


Amenorrhea (the absence of menstruation) can be primary or secondary.
Primary amenorrhea is failure of menses to occur by age 15 years in patients with normal growth and secondary sexual characteristics. However, absence of menarche and of any breast development by age 13 should prompt evaluation for primary amenorrhea.
Secondary amenorrhea is the absence of menses for 3 months in patients with regular menstrual cycles or for ≥ 6 months in patients with irregular menses (1).
General references
1. Gordon CM, Ackerman KE, Berga SL, et al: Functional hypothalamic amenorrhea: An Endocrine Society clinical practice guideline. Clin Endocrinol Metab 102 (5):1413–1439, 2017. doi: 10.1210/jc.2017-00131
Pathophysiology of Amenorrhea
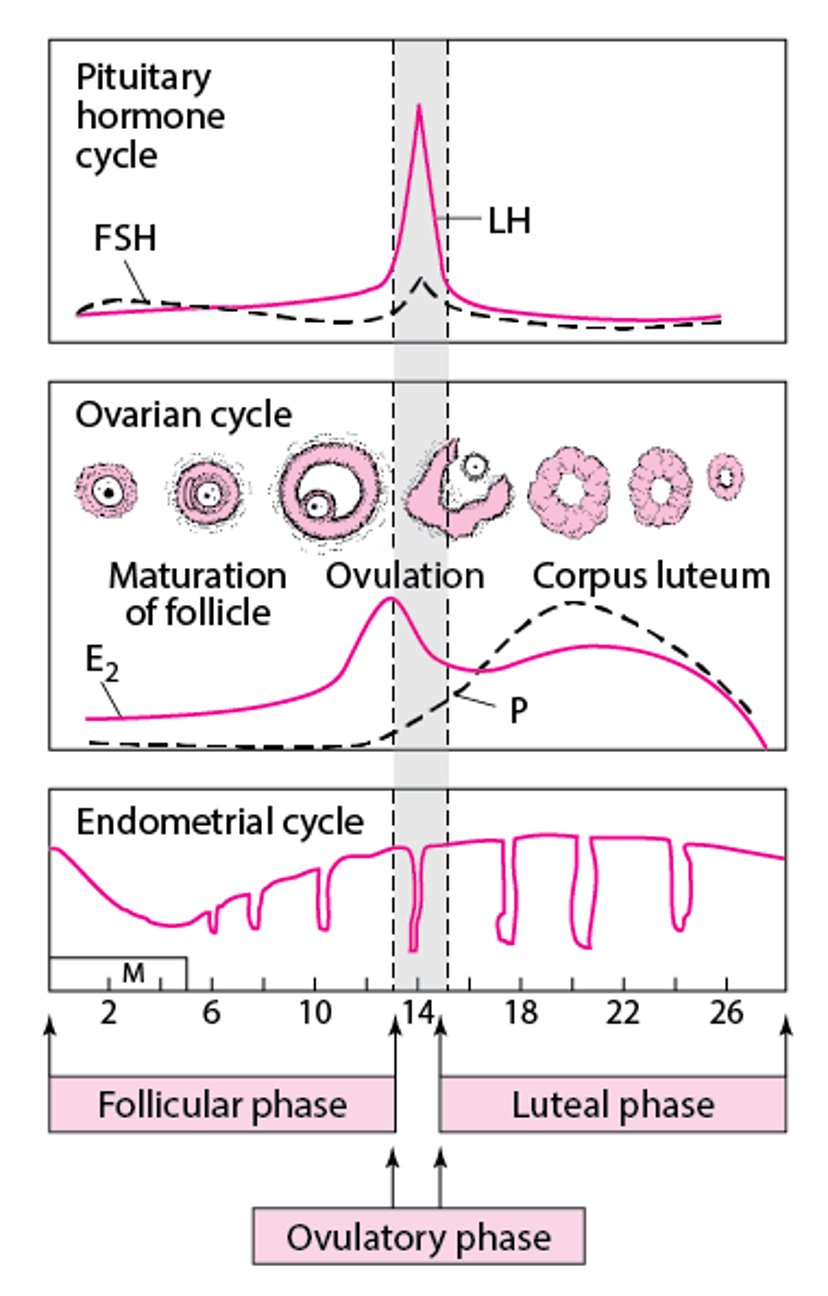
Normally, the hypothalamus generates pulses of gonadotropin-releasing hormone (GnRH). GnRH stimulates the pituitary to produce gonadotropins (follicle-stimulating hormone [FSH] and luteinizing hormone [LH]—see figure Normal Menstrual Cycle), which are released into the bloodstream. Gonadotropins stimulate the ovaries to produce estrogens (mainly estradiol), androgens (mainly testosterone), and progesterone. These hormones do the following:
Follicle-stimulating hormone activates aromatase in ovarian granulosa cells that surround the developing oocytes to convert androgens to estradiol.
Luteinizing hormonesurges during the menstrual cycle; this surge promotes maturation of the dominant oocyte, release of the oocyte, and formation of the corpus luteum (which produces progesterone).
Estrogen stimulates the endometrium, causing it to proliferate.
Progesterone changes the endometrium into a secretory structure and prepares it for egg implantation (endometrial decidualization).
If pregnancy does not occur, estrogen and progesterone production decrease, and the endometrium breaks down and is sloughed during menses. Menstruation occurs 14 days after ovulation in typical cycles.
Normal Menstrual Cycle

When part of this system malfunctions, ovulatory dysfunction occurs; the cycle of gonadotropin-stimulated estrogen production and cyclic endometrial changes is disrupted, resulting in anovulation, and menstrual flow may not occur. Ovulatory dysfunction is the most common cause of amenorrhea, particularly secondary amenorrhea.
However, amenorrhea can occur when ovulation is normal, as occurs when genital anatomic abnormalities (eg, congenital anomalies causing outflow obstruction, intrauterine adhesions [Asherman syndrome]) prevent normal menstrual flow despite normal hormonal stimulation.
Etiology of Amenorrhea
Amenorrhea can be classified based on a number of different criteria, such as
Primary or secondary
Gonadal dysgenesis, anatomic, or endocrinologic
Gonadal dysgenesis and congenital reproductive tract anomalies cause primary amenorrhea.
Secondary amenorrhea may be caused by acquired anatomic reproductive tract abnormalities that interfere with menstrual function or obstruct the menstrual flow.
Primary or secondary amenorrhea may be due to endocrinologic disorders.
Gonadal dysgenesis due to genetic or chromosomal abnormalities (which can cause primary ovarian insufficiency) include
46,XY gonadal dysgenesis
Anatomic causes of amenorrhea include
Congenital female reproductive tract anomalies (eg, vaginal agenesis, imperforate hymen)
Acquired abnormalities (eg, Asherman syndrome or cervical stenosis)
Common endocrinologic causes include
Constitutional delay of puberty
Pregnancy (the most common cause in women of reproductive age)
Hyperprolactinemia (eg, due to pituitary adenoma, lactational amenorrhea during breastfeeding, or use of antipsychotics)
Functional hypothalamic amenorrhea (eg, due to excessive exercise, eating disorders, or stress [1])
Primary ovarian insufficiency (premature ovarian failure)
Progestin-only contraceptives often cause amenorrhea. Combined estrogen/progestin contraceptives can cause amenorrhea if they are used continuously (without placebo pills or no medication every few weeks) or for a long time (if the endometrium becomes atrophic).
Other endocrinologic causes are receptor or enzyme disorders (eg, complete androgen insensitivity syndrome, 5-alpha-reductase deficiency).
Amenorrhea due to ovulatory dysfunction
Amenorrhea due to ovulatory dysfunction is usually secondary but may be primary if ovulation never begins—eg, because of a genetic disorder. If ovulation never begins, delayed puberty usually results, and development of secondary sexual characteristics is abnormal. Genetic disorders that confer a Y chromosome increase the risk of ovarian germ cell cancer.
The most common causes of ovulatory dysfunction involve a disruption of the hypothalamic-pituitary-ovarian axis. Thus, causes include
Hypothalamic dysfunction (particularly functional hypothalamic amenorrhea)
Pituitary dysfunction
Primary ovarian insufficiency (premature ovarian failure)
Endocrine disorders that cause androgen excess (particularly polycystic ovary syndrome)
Hypothalamic dysfunction may result in decreased GnRH production, which in turn may cause decreased gonadotropin production. A common cause is insufficient energy intake due to dietary restriction or strenuous exercise. Women with amenorrhea due to hypothalamic dysfunction have lower levels of serum leptin (an anorectic hormone produced by fat cells); lower levels may contribute to decreased gonadotropin production (2).
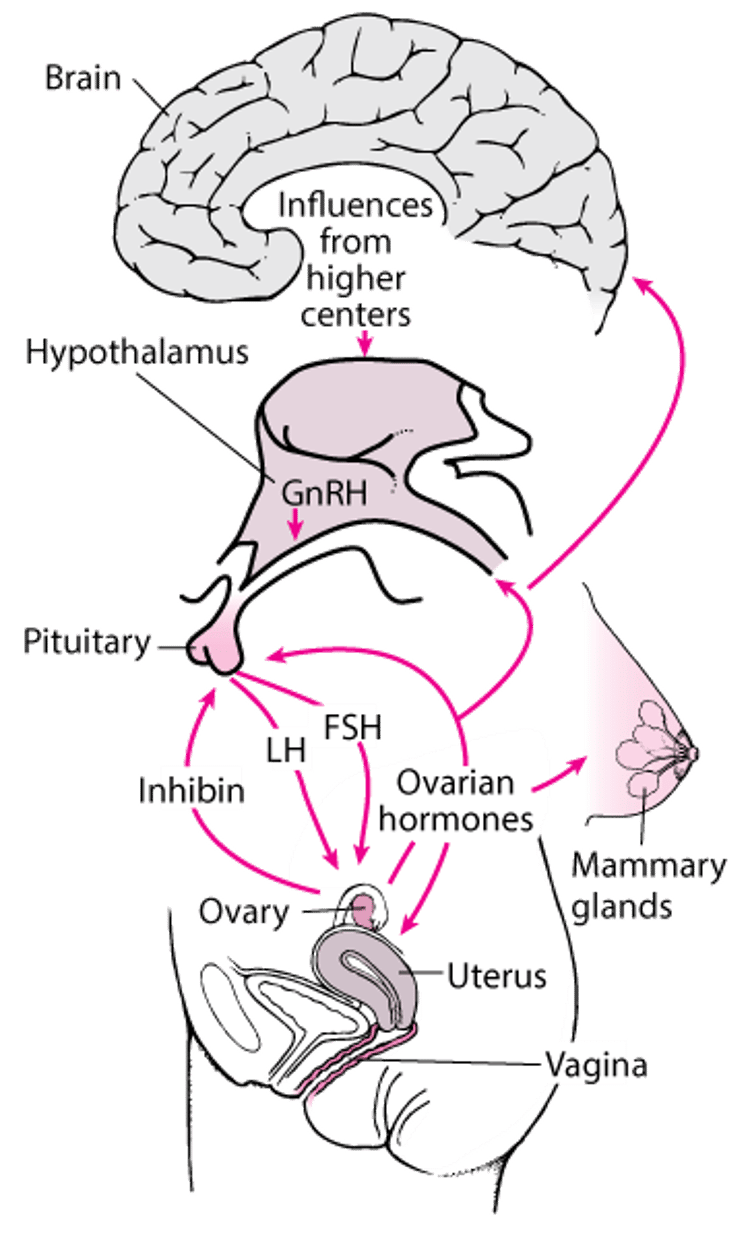
The central nervous system-hypothalamic-pituitary-gonadal target organ axis
Ovarian hormones have direct and indirect effects on other tissues (eg, bone, skin, muscle). FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; LH = luteinizing hormone. |

Amenorrhea due to reproductive tract abnormalities
Amenorrhea may also occur if patients have abnormalities that affect menstrual function or obstruct menstrual flow. Many patients with these conditions have normal reproductive endocrine function and may have ovulatory menstrual cycles.
The most common causes of amenorrhea due to reproductive tract abnormalities include
Congenital anatomic genital abnormalities that obstruct menstrual flow
Acquired abnormalities of female reproductive tract (eg, Asherman syndrome, cervical stenosis)
Obstructive abnormalities cause primary amenorrhea and are usually accompanied by normal hormonal function. Such obstruction may result in
Hematocolpos (accumulation of menstrual blood in the vagina), which can cause the vagina to bulge
Hematometra (accumulation of blood in the uterus), which can cause uterine distention that may be noted as a pelvic mass or bulging of the cervix
Because ovarian function is normal, external genital organs and other secondary sexual characteristics develop normally. Some congenital disorders (eg, those accompanied by vaginal aplasia or a vaginal septum) also cause urinary tract and skeletal abnormalities.
Some acquired anatomic abnormalities, such as endometrial scarring after uterine instrumentation (Asherman syndrome), cause secondary ovulatory amenorrhea.
Etiology references
1. Gordon CM, Ackerman KE, Berga SL, et al: Functional hypothalamic amenorrhea: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 102 (5):1413–1439, 2017. doi: 10.1210/jc.2017-00131
2. Bouzoni E, Perakakis N, Mantzoros CS: Circulating profile of activin-follistatin-inhibin axis in women with hypothalamic amenorrhea in response to leptin treatment. Metabolism 113:154392, 2020. doi: 10.1016/j.metabol.2020.154392 Epub 2020 Oct 10.
Evaluation of Amenorrhea
Girls are evaluated for primary amenorrhea if menarche has not occurred and they reach one of the following milestones:
Age 13 and they have no signs of puberty (eg, breast development, growth spurt)
Three years after thelarche (onset of breast development)
Age 15 (in patients with normal growth and development of secondary sexual characteristics)
Girls and women of reproductive age should be evaluated for secondary amenorrhea if they have previously been menstruating and have
Missed menstrual cycles for ≥ 3 months if they previously had regular menstrual cycles or ≥ 6 months if they previously had irregular menstrual cycles (1)
< 9 menses a year or cycle length > 38 days (oligomenorrhea)
A new and persistent change in menstrual pattern (frequency, volume, duration)
History
History of present illness includes questions about menstrual function (see table Normal Menstrual Parameters [2]):
Date of first day of last menstrual period
Cycle frequency
Cycle regularity in the past 3 to 12 months and whether periods have ever been regular
Duration of bleeding
Volume of bleeding
Questions about associated symptoms or factors include
Are menses accompanied by significant discomfort? (Rarely, discomfort indicates structural abnormalities.)
Does the patient have cyclic breast tenderness and mood changes (moliminal symptoms), which, if absent, may indicate abnormal uterine bleeding, not cyclic menses?
What are the patient's dietary and exercise habits?
For adolescents and some young patients, questions about pubertal development should be included:
Has menarche occurred (to distinguish primary from secondary amenorrhea) and, if so, what was the age at menarche?
At what ages did growth and development milestones occur?
Have the changes of puberty occurred (eg, breast development, growth spurt, presence of axillary and pubic hair)?
Review of systems should cover symptoms suggesting possible causes, including the following:
Galactorrhea, headaches, hearing loss, and visual field defects: Pituitary disorders
Fatigue, weight gain, and cold intolerance: Hypothyroidism
Palpitations, nervousness, tremor, and heat intolerance: Hyperthyroidism
Palpitations: Anorexia nervosa with electrolyte abnormalities (eg, hypokalemia, hypomagnesemia)
Acne, hirsutism, and deepening of the voice: Androgen excess
For patients with secondary amenorrhea, hot flushes, vaginal dryness, sleep disturbance, fragility fractures, and decreased libido: Ovarian insufficiency
Past medical history should note risk factors for the following:
Functional hypothalamic amenorrhea, such as stress; chronic illness; new medications; a recent change in weight, diet, or exercise intensity; and a history or current symptoms of eating disorders
Endometrial scarring (Asherman syndrome), as may occur in patients with a history of dilation and curettage (particularly if they also had a uterine infection), endometrial ablation, endometritis, obstetric injury, uterine surgery
Medication history should include specific questions about current or past medications, such as the following:
Medications that affect dopamine (eg, antihypertensives, antipsychotics, opioids, tricyclic antidepressants, antiseizure drugs)
Hormones that can cause virilization (eg, androgens, high-dose androgenic progestins, over-the-counter [OTC] anabolic steroids)
Hormonal contraceptives
Systemic corticosteroids
OTC products and supplements, some of which contain bovine hormones
Substance abuse, including opioid abuse, which may affect the secretion of pituitary hormones and lead to oligomenorrhea or amenorrhea
Family history should include any cases of delayed puberty or genetic disorders, including Fragile X syndrome.
Physical examination
Clinicians should note vital signs and calculate body mass index (BMI).
If pubertal development may be abnormal, secondary sexual characteristics are evaluated; breast and pubic hair development are staged using the Tanner method (see Sexual Maturation). If axillary and pubic hair is present, adrenarche has occurred.
A breast examination should be done to check for galactorrhea (breast milk secretion not temporally associated with childbirth); it can be distinguished from other types of nipple discharge by finding fat globules in the fluid using a low-power microscope.
Pelvic examination is done to check for enlargement of the uterus (possibly due to pregnancy or a tumor), ovaries, and clitoris (clitoromegaly). Pelvic examination findings also help determine whether estrogen has been deficient. In women of reproductive age, the presence of cervical mucus with spinnbarkeit (a stringy, stretchy quality) usually indicates adequate estrogen; thin, pale vaginal mucosa without rugae and pH > 6.0 indicates estrogen deficiency. In girls or some young women, examination may detect anatomic genital abnormalities (eg, imperforate hymen, vaginal septum, vaginal, cervical, or uterine aplasia). A bulging hymen may be caused by hematocolpos, which suggests genital outflow obstruction.
General examination focuses on evidence of virilization, including hirsutism, temporal balding, acne, voice deepening, increased muscle mass, and defeminization (a decrease in previously normal secondary sexual characteristics, such as decreased breast size and vaginal atrophy). Virilization results from increased androgen production by the adrenal glands or ovaries. Hypertrichosis (excessive growth of hair on the extremities, head, and back), which is common in some families, is differentiated from true hirsutism, which is characterized by excess hair on the upper lip and chin and between the breasts.
Finding black patches on the skin due to acanthosis nigricans is a possible sign of polycystic ovary syndrome (PCOS) or diabetes.
Clinicians should check for hypothermia, bradycardia, hypotension, and reduced subcutaneous fat, which suggest anorexia nervosa, and for dental erosion, palatal lesions, reduced gag reflex, subconjunctival hemorrhage, and subtle hand changes with calluses on the dorsum of the hand (due to frequent vomiting), which suggest bulimia.
Red flags
The following findings are of particular concern in patients with amenorrhea:
Delayed puberty
Virilization
Visual field defects
Impaired sense of smell (anosmia)
A spontaneous milky nipple discharge
A significant increase or decrease in weight
Pearls & Pitfalls
|
Interpretation of findings
History and physical examination findings may suggest an etiology of amenorrhea, even before laboratory testing (see table Findings Suggesting Possible Causes of Amenorrhea).
In primary amenorrhea, the presence of normal secondary sexual characteristics usually reflects normal hormonal function; amenorrhea is usually ovulatory and typically due to a congenital anatomic genital tract obstruction. Primary amenorrhea accompanied by abnormal secondary sexual characteristics is usually caused by ovulatory dysfunction (eg, due to a genetic disorder).
In secondary amenorrhea, clinical findings sometimes suggest a mechanism:
Galactorrhea suggests hyperprolactinemia (eg, pituitary dysfunction, use of certain drugs); if visual field defects and headaches are also present, pituitary tumors should be considered.
Symptoms and signs of estrogen deficiency (eg, hot flushes, night sweats, vaginal dryness or atrophy) suggest primary ovarian insufficiency (premature ovarian failure) or functional hypothalamic amenorrhea (eg, due to excessive exercise, a low body weight, or low body fat)
Virilization and clitoral enlargement suggest androgen excess (eg, polycystic ovary syndrome, androgen-secreting tumor, Cushing syndrome, use of certain drugs). If patients have a high BMI, acanthosis nigricans, or both, polycystic ovary syndrome is likely.
Testing
History and physical examination help direct testing.
The approach to primary amenorrhea (see algorithm Evaluation of primary amenorrhea) differs from that to secondary amenorrhea (see algorithm Evaluation of secondary amenorrhea), although no specific general approaches or algorithms are universally accepted.
If patients have primary amenorrhea and normal secondary sexual characteristics, testing should begin with pelvic ultrasonography to check for congenital anatomic genital tract obstruction. MRI may be needed if abnormalities are identified.
A pregnancy test is required
Evaluation of primary amenorrhea [a]
[a] Normal values are
Although these values are representative, normal ranges may vary between laboratories. Prolactin 50–100 ng/mL is considered mildly elevated and is usually due to use of a medication. Prolactin > 100 ng/mL is considered elevated and is more likely to be due to a tumor. |
[b] Some clinicians measure LH levels when they measure FSH levels or when FSH levels are equivocal. |
[c] If patients have primary amenorrhea and normal secondary sexual characteristics, testing should begin with pelvic examination and ultrasonography to check for congenital anatomic genital tract obstruction. |
[d] Constitutional delay of growth and puberty is possible. |
[e] Possible diagnoses include functional hypothalamic chronic anovulation and genetic disorders (eg, congenital gonadotropin-releasing hormone deficiency, Prader-Willi syndrome). |
[f] Possible diagnoses include Cushing syndrome, exogenous androgens, congenital adrenal virilism, and polycystic ovary syndrome. |
[g] Possible diagnoses include Turner syndrome and disorders characterized by Y chromosome material. |
[h] Pubic hair may be sparse. |
DHEAS = dehydroepiandrosterone sulfate; FSH = follicle-stimulating hormone; LH = luteinizing hormone. |

![Evaluation of primary amenorrhea [a]](https://edge.sitecorecloud.io/mmanual-ssq1ci05/media/professional/images/g/y/n/gyn_primary_amenorrhea_algorithm_no_fnts_change.gif?thn=0&sc_lang=en&mw=1920)
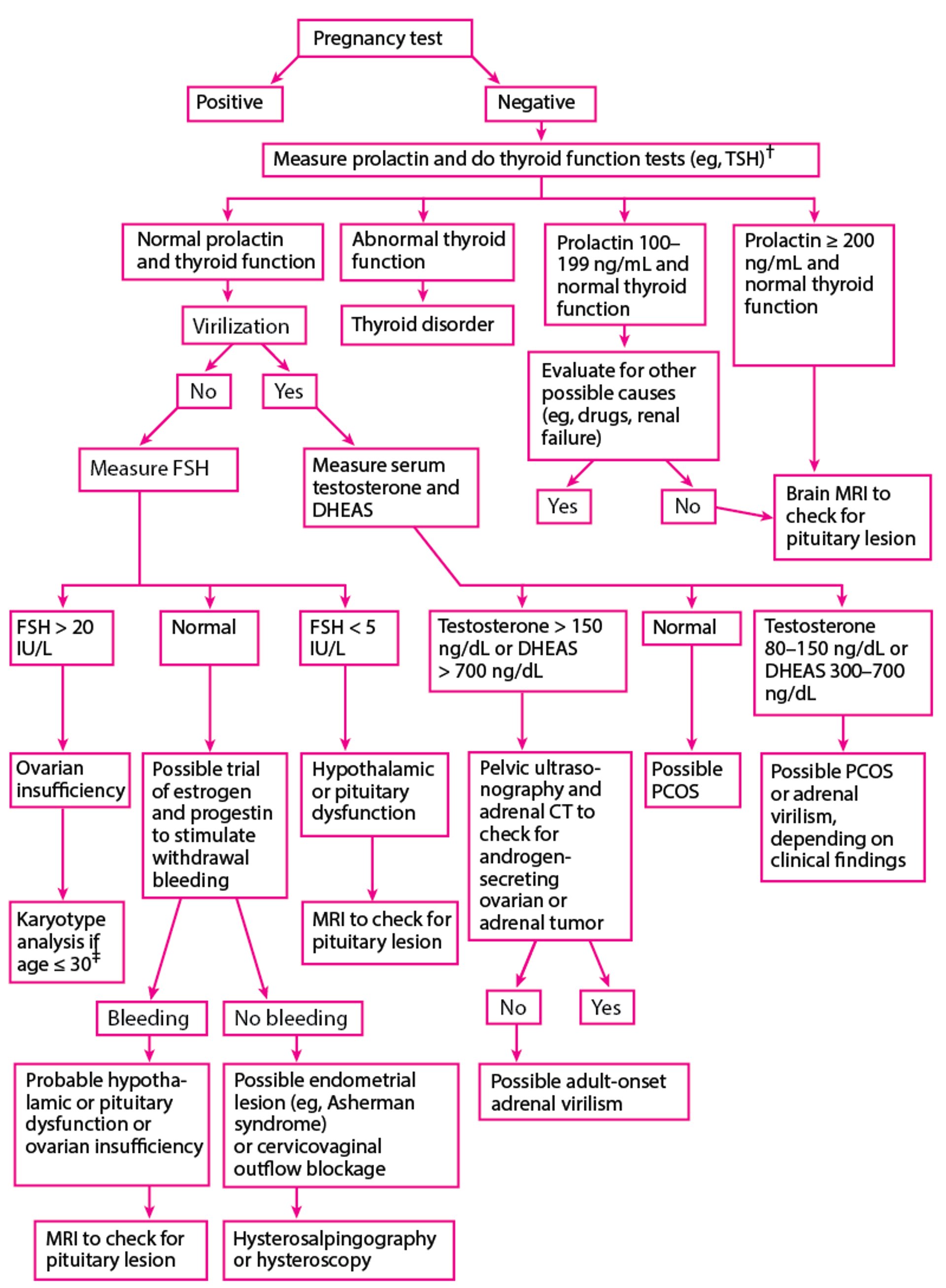
Evaluation of secondary amenorrhea*
* Normal values are
Although these values are representative, normal ranges may vary between laboratories. Prolactin 50–100 ng/mL is considered mildly elevated and is usually due to a drug adverse effect. Prolactin > 100 ng/mL is considered elevated and is more likely to be due to a tumor. |
† Some clinicians simultaneously measure FSH and LH levels. |
‡ Clinicians should check for the presence of Y chromosome and Fragile X syndrome (premutation for the FMR1 gene). |
DHEAS = dehydroepiandrosterone sulfate; FSH = follicle-stimulating hormone; LH = luteinizing hormone; PCOS = polycystic ovary syndrome; TSH = thyroid-stimulating hormone. |

Additional blood tests that are commonly done (to exclude specific etiologies) include
Follicle-stimulating hormone (ovarian insufficiency); if the level is high, it should be remeasured monthly at least twice
Thyroid stimulating hormone (thyroid disease)
Prolactin (if the level is high [hyperprolactinemia], it should be remeasured)
Total serum testosterone or dehydroepiandrosterone sulfate (PCOS or other causes of hirsutism or virilization)
Amenorrhea with high follicle-stimulating hormone (FSH) levels (hypergonadotropic hypogonadism) suggests ovarian dysfunction. Amenorrhea with low FSH levels (hypogonadotropic hypogonadism) suggests hypothalamic or pituitary dysfunction.
Mildly elevated levels of testosterone or DHEAS suggest PCOS, but levels can be elevated in women with hypothalamic or pituitary dysfunction and are sometimes normal in hirsute women with PCOS. The cause of elevated levels can sometimes be determined by measuring serum luteinizing hormone (LH). In polycystic ovary syndrome, circulating LH levels are often increased, increasing the ratio of LH to FSH.
If symptoms or signs suggest an underlying disorder, specific tests may be indicated. For example, patients with abdominal striae, moon facies, a buffalo hump, truncal obesity, and thin extremities should be tested for Cushing syndrome. Patients with headaches and visual field defects or evidence of pituitary dysfunction require brain MRI. If clinical evaluation suggests a chronic disease, liver and kidney function tests are done, and erythrocyte sedimentation rate (ESR) is determined.
Progestin challenge test
If patients have secondary amenorrhea with normal prolactin and FSH levels and normal thyroid function and do not have virilization, a trial of a progestin can be given to try to evaluate estrogen status. If the estrogen level is sufficient, a course of a progestin should stimulate withdrawal bleeding after the progestin is stopped (progestin challenge test; also called progestin withdrawal test).
If bleeding occurs within a few days, the estrogen level is sufficient and amenorrhea is probably caused by hypothalamic-pituitary dysfunction, ovarian insufficiency, or estrogen excess.
If bleeding does not occur, an estrogen/progestin challenge test is done.
Estrogen/progestin challenge test
The estrogen
However, bleeding may not occur in patients who do not have these abnormalities because the uterus is insensitive to estrogen due to prolonged use of estrogen/progestin contraceptives or rare endocrine disorders (estrogen insensitivity syndrome, estrogen resistance). Thus, the trial using estrogen and progestin may be repeated for confirmation.
Because this trial takes weeks and results can be inaccurate, diagnosis of some serious disorders may be delayed significantly; thus, brain MRI should be considered before or during the trial if a pituitary or other brain lesion is suspected.
Evaluation references
1. Rebar R: Evaluation of amenorrhea, anovulation, and abnormal bleeding [updated, 2018]. In Endotext [Internet], edited by KR Feingold, B Anawalt, A Boyce, et al. South Dartmouth (MA), MDText.com Inc, 2000.
2. Munro MG, Critchley HOD, Fraser IS for the FIGO (International Federation of Gynecology and Obstetrics) Menstrual Disorders Committee): The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynaecol Obstet 143 (3):393–408, 2018. doi: 10.1002/ijgo.12666 Epub 2018 Oct 10.
Treatment of Amenorrhea
Treatment is directed at the underlying disorder; with such treatment, menses sometimes resume. Some abnormalities obstructing the genital outflow tract can be surgically repaired. If a Y chromosome is present, bilateral oophorectomy is recommended because risk of ovarian germ cell cancer is increased.
Common problems associated with amenorrhea may also require treatment, including
For infertility if pregnancy is desired, inducing ovulation
Treating symptoms and long-term effects of estrogen deficiency (eg, osteoporosis, cardiovascular disorders, vaginal atrophy)
Treating symptoms and managing long-term effects of estrogen excess (eg, prolonged bleeding, persistent or marked breast tenderness, risk of endometrial hyperplasia and cancer)
Minimizing hirsutism and long-term effects of androgen excess (eg, cardiovascular disorders, hypertension)
Key Points
Primary amenorrhea in patients without normal secondary sexual characteristics is usually caused by ovulatory dysfunction (eg, due to a genetic disorder).
Always exclude pregnancy by urine or blood tests rather than by history.
Primary amenorrhea is evaluated differently from secondary amenorrhea.
If patients have primary amenorrhea and normal secondary sexual characteristics, begin testing with pelvic ultrasonography to check for congenital anatomic genital tract obstruction.
If patients have signs of virilization, check for conditions that cause androgen excess (eg, polycystic ovary syndrome, an androgen-secreting tumor, Cushing syndrome, use of certain medications).
If patients have symptoms and signs of estrogen deficiency (eg, hot flushes, night sweats, vaginal dryness or atrophy), check for primary ovarian insufficiency and conditions that cause functional hypothalamic amenorrhea.
If patients have galactorrhea, check for conditions that cause hyperprolactinemia (eg, pituitary dysfunction, use of certain medications).






