


Conditions that cause an abnormal protein content in the blood, typically in the form of immunoglobulins, can affect vascular fragility and lead to purpura.
(See also Overview of Vascular Bleeding Disorders.)
Purpura refers to purplish cutaneous or mucosal lesions caused by hemorrhage. Small lesions (< 2 mm) are termed petechiae, and large lesions are termed ecchymoses or bruises.
Amyloidosis
Amyloidosis causes amyloid deposition within vessels in the skin and subcutaneous tissues, which may increase vascular fragility, causing purpura. Purpura typically occurs on the upper extremities in contrast to immune thrombocytopenia, in which purpura occurs mostly in the lower extremities. Periorbital purpura or a purpuric rash that develops in a nonthrombocytopenic patient after gentle stroking of the skin suggests amyloidosis.
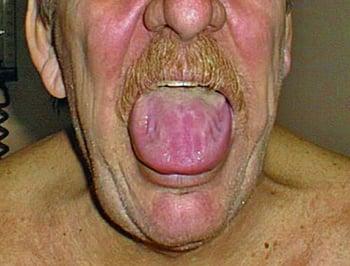
Some patients with amyloidosis have macroglossia (enlarged tongue) and can have amyloid deposits on the shoulders and in the skin.
In some patients, coagulation factor X is adsorbed by amyloid and becomes deficient, but this deficiency is usually not the cause of bleeding.

Most patients have elevated levels of serum free light chains.
The diagnosis of amyloidosis is confirmed by tissue biopsy (eg, Congo red birefringence staining of affected tissue or abdominal fat pad aspirate).
Cryoglobulinemia
Cryoglobulinemia produces immunoglobulins that precipitate when plasma is cooled (ie, cryoglobulins) while flowing through the skin and subcutaneous tissues of the extremities. Cryoglobulins may be IgG, IgM, or IgA. Mixed cryoglobulins are usually composed of IgM complexed with a monoclonal or polyclonal IgG. The immune complexes can interfere with normal platelet function and fibrin polymerization.
Monoclonal immunoglobulins formed in macroglobulinemia (lymphoplasmacytic lymphoma) or in multiple myeloma occasionally behave as cryoglobulins, as may mixed IgM-IgG immune complexes formed in some chronic infectious diseases, most commonly hepatitis C.
Cryoglobulins can also be idiopathic.
Cryoglobulinemia can also lead to small-vessel vasculitis, which can cause purpura; hyperviscosity and direct vascular trauma can contribute. Cryoglobulinemia can manifest with acral hemorrhagic necrosis, palpable purpura, livedo reticularis, and leg ulcers.
Cryoglobulins can be detected by laboratory testing.


Hypergammaglobulinemic purpura
Hypergammaglobulinemic purpura is a vasculitic purpura that primarily affects women. Recurrent crops of small, palpable purpuric lesions develop on the lower legs. These lesions leave small residual brown spots. Many patients have manifestations of an underlying immunologic disorder (eg, Sjögren syndrome, systemic lupus erythematosus).
The diagnostic finding is a polyclonal increase in IgG. Skin biopsy may be needed.
Immunoglobulin A–associated vasculitis
Immunoglobulin A–associated vasculitis (Henoch-Schonlein purpura) is an IgA-mediated small-vessel vasculitis that occurs primarily in children. It involves the skin, joints, intestine, and kidneys.
Palpable purpura develops mainly on the lower legs and buttocks. Because of its distribution, it can be confused with erythema nodosum, a reactive inflammatory panniculitis that can occur in patients with a variety of infectious, immunologic, neoplastic, and drug-induced disorders.
Hyperviscosity syndrome
Hyperviscosity syndrome, usually resulting from a markedly elevated plasma IgM concentration, may also result in purpura and other forms of abnormal bleeding (eg, profuse epistaxis) in patients with macroglobulinemia. Marked elevations of other immunoglobulins (especially IgA and IgG3) can also be associated with a hyperviscosity syndrome.






