


Hodgkin lymphoma is a localized or disseminated malignant proliferation of cells of the lymphoreticular system, primarily involving lymph node tissue, spleen, liver, and bone marrow. Symptoms typically include painless lymphadenopathy, sometimes with fever, night sweats, unintentional weight loss, pruritus, splenomegaly, and hepatomegaly. Diagnosis is based on lymph node biopsy. Treatment is curative in most cases and consists of chemotherapy with or without other treatment modalities, including antibody-drug conjugates, immunotherapy, and radiation therapy.
(See also Overview of Lymphoma.)
In the United States, it is estimated that in 2023 about 8,830 new cases of Hodgkin lymphoma will have been diagnosed, and about 900 people will have died of the disease (1). The male:female ratio is about 1.2:1. Hodgkin lymphoma is rare before age 10 years and is most common between ages 15 and 40 years; a second peak occurs in people > 60 years.
General reference
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin 2023;73(1):17-48. doi:10.3322/caac.21763
Pathophysiology of Hodgkin Lymphoma
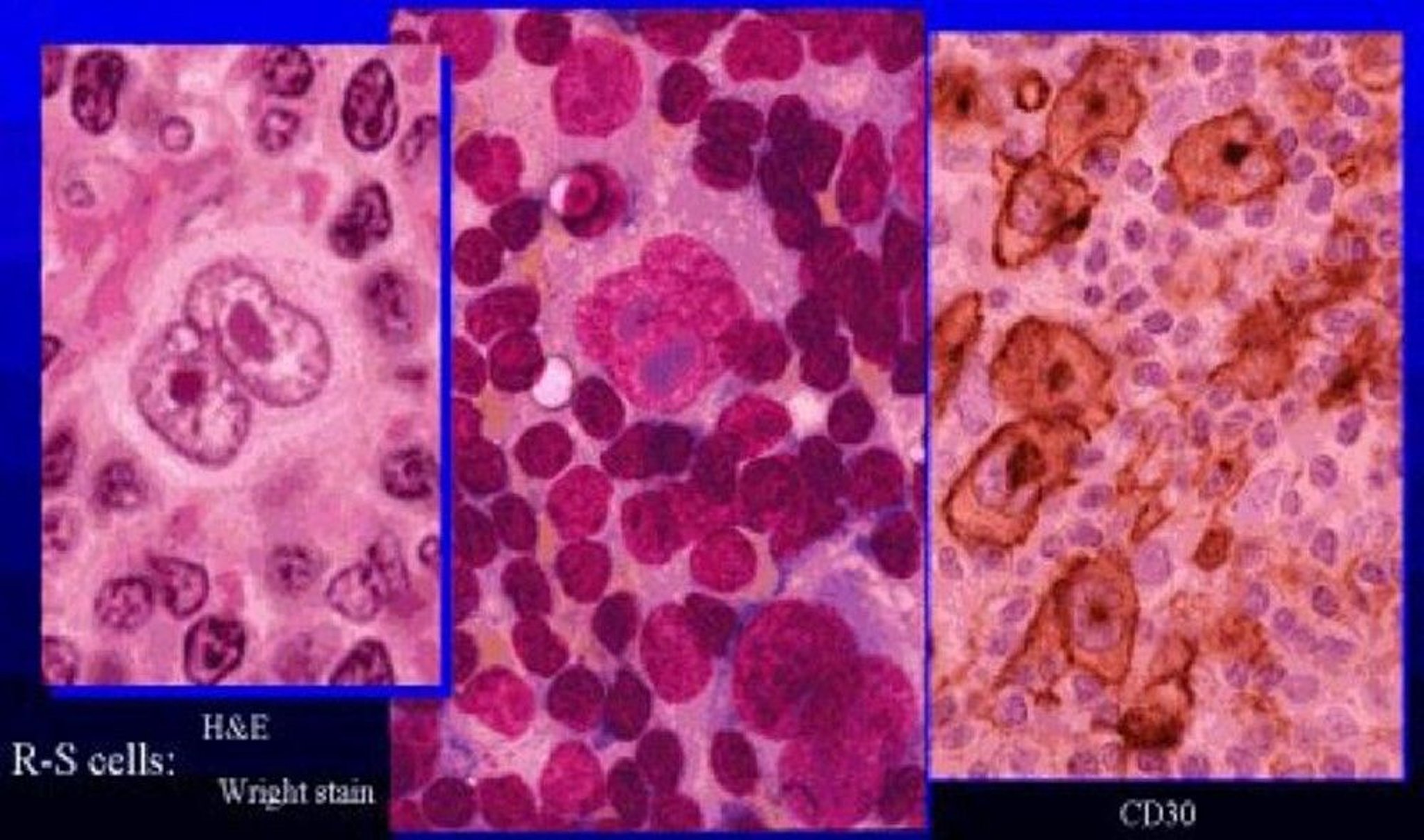
Hodgkin lymphoma results from the clonal transformation of cells of B-cell origin, giving rise to pathognomic binucleated Reed-Sternberg cells.
Epstein-Barr virus (EBV) or HIV. Risk is slightly increased in people with
Certain types of immunosuppression (eg, patients taking immunosuppressants after a transplant)
Congenital immunodeficiency disorders (eg, ataxia-telangiectasia, Klinefelter syndrome, Chédiak-Higashi syndrome, Wiskott-Aldrich syndrome)
Certain autoimmune disorders (rheumatoid arthritis, celiac disease, Sjögren syndrome, systemic lupus erythematosus)
Most patients also develop a slowly progressive defect in cell-mediated immunity (T-cell function) that, in advanced disease, contributes to common bacterial and unusual fungal, viral, and protozoal infections. Humoral immunity (antibody production) is depressed in advanced disease. Death can result from infection or progressive disease.
Symptoms and Signs of Hodgkin Lymphoma
Most patients with Hodgkin lymphoma present with painless cervical adenopathy. Although the mechanism is unclear, pain rarely may occur in diseased areas immediately after drinking alcoholic beverages, sometimes providing an early indication of the diagnosis.
Other manifestations develop as the disease spreads through the reticuloendothelial system, generally to contiguous sites. Intense pruritus refractory to usual therapies may occur early.
Systemic symptoms include fever, night sweats, and loss of appetite resulting in unintentional weight loss (> 10% of body weight in previous 6 months), which are referred to as "B symptoms." B symptoms are significant to prognosis and staging because they may signify involvement of internal lymph nodes (mediastinal or retroperitoneal), viscera (liver), or bone marrow. Splenomegaly is often present; hepatomegaly is unusual. Pel-Ebstein fever (a few days of high fever regularly alternating with a few days to several weeks of normal or below-normal temperature) occasionally occurs. Cachexia is common as disease advances.
Bone involvement is often asymptomatic but may cause vertebral osteoblastic lesions (ivory vertebrae) and, rarely, pain with osteolytic lesions and compression fractures.
Intracranial, gastric, and cutaneous lesions are rare and, when present, can suggest uncontrolled HIV-associated Hodgkin lymphoma.
Local compression by tumor masses often causes symptoms and signs, including
Jaundice secondary to intrahepatic or extrahepatic bile duct obstruction
Localized edema (lymphedema) secondary to lymphatic obstruction by the tumor
Severe dyspnea and wheezing secondary to tracheobronchial compression due to mediastinal disease
Dyspnea, cough, and/or chest discomfort due to infiltration of lung parenchyma, which may simulate lobar consolidation or bronchopneumonia
Epidural invasion that compresses the spinal cord may result in paraplegia.
Horner syndrome and laryngeal paralysis may result when enlarged lymph nodes compress the cervical sympathetic and recurrent laryngeal nerves.
Neuralgic pain follows nerve root compression.
Diagnosis of Hodgkin Lymphoma
Lymph node biopsy
FDG-PET/CT of chest, abdomen, and pelvis for staging
MRI if neurologic symptoms are present
Hodgkin lymphoma is usually suspected in patients with painless lymphadenopathy or mediastinal adenopathy detected on physical examination or routine chest x-ray (1).
Similar lymphadenopathy can result from viral infections such as infectious mononucleosis (EBV) or cytomegalovirus (CMV) infection, toxoplasmosis, non-Hodgkin lymphoma, or leukemia. Similar findings on chest radiograph can result from lung cancer, sarcoidosis, or tuberculosis.
Evaluation of a mediastinal mass is discussed elsewhere.

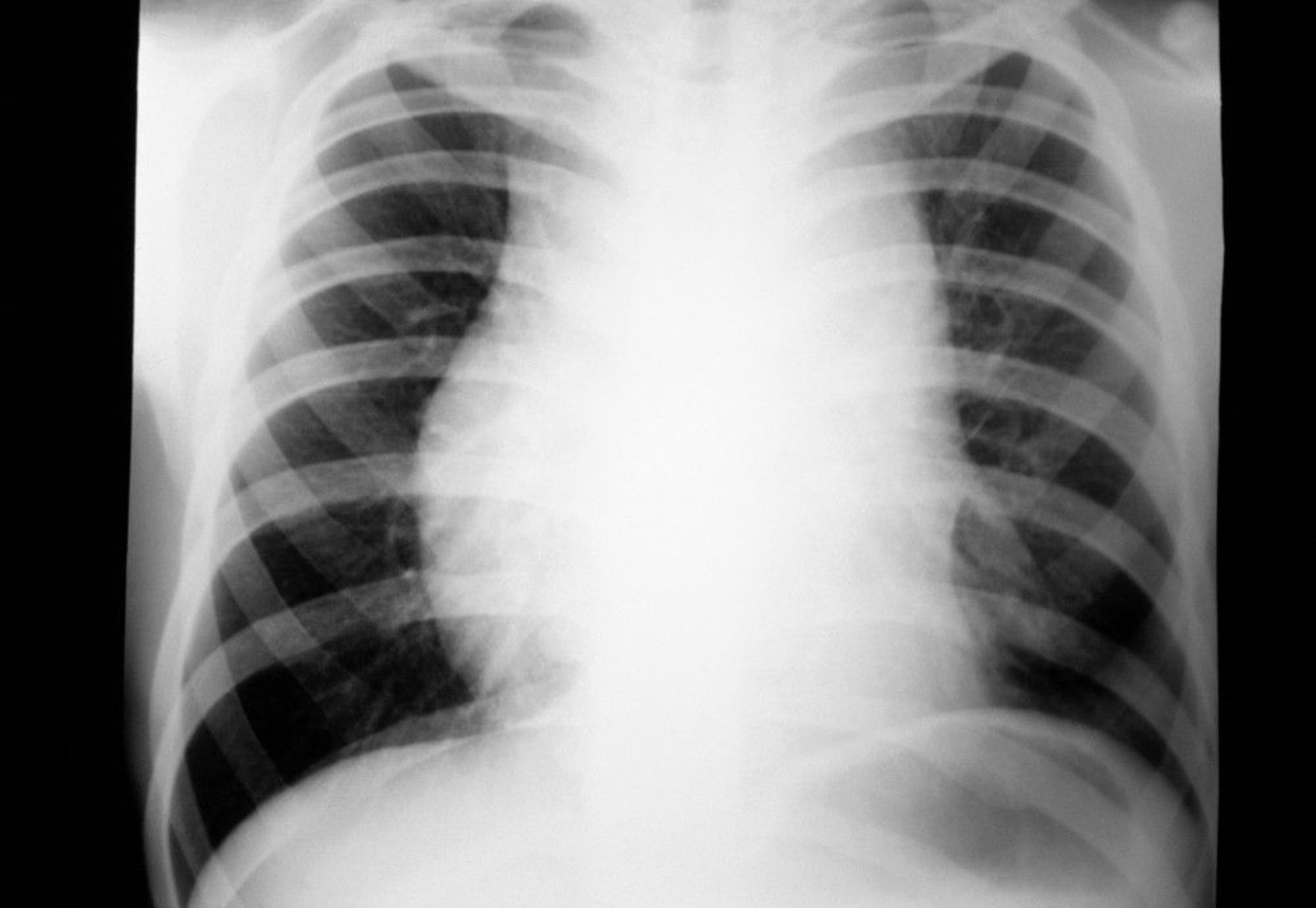
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Chest radiograph or physical examination abnormalities should be confirmed with CT or positron emission tomography (PET) scan of the chest in order to choose the most efficient biopsy procedure. If only mediastinal nodes are enlarged, mediastinoscopy, video-assisted thoracoscopy (VATS), or a Chamberlain procedure (a limited left anterior thoracostomy allowing biopsy of mediastinal lymph nodes inaccessible by cervical mediastinoscopy) may be indicated. CT-guided core needle biopsy may also be considered; fine-needle aspiration is often inadequate for the diagnosis of Hodgkin lymphoma.
Biopsy reveals Reed-Sternberg cells (large, binucleated cells) in a characteristically heterogeneous cellular infiltrate, consisting of histiocytes, lymphocytes, monocytes, plasma cells, and eosinophils. Classic Hodgkin lymphoma has 4 histopathologic subtypes (2) (see table Histopathologic Subtypes of Hodgkin Lymphoma):
Nodular sclerosis: Dense fibrous tissue surrounding nodules of Hodgkin tissue
Mixed cellularity: A moderate number of Reed-Sternberg cells with a mixed background infiltrate
Lymphocyte-rich: Few Reed-Sternberg cells but many B cells
Lymphocyte-depleted: Numerous Reed-Sternberg cells plus extensive fibrosis
Nodular lymphocyte-predominant Hodgkin lymphoma has been reclassified as a non-Hodgkin B-cell lymphoma by the International Consensus Classification and is called nodular lymphocyte predominant B-cell lymphoma (3).

Courtesy of the FDA.
Complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), lactate dehydrogenase (LDH), and kidney function and liver tests are generally done. Test results may be abnormal but are nondiagnostic.
CBC may show a slight polymorphonuclear leukocytosis. Lymphocytopenia may occur early and is an adverse prognostic factor. Eosinophilia is common, and thrombocytosis also may be present. Anemia, often microcytic, usually develops with advanced disease. In advanced anemia, defective iron reutilization is characterized by a low serum iron level, low iron-binding capacity, an elevated serum ferritin level, and an increased bone marrow iron level. Pancytopenia is occasionally caused by bone marrow invasion, more commonly in the lymphocyte-depleted subtype.
Elevated serum alkaline phosphatase levels may be present, but elevations do not always indicate bone marrow or liver involvement. Increases in leukocyte alkaline phosphatase, serum haptoglobin, and other acute-phase reactants usually reflect the presence of inflammatory cytokines due to active Hodgkin lymphoma. These substances are measured and tests are sometimes done to evaluate nonspecific symptoms, and results can suggest Hodgkin lymphoma; they are not done on all lymphoma patients. Erythrocyte sedimentation rate (ESR), an indirect marker of inflammation, is commonly ordered and elevation predicts a less favorable outcome.
Hypersplenism may occur in patients with marked splenomegaly.
A combined fluorodeoxyglucose (FDG)-PET/CT scan of the chest, abdomen, and pelvis is the imaging study of choice for staging Hodgkin lymphoma (see below). Bone lesions are detected more commonly with the use of FDG-PET imaging. If combined FDG-PET/CT is not available, a contrast-enhanced CT scan of the chest, abdomen, and pelvis is done.
A bone marrow biopsy is usually only done if a PET/CT scan is not obtained and if the findings might alter management.
Staging
After diagnosis, stage is determined to guide therapy. The commonly used Lugano staging system (see table Lugano Staging of Hodgkin and Non-Hodgkin Lymphomas) incorporates
Symptoms
Physical examination findings
Results of imaging tests, including CT of the chest, abdomen, and pelvis, and functional imaging with FDG-PET
Sometimes bone marrow biopsy findings
Laparotomy is not required for staging.
Diagnosis references
1. Cheson BD, Fisher RI, Barrington SF, et al: Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J Clin Oncol 32(27):3059–3068, 2014.
2. Alaggio R, Amador C, Anagnostopoulos I, et al: The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms [published correction appears in Leukemia 2023 Sep;37(9):1944-1951]. Leukemia 36(7):1720–1748, 2023. doi:10.1038/s41375-022-01620-2
3. Campo E, Jaffe ES, Cook JR, et al. The International Consensus Classification of Mature Lymphoid Neoplasms: a report from the Clinical Advisory Committee [published correction appears in Blood 2023 Jan 26;141(4):437]. Blood 2022;140(11):1229-1253. doi:10.1182/blood.2022015851
Treatment of Hodgkin Lymphoma
Chemotherapy
Immunotherapy (eg, immune checkpoint inhibitors)
Radiation therapy
Sometimes autologous stem cell transplantation
The choice of treatment modality is complex and depends on the precise stage of disease. Before treatment and when applicable, patients should discuss options to preserve fertility with their oncologists and a fertility specialist.
Initial treatment
Limited-stage diseaseradiation therapy>60 years due to increased risk of pulmonary toxicity.
Advanced-stage disease12, 3). Optimal management of very old or frail patients is not standardized.
Subsequent treatment
Multiple second-line chemotherapy regimens are considered acceptable for patients who are not cured with first-line therapy. For patients who achieve a good response to second-line therapy, high-dose chemotherapy and autologous stem cell transplantation should be considered, while non-responders may be candidates for subsequent lines of therapy or allogeneic stem cell transplantation.
4, 5).
Complications of treatment
Radiation therapy carries increased risk of malignant solid tumors (eg, breast, gastrointestinal, lung, thyroid, soft tissue).
cardiomyopathy, coronary atherosclerosis and valvular heart disease.
Immune checkpoint inhibitors are associated with immune-related toxicities.
Posttreatment surveillance
All patients who are not PET-negative at the end of induction therapy should have a biopsy or be followed closely with serial imaging; if residual disease is present, additional treatment is necessary. Once in remission, patients should be followed for signs and symptoms of relapse for 5 years. Those with manifestations of relapse, defined as reappearance of disease at sites of prior disease or at new sites, should have imaging with PET/CT or CT alone. Routine, scheduled imaging in asymptomatic patients is not mandatory. For a schedule of posttreatment surveillance, see table Hodgkin Lymphoma Posttreatment Surveillance.
Treatment references
1. Johnson P, Federico M, Kirkwood A, et al: Adapted treatment guided by interim PET-CT scan in advanced Hodgkin's lymphoma. N Engl J Med 374(25):2419– 2429, 2016.
2. Connors JM, Jurczak W, Straus DJ, et al: Brentuximab vedotin with chemotherapy for stage III or IV Hodgkin's lymphoma. N Engl J Med 378(4):331–344, 2018. Epub 2017 Dec 10.
3. Straus DJ, Długosz-Danecka M, Connors JM, et al: Brentuximab vedotin with chemotherapy for stage III or IV classical Hodgkin lymphoma (ECHELON-1): 5-year update of an international, open-label, randomised, phase 3 trial. Lancet Haematol 8(6):e410–e421, 2021. doi: 10.1016/S2352-3026(21)00102-2
4. Armand P, Engert A, Younes A, et al: Nivolumab for Relapsed/Refractory Classic Hodgkin Lymphoma After Failure of Autologous Hematopoietic Cell Transplantation: Extended Follow-Up of the Multicohort Single-Arm Phase II CheckMate 205 Trial [published correction appears in J Clin Oncol 2018 Sep 10;36(26):2748]. J Clin Oncol 36(14):1428–1439, 2018. doi:10.1200/JCO.2017.76.0793
5. Chen R, Zinzani PL, Fanale MA, et al: Phase II Study of the Efficacy and Safety of Pembrolizumab for Relapsed/Refractory Classic Hodgkin Lymphoma. J Clin Oncol 35(19):2125–2132, 2017. doi:10.1200/JCO.2016.72.1316
Prognosis for Hodgkin Lymphoma
About 85 to 90% of patients with limited-stage classic Hodgkin lymphoma are cured compared with 75 to 80% of patients with advanced-stage disease (1). Limited-stage disease is frequently subdivided into favorable and unfavorable prognostic groups. Unfavorable disease is based on risk factors, for example:
Presence of bulky disease
≥ 4 nodal sites involved
Age > 50 years
Erythrocyte sedimentation rate (ESR) > 50 mm/hour with no B symptoms or > 30 mm/hour with B symptoms (weight loss, fever, night sweats)
Risk factors in advanced-stage Hodgkin lymphoma include
Male sex
Age > 45 years
Stage 4 disease
Signs of tumor-induced inflammation (low albumin, anemia, leukocytosis, and lymphopenia)
However, selection of which risk factors to use in estimating prognosis is still subject to revision. Patients who do not achieve complete remission with treatment, or who relapse within 12 months have a poor prognosis.
Prognosis reference
1. National Institutes of Health: National Cancer Institute Surveillance, Epidemiology, and End-Results (SEER) Program. Cancer Stat Facts—Hodgkin Lymphoma. SEER 2023
Key Points
Hodgkin lymphoma is of B cell origin.
Patients usually present with painless lymphadenopathy or with incidental cervical or mediastinal adenopathy discovered on chest radiograph or physical examination.
Biopsy shows pathognomonic, binucleated Reed-Sternberg cells.
Most patients are cured using combination chemotherapy and sometimes additional systemic therapies or radiation therapy.
More Information
The following English language resource provides information for clinicians and support and information for patients. THE MANUAL is not responsible for the content of this resource.
Leukemia & Lymphoma Society: Resources for Healthcare Professionals : provides educational resources for health care practitioners as well as information for patient referrals






