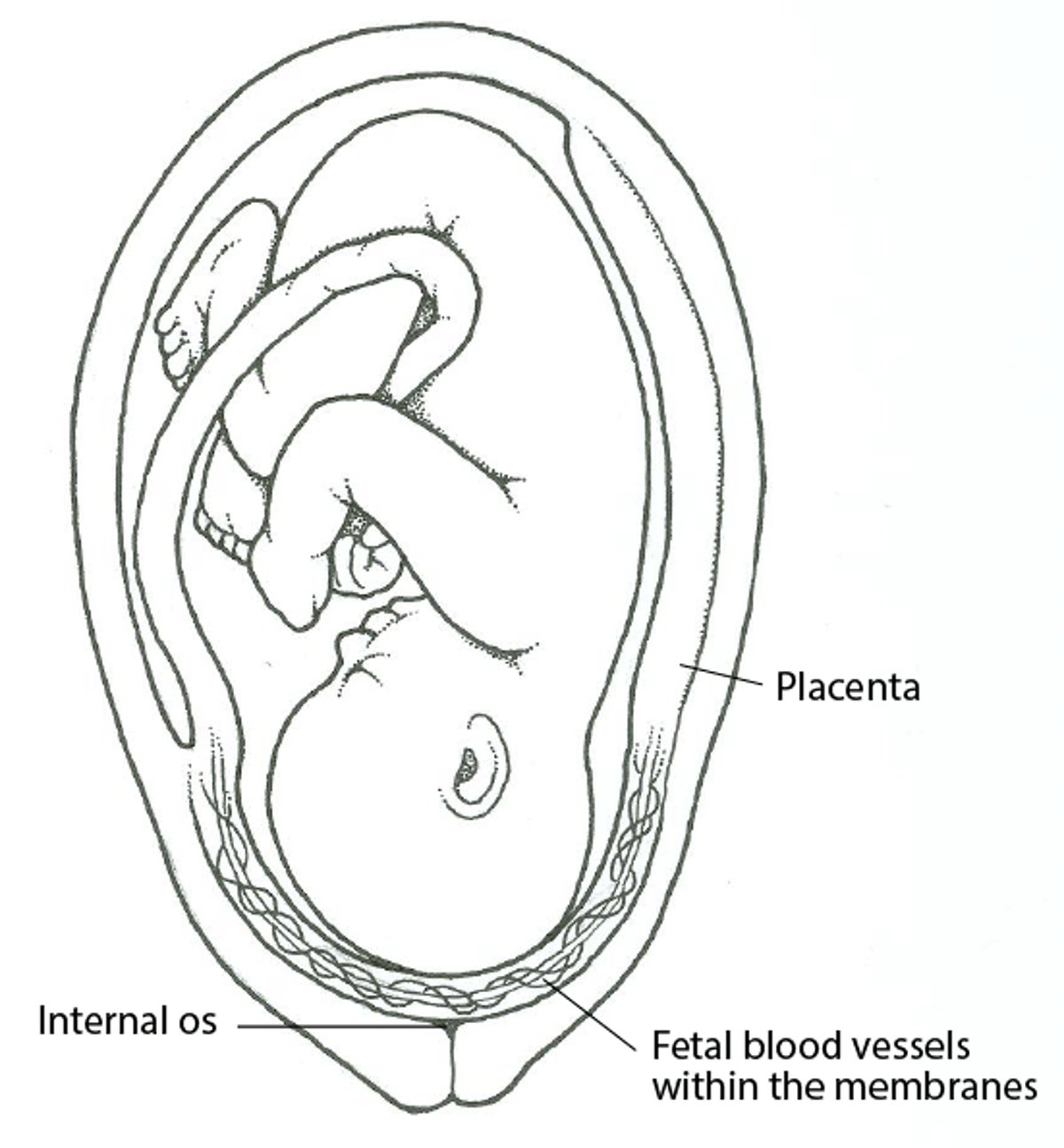
In vasa previa, membranes that contain fetal blood vessels connecting the umbilical cord and placenta overlie or are within 2 cm of the internal cervical os. Diagnosis is by ultrasonography. Management is fetal surveillance and delivery at about 34 weeks, or earlier for bleeding or nonreassuring fetal status. The source of bleeding in vasa previa is fetal, thus blood loss can rapidly impair fetal status.
Vasa previa can occur on its own (see figure Vasa Previa) or with placental abnormalities, such as a velamentous cord insertion. In velamentous cord insertion, vessels from the umbilical cord run through part of the chorionic membrane rather than directly into the placenta. Thus, the blood vessels are not protected by Wharton jelly within the cord, making fetal hemorrhage more likely to occur when the fetal membranes rupture.
Vasa previa is rare, and prevalence is difficult to ascertain; prevalence was 1/1300 deliveries in one large study (1). Fetal mortality rate may approach 60% if vasa previa is not diagnosed before birth.
Vasa Previa

General reference
1. Zhang W, Geris S, Beta J, Ramadan G, Nicolaides KH, Akolekar R: Prevention of stillbirth: impact of two-stage screening for vasa previa. Ultrasound Obstet Gynecol. 2020;55(5):605-612. doi:10.1002/uog.21953
Symptoms and Signs of Vasa Previa
The classic presentation of vasa previa is painless vaginal bleeding, rupture of membranes, and fetal bradycardia.
Diagnosis of Vasa Previa
Transvaginal ultrasonography
Doppler color flow mapping
The diagnosis of vasa previa should be suspected based on presentation or results of routine prenatal ultrasonography (1). The diagnosis is typically confirmed by transvaginal ultrasonography. Fetal vessels can be seen within the membranes passing directly over or near the internal cervical os. Doppler color flow mapping is used.
Vasa previa must be distinguished from funic presentation (prolapse with the umbilical cord between the presenting part and the internal cervical os), in which fetal blood vessels wrapped with Wharton jelly can be seen covering the cervix. In funic presentation, unlike in vasa previa, the umbilical cord moves away from the cervix during ultrasound evaluation; in vasa previa, the cord is fixed in place.
Diagnosis reference
1. Society of Maternal-Fetal (SMFM) Publications Committee, Sinkey RG, Odibo AO, Dashe JS: #37: Diagnosis and management of vasa previa. Am J Obstet Gynecol 213(5):615-619, 2015. doi:10.1016/j.ajog.2015.08.031
Treatment of Vasa Previa
Prenatal monitoring to detect cord compression
Cesarean delivery
Prenatal management of vasa previa is controversial, partly because randomized clinical trials are lacking. At most centers, nonstress testing is done once or twice a week beginning at 28 to 30 weeks. The purpose is to detect compression of the umbilical cord. Admission for fetal and maternal monitoring at about 30 to 34 weeks gestation, or 1 to 2 weeks before scheduled delivery, can be offered. Inpatient fetal monitoring can be continuous or take place every 6 to 8 hours.
Corticosteroids are used to accelerate fetal lung maturity if bleeding occurs or within 7 days of the planned delivery.
Emergency cesarean delivery is usually indicated if any of the following occurs:
Prelabor rupture of the membranes occurs.
Vaginal bleeding continues.
Fetal status is nonreassuring
If none of these problems are present and labor has not occurred, clinicians can offer to schedule cesarean delivery. Cesarean delivery between 34 to 37 weeks has been suggested, but the timing of delivery is controversial; some evidence favors delivery at 34 to 35 weeks (1).
Treatment reference
1. American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice, Society for Maternal-Fetal Medicine: Medically indicated late-preterm and early-term deliveries: ACOG Committee Opinion, Number 831. Obstet Gynecol 138 (1):e35–e39, 2021. doi: 10.1097/AOG.0000000000004447
Key Points
In vasa previa, membranes that contain fetal blood vessels connecting the umbilical cord and placenta overlie or are within 2 cm of the internal cervical os.
Vasa previa may be accompanied by other placental abnormalities, such as velamentous insertion, which increases the risk of fetal hemorrhage when the fetal membranes rupture.
Suspect vasa previa based on symptoms and (painless vaginal bleeding, rupture of membranes, fetal bradycardia) and/or findings during routine prenatal ultrasonography.
Use transvaginal ultrasonography to confirm vasa previa and to distinguish it (fixed umbilical cord) from funic presentation (movable cord).
Check for compression of the cord using nonstress testing, possibly once or twice a week beginning at 28 to 30 weeks.
Schedule cesarean delivery, or if prelabor rupture of the membranes occurs, vaginal bleeding continues, or fetal status is nonreassuring, do emergency cesarean delivery.






