


Meningococci (Neisseria meningitidis) are gram-negative diplococci that cause meningitis and meningococcemia. Symptoms, usually severe, include headache, nausea, vomiting, photophobia, lethargy, rash, multiple organ failure, shock, and disseminated intravascular coagulation. Diagnosis is clinical, confirmed by culture. Treatment is penicillin or a third-generation cephalosporin.
Meningococci are gram-negative aerobic diplococci that belong to the family Neisseriaceae. There are 13 serogroups; 6 serogroups (A, B, C, W135, X, and Y) cause most human disease.
Worldwide, the incidence of endemic meningococcal disease is 0.5 to 5/100,000, with an increased number of cases during winter and spring in temperate climates. Local outbreaks occur most frequently in sub-Saharan Africa between Gambia and Senegal in the west and Ethiopia, Eritrea, and northern Kenya in the east; this area is known as the sub-Saharan (African) meningitis belt, which includes 26 countries. In major African epidemics (which were often caused by serogroup A), attack rates ranged from 100 to 800/100,000 and affected up to 200,000 people each year. After widespread use of the meningococcal A vaccine in the African meningitis belt, serogroup A has been replaced by other meningococcal serogroups and by Streptococcus pneumoniae.
In the US, the annual incidence ranges from 0.12 to 1.1/100,000. Over the past 20 years, incidence of meningococcal disease has declined annually. Most cases are sporadic, typically in children < 2 years of age. Outbreaks of meningococcal disease are rare in the US, and only about 1 in 20 cases (5%) is related to an outbreak (see the Centers for Disease Control and Prevention's [CDC] Meningococcal Outbreaks). Outbreaks tend to occur in semiclosed communities (eg, military recruit camps, college dormitories, schools, day care centers) and most often involve patients 16 to 23 years of age. Serogroups B and C cause 50 to 80% of invasive disease (1). Serogroup A is rare in the US.
Reference
1. Centers for Disease Control and Prevention: The Pink Book: Meningococcal Disease. Accessed 08/24/2022.
Diseases Caused by Meningococci
Over 90% of meningococcal infections involve
Meningococcemia
(See also Bacterial Meningitis in Infants Over 3 Months of Age.)
Infections of lungs, joints, respiratory passageways, genitourinary organs, rectum, eyes, endocardium, and pericardium may occur but are less common.
N. meningitidis has been reported to cause urethritis and cervicitis. Recently, the incidence of meningococcal urethritis has been increasing in men who have sex with men and typically follows orogenital contact with an oropharyngeal meningococcal carrier. N. meningitidis colonizes the nasopharynx. N. meningitidis may also cause proctitis, primarily in men who have sex with men.
Pathophysiology of Meningococcal Diseases
Meningococci can asymptomatically colonize the nasopharynx (carrier state). Despite documented high rates of colonization (5 to 40% of healthy people), which may be transient, brief, or prolonged, transition to invasive disease is rare (< 1%). A combination of factors is probably responsible for transition from carrier state to invasive disease, which occurs primarily in previously uninfected patients. Carriers (and infected patients) may transmit the organism to people who have direct contact with respiratory secretions or who inhale large-droplet nuclei from a carrier or patient. Nasopharyngeal carriage rates are highest in adolescents and young adults, who serve as reservoirs for transmission of N. meningitidis. Carrier rates rise dramatically during epidemics.
After invading the body, N. meningitidis causes meningitis and severe bacteremia in children and adults, resulting in profound vascular effects. Infection can rapidly become fulminant. The case-fatality rate is 4 to 6% for meningitis alone, compared with up to 40% for meningococcemia with septic shock.
Risk factors
The most frequently infected are
Children aged 6 months to 3 years
Other high-risk groups include
Adolescents and young adults (16 to 20 years of age)
Military recruits
College freshmen living in dormitories
Travelers to places where meningococcal disease is common (eg, certain countries in Africa and in Saudi Arabia during the Hajj)
People with functional or anatomic asplenia or a complement deficiency
People living with HIV infection
Microbiologists working with N. meningitidis isolates
Close contacts of patients with invasive meningococcal disease
Infection or vaccination confers serogroup-specific immunity.
Antecedent viral infection, household crowding, chronic underlying illness, and both active and passive smoking are associated with increased risk of meningococcal disease (1).
Pathophysiology reference
1.Mbaeyi SA, Bozio CH, Duffy J, et al: Meningococcal Vaccination: Recommendations of the Advisory Committee on Immunization Practices, United States, 2020. MMWR Recomm Rep 69(No. RR-9):1–41, 2020. doi: 10.15585/mmwr.rr6909a1
Symptoms and Signs of Meningococcal Diseases
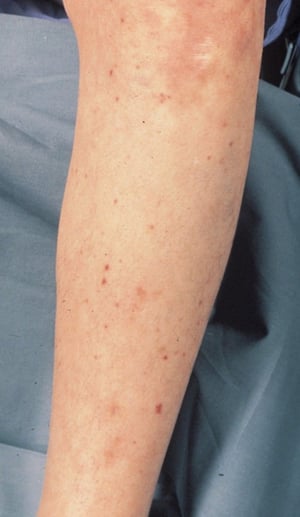
Patients with meningitis frequently report fever, headache, and stiff neck. Other symptoms include nausea, vomiting, photophobia, and lethargy. A maculopapular or hemorrhagic petechial rash often appears soon after disease onset. Meningeal signs are often apparent during physical examination.
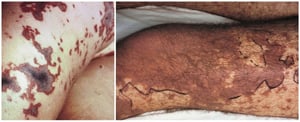
Fulminant meningococcemia syndromes include Waterhouse-Friderichsen syndrome (septicemia, profound shock, cutaneous purpura, adrenal hemorrhage), sepsis with multiple organ failure, shock, and disseminated intravascular coagulation. A rare, chronic meningococcemia causes recurrent mild symptoms (mostly joint and cutaneous).
Complications of meningococcal meningitis are common and serious. Of patients who recover, 10 to 20% have serious sequelae, such as permanent hearing loss, intellectual disability, or loss of phalanges or limbs.

Image courtesy of Mr. Gust via the Public Health Image Library of the Centers for Disease Control and Prevention.

© Springer Science+Business Media
© Springer Science+Business Media

Image courtesy of Karen McKoy, MD.

© Springer Science+Business Media
© Springer Science+Business Media


Image courtesy of Mr. Gust via the Public Health Image Library of the Centers for Disease Control and Prevention.


© Springer Science+Business Media


© Springer Science+Business Media


Image courtesy of Karen McKoy, MD.


© Springer Science+Business Media


© Springer Science+Business Media
Diagnosis of Meningococcal Diseases
Gram stain and culture
Sometimes nucleic acid–based testing (NAAT) such as polymerase chain reaction (PCR)
Neisseria are small, gram-negative diplococci readily identified with Gram stain and by other standard bacteriologic identification methods. Serologic methods, such as latex agglutination and coagglutination tests, allow rapid presumptive diagnosis of N. meningitidis in blood, cerebrospinal fluid, synovial fluid, and urine. However, both positive and negative results should be confirmed by culture.
PCR testing of cerebrospinal fluid, blood, and other normally sterile sites for N. meningitidis is more sensitive and specific than culture and may be useful when the cerebrospinal fluid Gram stain is negative and when prior antibiotic administration interferes with isolating the organism.
Because meningococci and gonococci appear similar on Gram stain, meningococcal urethritis should be considered if the urethral discharge shows gram-negative diplococci, but the NAAT is negative for gonococci; this situation requires culture of the urethral discharge to identify the Neisseria species causing the infection (see Diseases Characterized by Urethritis and Cervicitis from the CDC).
Treatment of Meningococcal Diseases
> 50 years, coverage for Listeria monocytogenes
Once N. meningitidis has been definitively identified, the preferred treatment is one of the following:
Penicillin 4 million units IV every 4 hours
penicillin, those countries typically give initial treatment with a third-generation cephalosporin, such as ceftriaxone or cefotaxime. Also, when penicillin is used, follow-up treatment with ceftriaxone
Corticosteroids decrease the incidence of neurologic complications in children and adults with suspected bacterial meningitis due to Haemophilus influenzae type b or S. pneumoniae. The evidence is less clear when N. meningitidis
Meningococcal urethritis is treated with the same drug regimens as gonococcal urethritis. The risk of sexual transmission of meningococcal urethritis is unclear; however, treatment of sex partners can be considered (see Diseases Characterized by Urethritis and Cervicitis from the CDC).
Prevention of Meningococcal Diseases
Antibiotic prophylaxis
Close contacts of people with meningococcal disease are at increased risk of acquiring disease and should receive a prophylactic antibiotic.
Options include
< 1 month, 5 mg/kg) orally every 12 hours for 4 doses
< 15 years, 125 mg; for children ≥ 15 years, 250 mg) IM for 1 dose
rifampin for chemoprophylaxis and so could be an alternative for patients with contraindications to recommended drugs.
Ciprofloxacin-resistant meningococcal disease is rare but has been reported in several countries (Greece, England, Wales, Australia, Spain, Argentina, France, and India) and in 2 US states (North Dakota and Minnesota). When choosing an antibiotic for postexposure prophylaxis, clinicians should consider reports of local ciprofloxacin-resistant meningococci.
Vaccination
See Meningococcal Vaccine for more information, including indications, contraindications and precautions, dosing and administration, and adverse effects. See also the vaccine schedules for children and adults from the Centers for Disease Control and Prevention (CDC) and meningococcal vaccine recommendations from the Advisory Committee on Immunization Practices (ACIP).
There are several meningococcal vaccines:
Three quadrivalent conjugate vaccines (MenACWY-D, MenACWY-CRM, and MenACWY-TT) that protect against 4 of the 6 common pathogenic serogroups of meningococcus (all but B and X) are available.
A bivalent conjugate vaccine that protects against serogroups C and Y is available only in combination with tetanus toxoid and Haemophilus influenzae type b vaccine (Hib-MenCY-TT) is approved for children 6 weeks through 18 months of age at increased risk of meningococcal disease; however, Hib-MenCY-TT is no longer available in the US (1).
A quadrivalent polysaccharide vaccine (MPSV4) for use in selected patients ≥ 56 years is no longer available in the US.
Two monovalent vaccines that protect against serogroup B (MenB-4C and MenB-FHbp) are available.
All children should receive a quadrivalent conjugate vaccine at age 11 or 12 years, with a booster dose at age 16 years (see also the routine childhood vaccination schedule). These vaccines are also recommended for adults who are at increased risk.
MenB-4C or MenB-FHbp is recommended for people ≥ 10 years who are at increased risk of serogroup B meningococcal disease.
Prevention reference
1. Mbaeyi SA, Bozio CH, Duffy J, et al: Meningococcal vaccination: Recommendations of the Advisory Committee on Immunization Practices, United States, 2020. MMWR Recomm Rep 69(No. RR-9):1–41, 2020. doi: 10.15585/mmwr.rr6909a1
Key Points
Over 90% of meningococcal infections involve meningitis or meningococcemia.
An asymptomatic nasopharyngeal carrier state is common; transmission usually occurs via direct contact with respiratory secretions from a carrier.
In the US, most cases are sporadic, typically in children < 2 years of age, but outbreaks can occur, primarily in semiclosed communities (eg, military recruit camps, dormitories, day care centers) and often involve patients aged 16 to 23 years.
Give close contacts a prophylactic antibiotic.
Vaccinate all children starting at age 11 or 12 years, and selectively vaccinate high-risk younger children and other high-risk people.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Centers for Disease Control and Prevention (CDC): Vaccine schedule for children 18 years of age or younger
CDC: STI Treatment Guidelines 2021: Diseases Characterized by Urethritis and Cervicitis
Advisory Committee on Immunization Practices (ACIP): Meningococcal vaccine recommendations






