


There has been a gradual decrease in overall transfusion due to patient blood management programs. The total components transfused in 2019 (subsequent data will be skewed due to COVID-19) was approximately 15 million (1), down from approximately 16 million units of blood components transfused in 2017 in the United States (2). Although transfusion is probably safer than ever, risk (and the public’s perception of risk) mandates informed consent whenever practical.
In the United States, the collection, storage, and transport of blood and its components are standardized and regulated by the FDA, by the AABB (formerly known as the American Association of Blood Banks), and sometimes by state or local health authorities. Donor screening includes an extensive questionnaire and health interview; measurement of temperature, heart rate, and blood pressure; and hemoglobin (Hb) determination. Some potential donors are deferred either temporarily or permanently (see table Some Reasons for Blood Donation Deferral or Denial). Criteria for deferral protect prospective donors from possible ill effects of donation and protect recipients from disease.
Whole blood donations are limited to once every 56 days, whereas apheresis red blood cell (RBC) donations (donations of twice the usual amount of RBCs in one sitting, with the separated plasma being returned to the donor) are limited to once every 112 days. Apheresis platelet donations are limited to once every 72 hours with a maximum of 24/year. With rare exceptions, blood donors are unpaid. (See also the American Red Cross for information regarding donor eligibility.)
In a standard blood donation, approximately 450 mL of whole blood is collected in a plastic bag containing an anticoagulant preservative. Whole blood or packed RBCs preserved with citrate-phosphate-dextrose-adenine may be stored for 35 days. Packed RBCs may be stored for 42 days if an adenine-dextrose-saline solution is added.
Autologous donation, which is use of the patient’s own blood, is less preferred as a method of transfusion. When done before elective surgery, up to 3 or 4 units of whole blood or packed RBCs are collected in the 2 to 3 weeks preceding surgery. The patient is then given iron supplements. Such elective autologous donation may be considered when matched blood is difficult to obtain because the patient has made antibodies to red cell antigens or has a rare blood type. Special blood salvage procedures are also available for collecting and autotransfusing blood shed after trauma and during surgery.
General references
1. Jones JM, Sapiano MRP, Mowla S, et al: Has the trend of declining blood transfusions in the United States ended? Findings of the 2019 National Blood Collection and Utilization Survey. Transfusion 61(Suppl 2):S1–S10, 2021. doi: 10.1111/trf.16449
2. Jones JM, Sapiano MPR, Savinkina AA, et al: Slowing decline in blood collection and transfusion in the United States - 2017. Transfusion 60(Suppl 2):S1–S9, 2020. doi: 10.1111/trf.15604
Pretransfusion Testing
Donor blood testing includes
ABO and Rho(D) antigen typing
Antibody screening
Testing for infectious disease markers (see table Infectious Disease Transmission Testing)
Compatibility testing
Tests the recipient’s RBCs for antigens A, B, and Rho(D)
Screens the recipient’s plasma for antibodies against RBC antigens
Includes a cross-match to ensure that the recipient’s plasma is compatible with antigens on donor RBCs
Compatibility testing is done before a transfusion; however, in an emergency, testing is done after releasing blood from the blood bank. Testing can also help in diagnosing transfusion reactions.
The addition of a cross-match to ABO/Rh typing and antibody screening increases detection of incompatibility by only 0.01%. Therefore, many hospitals do computerized electronic cross-matches rather than physical cross-matches in a test tube in patients who have negative antibody screening. If the recipient has a clinically significant anti-RBC antibody, donor blood is restricted to RBC units negative for the corresponding antigen; further testing for compatibility is done by combining recipient plasma, donor RBCs, and antihuman globulin. In recipients without clinically significant anti-RBC antibodies, an immediate spin cross-match, which omits the antiglobulin phase, confirms ABO compatibility.
Emergency transfusion is done when not enough time (generally < 60 minutes) is available for thorough compatibility testing because the patient is in hemorrhagic shock. When time permits (approximately 10 minutes is needed), ABO/Rh type-specific blood may be given. In more urgent circumstances, type O RBCs are transfused if the ABO type is uncertain, and Rh-negative blood is given to females of child-bearing age if the Rh type is uncertain; otherwise, either Rh-negative or Rh-positive O blood can be used.
“Type and screen” may be requested in circumstances that are not likely to require transfusion, as in surgery in which the risk of bleeding is low. The patient’s blood is typed for ABO/Rh antigens and screened for antibodies. If antibodies are absent and the patient needs blood, ABO/Rh type–specific or compatible RBCs may be released without the antiglobulin phase of the cross-match. If an unexpected antibody is present, full testing is required. "Type and cross" is requested for procedures in which there is a high bleeding risk (eg, cardiac bypass surgery), and the number of units for cross matching is specified.
ABO and Rh typing
ABO typing of donor and recipient blood is done to prevent transfusion of incompatible RBCs (see figure Compatible RBC Types). As a rule, blood for transfusion should be of the same ABO type as that of the recipient. In urgent situations or when the correct ABO type is in doubt or unknown, type O Rh-negative packed RBCs (not whole blood—see Acute Hemolytic Transfusion Reaction), which contains neither A nor B antigens, may be used for patients of any ABO type.
Compatible RBC Types

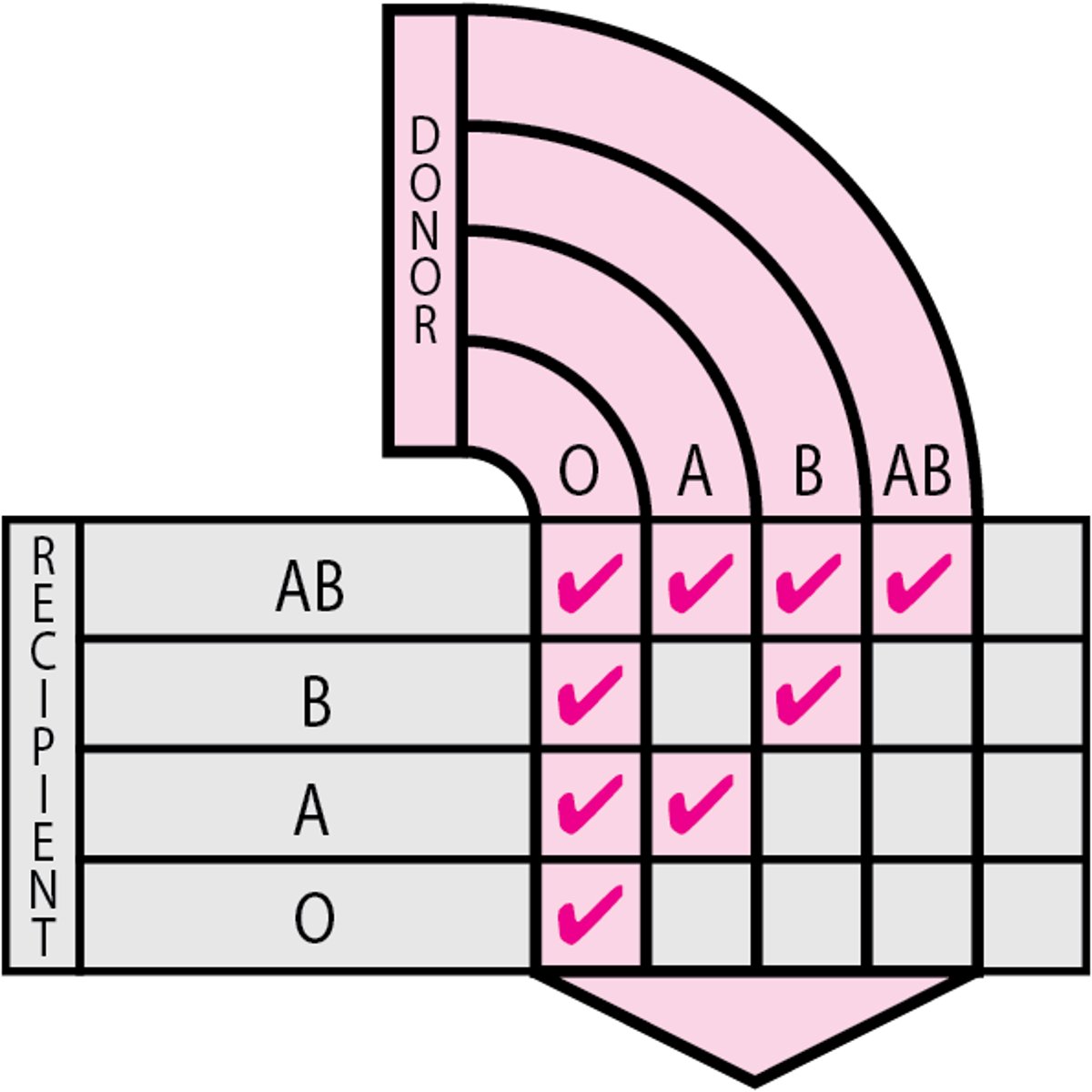
Rh typing determines whether the Rh factor Rho(D) is present on (Rh-positive) or absent from (Rh-negative) the RBCs. Rh-negative patients should always receive Rh-negative blood except in life-threatening emergencies when Rh-negative blood is unavailable. Rh-positive patients may receive Rh-positive or Rh-negative blood. Occasionally, RBCs from some Rh-positive people react weakly on standard Rh typing (weak D, or Du, positive), but these people are still considered Rh-positive.
Antibody screening
Antibody screening for unexpected anti-RBC antibodies is routinely done on blood from prospective recipients and prenatally on maternal specimens. Unexpected anti-RBC antibodies are specific for RBC blood group antigens other than A and B [eg, Rho(D), Kell (K), Duffy (Fy)]. Early detection is important because such antibodies can cause serious hemolytic transfusion reactions or hemolytic disease of the fetus and neonate, and they may greatly complicate compatibility testing and delay procurement of compatible blood.
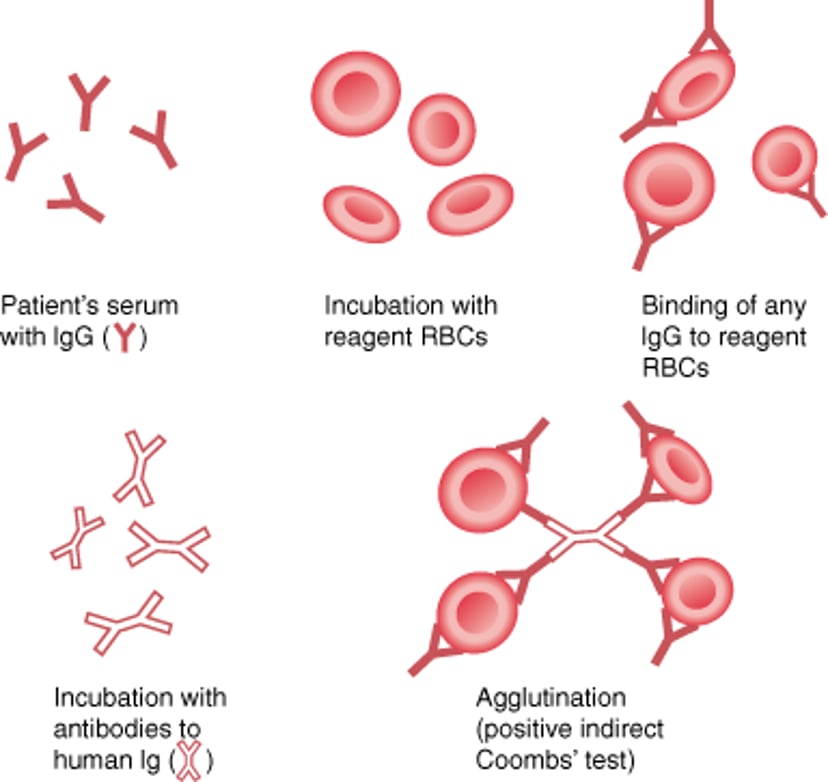
Indirect antiglobulin testing (the indirect Coombs test) is used to screen for unexpected anti-RBC antibodies (see figure Indirect Antiglobulin (Indirect Coombs) Test). This test may be positive in the presence of an unexpected blood group antibody or when free (non-RBC–attached) antibody is present in autoimmune hemolytic anemias. Reagent RBCs are mixed with the patient’s plasma or serum, incubated, washed, tested with antihuman globulin, and observed for agglutination. Once an antibody is detected, its specificity is determined. Knowing the specificity of the antibody is helpful for assessing its clinical significance, selecting compatible blood, and managing hemolytic disease of the fetus and neonate.
Indirect Antiglobulin (Indirect Coombs) Test
The indirect antiglobulin (indirect Coombs) test is used to detect IgG antibodies against red blood cells (RBCs) in a patient's plasma. The patient's plasma is incubated with reagent RBCs; then Coombs serum (antibodies to human IgG, or human anti-IgG) is added. If agglutination occurs, IgG antibodies (autoantibodies or alloantibodies) against RBCs are present. This test is also used to determine the specificity of an alloantibody. |

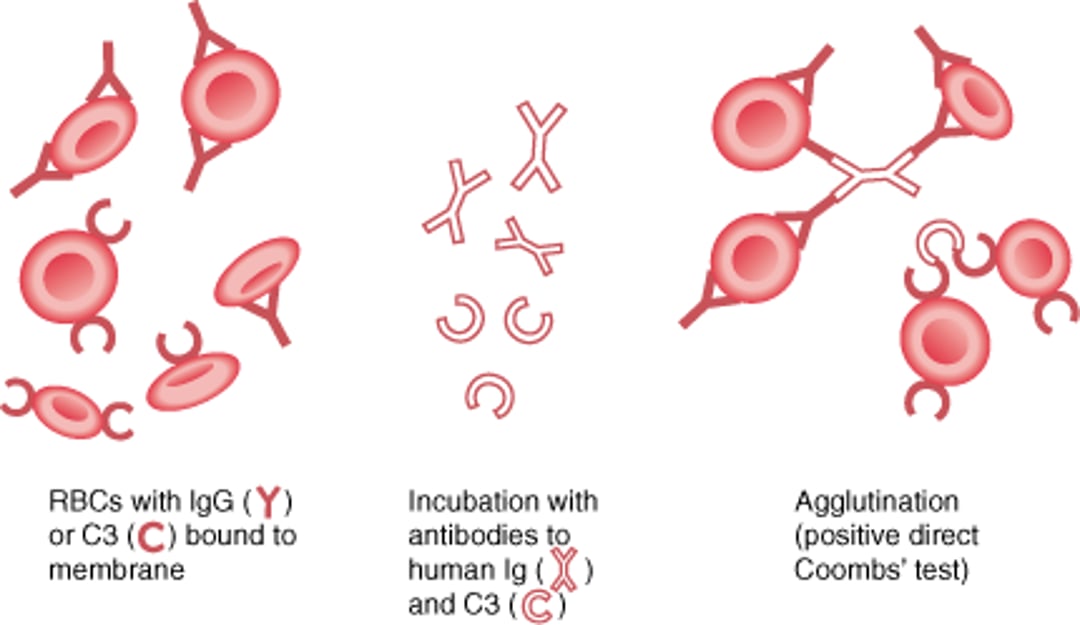
Direct antiglobulin testing (the direct Coombs test) detects antibodies that have coated the patient’s RBCs in vivo (see figure Direct Antiglobulin (Direct Coombs) Test). It is used when immune-mediated hemolysis is suspected. Patients’ RBCs are directly tested with antihuman globulin and observed for agglutination. A positive result, if correlated with clinical findings and laboratory indicators of hemolysis, suggests autoimmune hemolytic anemia, drug-induced hemolysis, a transfusion reaction, or hemolytic disease of the newborn.
Direct Antiglobulin (Direct Coombs) Test
The direct antiglobulin (direct Coombs) test is used to determine whether red blood cell (RBC)-binding antibody (IgG) or complement (C3) is present on RBC membranes. The patient's RBCs are incubated with antibodies to human IgG and C3. If IgG or C3 is bound to RBC membranes, agglutination occurs—a positive result. A positive result suggests the presence of autoantibodies to RBCs. A positive test result does not always equate with hemolysis. Thus, results should always be correlated with the clinical signs and symptoms. |

Antibody titration is done when a clinically significant, unexpected anti-RBC antibody is identified in the plasma of a patient who is pregnant or in a patient with cold agglutinin disease. The maternal antibody titer correlates fairly well with the severity of hemolytic disease in the fetus with the corresponding antigen and is often used to guide treatment in hemolytic disease of the fetus and neonate along with ultrasonography and amniotic fluid study.
Infectious disease testing
Donated blood products are tested for the presence of a number of infectious agents (see table Infectious Disease Transmission Testing).
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
CDC: Blood Safety Basics
FDA May 2023 Guidance document: Recommendations for Evaluating Donor Eligibility Using Individual Risk-Based Questions to Reduce the Risk of Human Immunodeficiency Virus Transmission by Blood and Blood Products.






