


Chronic mucocutaneous candidiasis is persistent or recurrent candidal infection due to inherited T-cell defects. Autoimmune and endocrine disorders may develop in its recessive form. Diagnosis is based on recurrent, unexplained candida infections. Treatment includes antifungal drugs and treatment of any endocrine and autoimmune disorders.
(See also Overview of Immunodeficiency Disorders and Approach to the Patient With an Immunodeficiency Disorder.)
Chronic mucocutaneous candidiasis is a primary immunodeficiency disorder that involves T cell defects. Some patients also have deficient humoral immunity (sometimes called antibody deficiency), characterized by abnormal antibody responses to polysaccharide antigens despite normal immunoglobulin levels.
Inheritance may be
Autosomal dominant: Involving a mutation in the signal transducer and activator of transcription 1 gene (STAT1)
Autosomal recessive: Involving a mutation in the autoimmune regulator gene (AIRE)
In the recessive form (autoimmune polyendocrinopathy–candidosis-ectodermal dystrophy), autoimmune manifestations typically develop; they include endocrine disorders (eg, hypoparathyroidism, adrenal insufficiency, hypogonadism, thyroid disorders, diabetes), alopecia areata, pernicious anemia, and hepatitis. Mutations may also occur in genes that encode various proteins involved in the innate immune response to fungi—notably, the following:
PTPN22 (protein tyrosine phosphatase, non-receptor type 22 [also called LYP, or lymphoid tyrosine phosphatase], which is involved in T-cell–receptor signalling)
Dectin-1 (an innate pattern recognition receptor essential for the control of fungal infections)
CARD9 (caspase recruitment domain-containing protein 9, which is an adaptor molecule important in the production of interleukin (IL)-17 and for protection against fungal invasion)
Patients (dominant and recessive) have cutaneous anergy to Candida, absent proliferative responses to Candida antigen (but normal proliferative responses to mitogens), and intact antibody response to Candida and other antigens. Mucocutaneous candidiasis recurs or persists, usually beginning during infancy but sometimes during early adulthood. Life span is not affected.
Symptoms and Signs of Chronic Mucocutaneous Candidiasis
Thrush is common, as are candidal infections of the scalp, skin, nails, and gastrointestinal and vaginal mucosa. Severity varies. Nails may be thickened, cracked, and discolored, with edema and erythema of the surrounding periungual tissue, resembling clubbing. Skin lesions are crusted, pustular, erythematous, and hyperkeratotic. Scalp lesions may result in scarring alopecia.
Infants often present with refractory thrush, candidal diaper rash, or both.

Image courtesy of CDC/Sherry Brinkman via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image provided by Thomas Habif, MD.

Image provided by Kristle Lynch, MD.


Image courtesy of CDC/Sherry Brinkman via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image provided by Thomas Habif, MD.

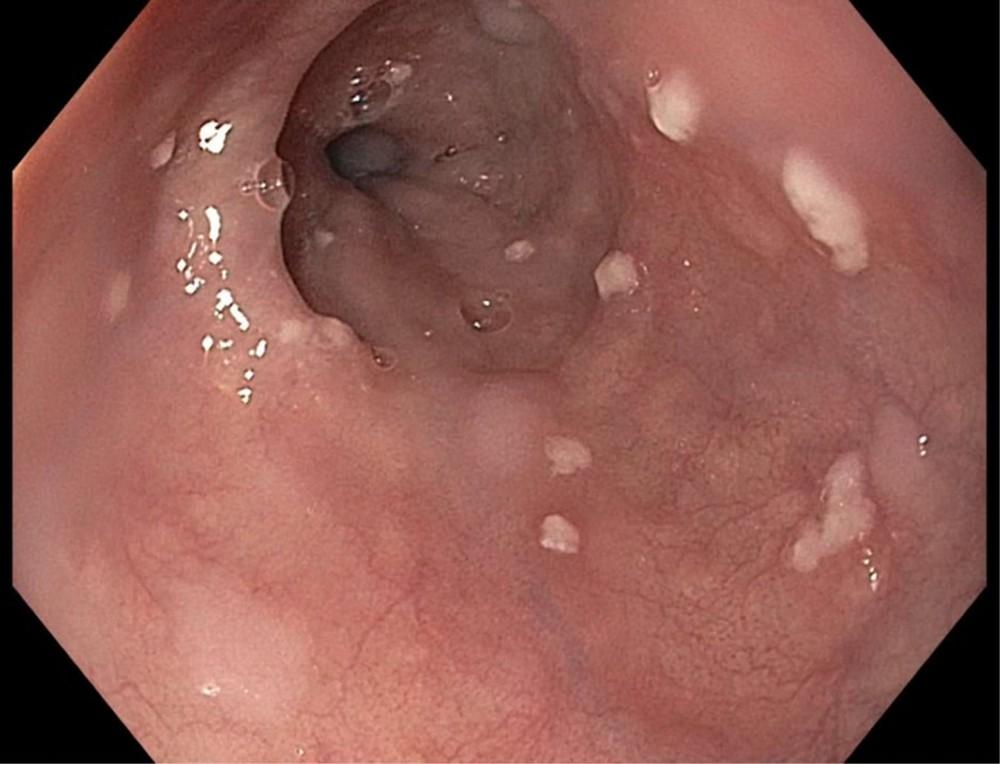
Image provided by Kristle Lynch, MD.
Diagnosis of Chronic Mucocutaneous Candidiasis
Clinical evaluation
Candidal lesions are confirmed by standard tests (eg, potassium hydroxide wet mount of scrapings).
Diagnosis of chronic mucocutaneous candidiasis is based on the presence of recurrent candidal skin or mucosal lesions when no other known causes of candidal infection (eg, diabetes, antibiotic use) are present.
Patients are screened for endocrine disorders based on clinical suspicion.
Genetic testing is done if clinical suspicion is high and other common causes of the patient's clinical symptoms have been eliminated. If an AIRE mutation is detected, screening can be offered to the patient's siblings and children.
Treatment of Chronic Mucocutaneous Candidiasis
Antifungal drugs
Treatment of endocrine and autoimmune manifestations
Autoimmune (including endocrine) manifestations are treated aggressively.
Hematopoietic stem cell transplantation has rarely been successful and could be considered as last-line treatment in severe cases.
Key Points
Inheritance of chronic mucocutaneous candidiasis is autosomal dominant or recessive.
Patients with the recessive form can have autoimmune (including endocrine) manifestations.
Diagnose the disorder by confirming mucocutaneous candidiasis and excluding other causes.
Treat candidiasis with antifungal drugs (using a systemic drug if needed), and treat autoimmune manifestations.






