


Anemia is a decrease in the number of red blood cells (RBCs) as measured by the red cell count, the hematocrit, or the red cell hemoglobin content.
In men, anemia is defined as any of the following:
Hemoglobin < 14 g/dL (140 g/L)
Hematocrit < 42% (< 0.42)
RBC < 4.5 million/mcL (< 4.5 × 1012/L)
In women, anemia is defined as any of the following:
Hemoglobin < 12 g/dL (120 g/L)
Hematocrit < 37% (< 0.37)
RBC < 4 million/mcL (< 4 × 10 12/L)
For infants and children, normal values vary with age, necessitating use of age-related tables (see table Age-Specific Values for Hemoglobin and Hematocrit).
Anemia is not a diagnosis; it is a manifestation of an underlying disorder (see Etiology of Anemia). Thus, even mild, asymptomatic anemia should be investigated so that the primary problem can be diagnosed and treated.
Anemia is usually suspected based on the history and physical examination. Common symptoms and signs of anemia include
General fatigue
Weakness
Dyspnea on exertion
Pallor
History and physical examination are followed by laboratory testing with a complete blood count, reticulocyte count, and peripheral smear. The differential diagnosis (and cause of anemia) can then be further refined based on the results of testing.
Pearls & Pitfalls
|
Patient History in Anemia
The history should address
Risk factors for particular anemias
Symptoms of anemia itself
Symptoms that reflect the underlying disorder
Risk factors for anemia
Anemia has many risk factors. For example, a vegan diet predisposes to vitamin B12 deficiency anemia, whereas alcohol use disorder increases the risk of folate deficiency anemia. A number of hemoglobinopathies are inherited, and certain drugs and infections predispose to hemolysis. Cancer, rheumatic disorders, and chronic inflammatory disorders can suppress red cell production. Autoimmune disorders such as systemic lupus erythematosus or lymphoma can predispose to autoimmune hemolytic anemia.
Symptoms of anemia
The symptoms of anemia are neither sensitive nor specific and do not help differentiate between types of anemias. Symptoms reflect compensatory responses to tissue hypoxia and usually develop when the hemoglobin level falls well below the patient's individual baseline. Symptoms are generally more pronounced in patients with limited cardiopulmonary reserve or when the anemia develops very rapidly.
Symptoms such as weakness, fatigue, drowsiness, angina, syncope, and dyspnea on exertion can indicate anemia. Vertigo, headache, pulsatile tinnitus, amenorrhea, loss of libido, and gastrointestinal (GI) complaints may also occur.
Heart failure or shock can develop in patients with severe tissue hypoxia or hypovolemia.
Symptoms that suggest cause of anemia
Certain symptoms may suggest the cause of the anemia. For example, melena, epistaxis, hematochezia, hematemesis, or menorrhagia indicates bleeding. Jaundice and dark urine, in the absence of liver disease, suggest hemolysis. Weight loss may suggest cancer. Diffuse severe bone or chest pain may suggest sickle cell disease, and stocking-glove paresthesias may suggest vitamin B12 deficiency.
Physical Examination in Anemia
A complete physical examination is necessary. Signs of anemia itself are neither sensitive nor specific; however, pallor is common with severe anemia.
Signs of underlying disorders are more diagnostically accurate than are signs of anemia. Heme-positive stool identifies gastrointestinal bleeding. Hemorrhagic shock (eg, hypotension, tachycardia, pallor, tachypnea, diaphoresis, confusion) may result from acute bleeding. Jaundice may suggest hemolysis. Splenomegaly may occur with hemolysis, a hemoglobinopathy, connective tissue diseases, myeloproliferative disorders, infection, or cancer. Peripheral neuropathy suggests vitamin B12 deficiency. Fever and heart murmurs suggest infective endocarditis. Rarely, high-output heart failure develops as a compensatory response to anemia-induced tissue hypoxia.
Testing in Anemia
CBC with white blood cells (WBC) and platelet counts
RBC indices and morphology
Reticulocyte count
Peripheral smear
Sometimes bone marrow aspiration and biopsy
Laboratory evaluation begins with a complete blood count (CBC), including white blood cell (WBC) and platelet counts, RBC indices and morphology (mean corpuscular volume [MCV], mean corpuscular hemoglobin [MCH], mean corpuscular hemoglobin concentration [MCHC], red blood cell distribution width [RDW]), and examination of the peripheral smear. The reticulocyte count demonstrates how well the bone marrow is compensating for the anemia. Subsequent tests are selected on the basis of these results and on the clinical presentation. Recognition of general diagnostic patterns can expedite the diagnosis (see table Characteristics of Common Anemias).
Complete blood count and RBC indices
The automated CBC directly measures hemoglobin, RBC count, WBC count, and platelet count, plus mean corpuscular volume (MCV), which is a measure of RBC volume. Hematocrit, which is a measure of the percentage of blood made up of RBCs, mean corpuscular hemoglobin (MCH), which is a measure of the hemoglobin content in individual RBCs but is of no clinical significance, and mean corpuscular hemoglobin concentration (MCHC), which is a measure of the hemoglobin concentration in individual RBCs are calculated values.
The diagnostic criterion for anemia is
For men: Hemoglobin < 14 g/dL (140 g/L), hematocrit < 42% (< 0.42), or RBC < 4.5 million/mcL (< 4.5 × 10 12/L)
For women: Hemoglobin < 12 g/dL (120 g/l), hematocrit < 37% (< 0.37), or RBC < 4 million/mcL (< 4 × 10 12/L)
For infants and children, normal values vary with age, necessitating use of age-related tables (see table Age-Specific Values for Hemoglobin and Hematocrit).
RBC populations are termed microcytic (small cells) if MCV is < 80 fL, and macrocytic (large cells) if MCV is > 100 fL. However, because reticulocytes are also larger than mature red cells, large numbers of reticulocytes can elevate the MCV.
Automated techniques can also determine the degree of variation in RBC size, expressed as the RBC volume distribution width (RDW). A high RDW may be the only indication of simultaneous microcytic and macrocytic disorders; such a pattern may result in a normal MCV, which measures only the mean value. The term hypochromia refers to RBC populations in which the MCHC is < 30%. RBC populations with a normal MCHC value are normochromic. Spherocytes can have an elevated MCHC. Red cells defend their MCHC over their MCV (preserving hemoglobin at the expense of RBC size), which is why microcytosis occurs with iron deficiency and with impaired hemoglobin synthesis.
The RBC indices can help indicate the mechanism of anemia and narrow the number of possible causes.
Microcytic indices occur with altered heme or globin synthesis. The most common causes are iron deficiency, thalassemia, and related hemoglobin-synthesis defects. In some patients with the anemia of chronic disease, the MCV is microcytic or borderline microcytic.
Normocytic indices occur in anemias resulting from deficient erythropoietin (EPO) production or inadequate response to it (hypoproliferative anemias). Hemorrhage, before iron deficiency develops, usually results in normocytic and normochromic anemia unless the number of reticulocytes is excessive.
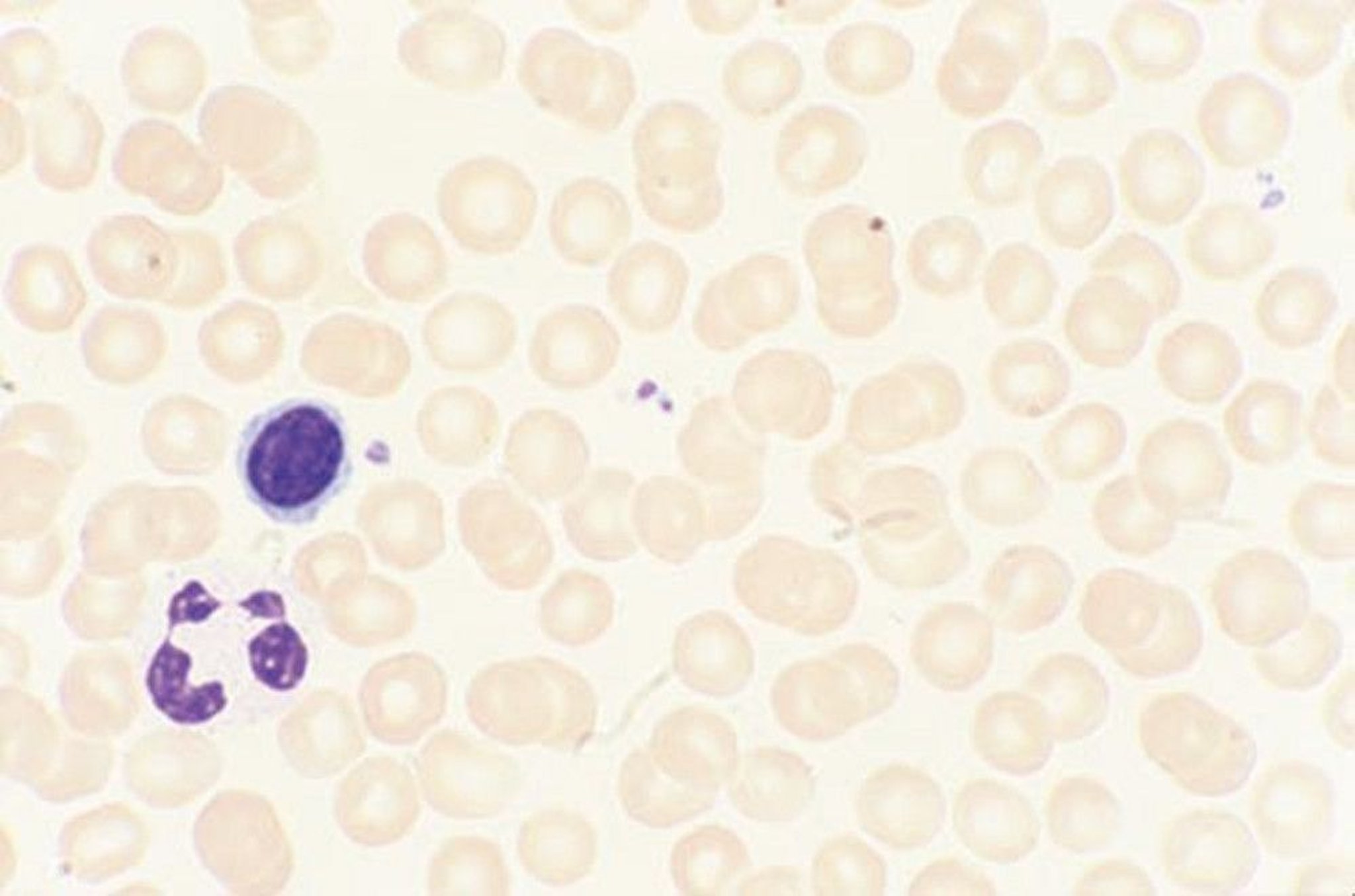
Peripheral smear
The peripheral smear is highly sensitive to excessive RBC production and hemolysis. It is more accurate than automated technologies for recognition of altered RBC structure, thrombocytopenia, nucleated RBCs, or immature granulocytes and can detect other abnormalities (eg, malaria and other parasites, intracellular RBC or granulocyte inclusions) that can occur despite normal automated blood cell counts. RBC injury may be identified by finding RBC fragments, portions of disrupted cells (schistocytes), or evidence of significant membrane alterations from sickled cells, oval-shaped cells (ovalocytes) or spherocytic cells. Target cells (thin RBCs with a central dot of hemoglobin) are RBCs with insufficient hemoglobin or excess cell membrane (eg, due to hemoglobinopathies or liver disorders). The peripheral smear can also reveal variation in RBC shape (poikilocytosis) and size (anisocytosis).

By permission of the publisher. From Tefferi A, Li C. In Atlas of Clinical Hematology. Edited by JO Armitage. Philadelphia, Current Medicine, 2004.

By permission of the publisher. From Tefferi A, Li C. In Atlas of Clinical Hematology. Edited by JO Armitage. Philadelphia, Current Medicine, 2004.

By permission of the publisher. From Tefferi A, Li C. In Atlas of Clinical Hematology. Edited by JO Armitage. Philadelphia, Current Medicine, 2004.
Reticulocyte count
The reticulocyte count is expressed as the percentage of reticulocytes (normal range, 0.5 to 1.5%) or as the absolute reticulocyte count (normal range, 50,000 to 150,000/mcL, or 50 to 150 × 10 9/L). The reticulocyte count is a crucial test in the evaluation of anemia because it informs about the response of the bone marrow and facilitates differentiation between deficient erythropoiesis (RBC production) and excessive hemolysis (RBC destruction ) as the cause of anemia. For example, higher values indicate excessive production (reticulocytosis); in the presence of anemia, reticulocytosis suggests excessive RBC destruction. Low numbers in the presence of anemia indicate decreased RBC production.
Reticulocytes are best visualized when blood is stained with a supravital stain, but because red cell reticulin is composed of RNA, which is present only in young red cells and they will only have a bluish appearance in a Wright-stained blood smear (polychromatophilia or polychromasia), which can provide a rough estimate of reticulocyte production on a routine blood smear.
Bone marrow aspiration and biopsy
Bone marrow aspiration and biopsy provide direct observation and assessment of RBC precursors. The presence of abnormal maturation (dyspoiesis) of blood cells and the amount, distribution, and cellular pattern of iron content can be assessed. Bone marrow aspiration and biopsy are usually not indicated in the evaluation of anemia and are only done when one of the following conditions is present:
Unexplained anemia
More than one cell lineage abnormality (ie, concurrent anemia and thrombocytopenia or leukopenia)
Suspected primary bone marrow disorder (eg, leukemia, multiple myeloma, aplastic anemia, myelodysplastic syndrome, metastatic carcinoma, myelofibrosis)
Cytogenetic and molecular analyses can be done on aspirate material in hematopoietic or other tumors or in suspected congenital lesions of RBC precursors (eg, Fanconi anemia). Flow cytometry can be done in suspected lymphoproliferative or myelodysplastic states to define the immunophenotype. Bone marrow aspiration and biopsy are not technically difficult and do not pose significant risk of morbidity. These procedures are safe and helpful when hematologic disease is suspected. Bone marrow aspiration and biopsy are usually can be done as a single procedure. Because biopsy requires adequate bone depth, the sample is usually taken from the posterior (or, less commonly, anterior) iliac crest. If myeloma is suspected or there is severe osteoporosis, an ultrasound-guided biopsy is done because it is the safest to avoid penetrating the pelvis.
Other tests for evaluation of anemia
Serum bilirubin and lactate dehydrogenase (LDH) can sometimes help differentiate between hemolysis and blood loss; both are elevated in hemolysis and normal in blood loss. Other tests, such as vitamin B12 and folate levels and iron and iron binding capacity, are done depending on the suspected cause of anemia. Other tests are discussed under specific anemias and bleeding disorders.






