


Smallpox is a highly contagious disease caused by the smallpox virus, an orthopoxvirus. Case fatality rate is about 30%. Natural infection has been eradicated. The main concern for outbreaks is from bioterrorism. Severe constitutional symptoms and a characteristic pustular rash develop. Treatment is generally supportive and potentially with antiviral drugs. Prevention involves vaccination, which, because of its risks, is done selectively.
No cases of smallpox have occurred in the world since 1977 because of worldwide vaccination. In 1980, the World Health Organization (WHO) recommended discontinuation of routine smallpox vaccination. Routine vaccination in the United States ended in 1972. Because humans are the only natural host of the smallpox virus and because the virus cannot survive > 2 days in the environment, WHO has declared natural infection eradicated.
Concerns about bioterrorism using smallpox virus from retained research stores or even from synthetically created virus raise the possibility of a recurrence (see Biological Agents as Weapons and Centers for Disease Control and Prevention [CDC]: Smallpox/Bioterrorism).
Pathophysiology of Smallpox
There are at least 2 strains of smallpox virus:
Variola major (classic smallpox), the more virulent strain
Variola minor (alastrim), the less virulent strain
Smallpox is transmitted from person to person by inhalation of respiratory droplets or, less efficiently, by direct contact. Contaminated clothing or bed linens can also transmit infection. The infection is most communicable for the first 7 to 10 days after the rash appears. Once crusts form on the skin lesions, infectivity declines.
The attack rate is as high as 85% in unvaccinated people, and infection may lead to as many as 4 to 10 secondary cases from each primary case. However, infection tends to spread slowly and mainly among close contacts.
The virus invades the oropharyngeal or respiratory mucosa and multiplies in regional lymph nodes, causing subsequent viremia. It eventually localizes in small blood vessels of the dermis and the oropharyngeal mucosa. Other organs are seldom clinically involved, except for occasionally the central nervous system, with encephalitis. Secondary bacterial infection of the skin, lungs, and bones may develop.
Symptoms and Signs of Smallpox
Variola major
Variola major has a 10- to 12-day incubation period (range 7 to 17 days), followed by a 2- to 3-day prodrome of fever, headache, backache, and extreme malaise. Sometimes severe abdominal pain and vomiting occur. After the prodrome, maculopapular lesions develop on the oropharyngeal mucosa, face, and arms, spreading shortly thereafter to the trunk and legs. The oropharyngeal lesions quickly ulcerate. After 1 or 2 days, the cutaneous lesions become vesicular, then pustular. Pustules are denser on the face and extremities than on the trunk, and they may appear on the palms. The pustules are round and tense and appear deeply embedded. Skin lesions of smallpox, unlike those of chickenpox, are all at the same stage of development on a given body part. After 8 or 9 days, the pustules become crusted. Severe residual scarring is typical.
Case fatality rate is about 30%. Death results from a massive inflammatory response causing shock and multiple organ failure and usually occurs during the 2nd week of illness.
About 5 to 10% of people with variola major develop either a hemorrhagic or a malignant (flat) variant.
The hemorrhagic form is rarer and has a shorter, more intense prodrome, followed by generalized erythema and cutaneous and mucosal hemorrhage. It is uniformly fatal within 5 or 6 days.

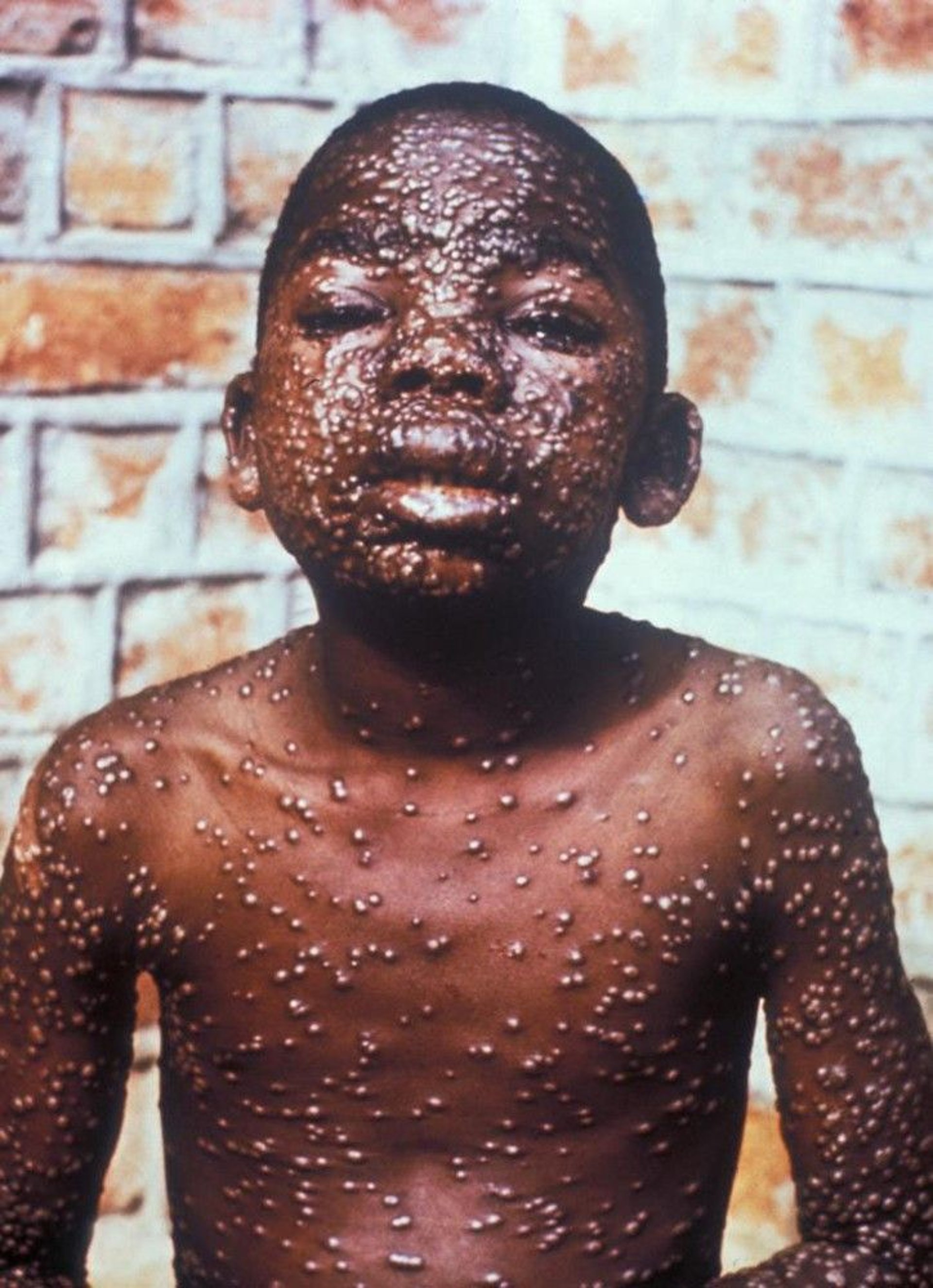
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
The malignant form has a similar, severe prodrome, followed by development of confluent, flat, nonpustular skin lesions. In survivors, the epidermis frequently desquamates.
Variola minor
Variola minor results in symptoms that are similar but much less severe, with a less extensive rash.
Case fatality rate is < 1%.
Diagnosis of Smallpox
Polymerase chain reaction (PCR)
Electron microscopy
Unless laboratory exposure is documented or an outbreak (due to bioterrorism) is suspected, only patients that fit the clinical case definition for smallpox should be tested because of the risk that test results may be falsely positive. An algorithm for evaluating the risk of smallpox in patients with fever and rash is available on the CDC web site (CDC Algorithm Poster for Evaluation of Suspected Smallpox).
Diagnosis of smallpox is confirmed by documenting the presence of variola DNA by PCR of vesicular or pustular samples. Or the virus can be identified by electron microscopy or viral culture of material scraped from skin lesions and subsequently confirmed by PCR. Suspected smallpox must be reported immediately to local public health agencies or the CDC at 770-488-7100. These agencies then arrange for testing in a laboratory with high-level containment capability (biosafety level 4).
Point-of-care antigen detection assays are being developed.
Treatment of Smallpox
Supportive care
Isolation
12, 3). (See also CDC: Smallpox Prevention and Treatment.)
Isolation of people with smallpox is essential. In limited outbreaks, patients may be isolated in a hospital under airborne transmission precautions in an airborne-infection isolation room. In mass outbreaks, home isolation may be required. Contacts should be placed under surveillance, typically with daily temperature measurement; if they develop a temperature of > 38° C or other sign of illness, they should be isolated at home.
Treatment references
1. Grosenbach DW, Honeychurch K, Rose EA, et al: Oral tecovirimat for the treatment of smallpox. N Engl J Med 5;379(1):44-53, 2018. doi: 10.1056/NEJMoa1705688
2. Chittick G, Morrison M, Brundage T, et al: Short-term clinical safety profile of brincidofovir: A favorable benefit-risk proposition in the treatment of smallpox. Antiviral Res 143:269–277, 2017. doi: 10.1016/j.antiviral.2017.01.009
3. Chan-Tack K, Harrington P, Bensman T, et al: Benefit-risk assessment for brincidofovir for the treatment of smallpox: U.S. Food and Drug Administration's Evaluation. Antiviral Res 195:105182, 2021. doi: 10.1016/j.antiviral.2021.105182. Epub 2021 Sep 25. PMID: 34582915.
Prevention of Smallpox
Licensed smallpox vaccines in the United States consist of ACAM2000, a live replication-competent vaccinia virus and JYNNEOS, a live attenuated (replication-deficient) modified vaccinia Ankara (MVA) vaccine (1). This attenuated (weakened) vaccine does not reproduce in the person who receives it. (See also CDC: Smallpox Vaccine Basics.)
Vaccinia virus is related to smallpox and provides cross-immunity. ACAM2000 vaccine is administered with a bifurcated needle dipped in reconstituted vaccine. The needle is rapidly jabbed 15 times in an area about 5 mm in diameter and with sufficient force to draw a trace of blood. The vaccine site is covered with a dressing to prevent spread of the vaccine virus to other body sites or to close contacts. Fever, malaise, and myalgias are common the week after vaccination. Successful vaccination is indicated by development of a pustule by about the 7th day. People without such signs of successful vaccination should be given another dose of vaccine.
Vaccination with ACAM2000 is dangerous and not recommended for some people, especially those with the following risk factors:
Weakened immune system (such as those who have AIDS or who take medications that suppress the immune system)
Skin disorders (particularly atopic dermatitis [eczema])
Eye inflammation
Heart condition
Age under 1 year
Pregnancy
JYNNEOS is administered as 2 subcutaneous injections 4 weeks apart. It is licensed by the FDA for people 18 years of age and older. The JYNNEOS vaccine may have a particular role in vaccinating people for whom ACAM2000 may be contraindicated, such as those with immunocompromised states or atopic dermatitis (see above list). However, people who have a weakened immune system may have a diminished response the JYNNEOS vaccine.
After a single vaccination, immunity begins to fade after 5 years and is probably negligible after 20 years. If people have been successfully revaccinated one or more times, some residual immunity may persist for ≥ 30 years.
Until an outbreak in the population occurs, preexposure vaccination remains recommended only for people at high risk of exposure to the virus (eg, laboratory technicians [2]).

Image courtesy of Dr. Allen W. Mathies of the Immunization Branch of the California Emergency Preparedness Office (Calif/EPO) via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Dr. Allen W. Mathies of the Immunization Branch of the California Emergency Preparedness Office (Calif/EPO) via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Arthur E. Kaye via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Dr. Allen W. Mathies of the Immunization Branch of the California Emergency Preparedness Office (Calif/EPO) via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Dr. Allen W. Mathies of the Immunization Branch of the California Emergency Preparedness Office (Calif/EPO) via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Dr. Allen W. Mathies of the Immunization Branch of the California Emergency Preparedness Office (Calif/EPO) via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Arthur E. Kaye via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Dr. Allen W. Mathies of the Immunization Branch of the California Emergency Preparedness Office (Calif/EPO) via the Public Health Image Library of the Centers for Disease Control and Prevention.
Live vaccinia virus vaccine complications
Risk factors for complications of the replication-competent virus vaccine (ACAM2000) include extensive skin disorders (particularly eczema), immunosuppressive diseases or therapies, ocular inflammation, pregnancy, heart conditions, and age under 1 year. Widespread vaccination is not recommended because of the risk.
Serious complications occur in about 1 of 10,000 patients after their first (primary) vaccination and include
Postvaccinial encephalitis
Progressive vaccinia
Eczema vaccinatum
Generalized vaccinia
Myocarditis and/or pericarditis
Vaccinia virus keratitis
Noninfectious rashes
Postvaccinial encephalitis occurs in about 1 of 300,000 recipients of primary vaccination, typically 8 to 15 days postvaccination.
Progressive vaccinia (vaccinia necrosum) results in a nonhealing vaccinial (vesicular) skin lesion that spreads to adjacent skin and ultimately other skin areas, bones, and viscera. Progressive vaccinia may occur after primary vaccination or revaccination but occurs almost exclusively in patients with an underlying defect in cell-mediated immunity; it can be fatal.
Eczema vaccinatum results in vaccinial skin lesions appearing on areas of active or even healed eczema.
Generalized vaccinia results from hematogenous dissemination of the vaccinia virus and causes vaccinia lesions at multiple body locations; it is usually benign.
Vaccinia virus keratitis occurs rarely, when vaccinia virus is inadvertently implanted in the eye.
Postexposure prophylaxis
Postexposure vaccination with a replication-competent vaccine can prevent or significantly limit the severity of illness and is indicated for family members and close personal contacts of smallpox patients. Early administration is most effective, but some benefit is realized up to 7 days postexposure.
Prevention references
1. Pittman PR, Hahn M, Lee HS, et al: Phase 3 efficacy trial of modified vaccinia ankara as a vaccine against smallpox. N Engl J Med 381(20):1897-1908, 2019. doi: 10.1056/NEJMoa1817307
2. Petersen BW, Harms TJ, Reynolds MG, et alMMWR Morb Mortal Wkly Rep 65 (10):257–262, 2016. doi: 10.15585/mmwr.mm6510a2
Key Points
No cases of smallpox have occurred since 1977, but concerns about possible use for bioterrorism remain.
Diagnosis is made by PCR.
Vaccination is highly protective, but rare complications from replication-competent virus vaccine (about 1:10,000) can be serious.
Immunity fades over decades.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Centers for Disease Control and Prevention (CDC): Smallpox Vaccination: Information for Health Care Providers






