


Plague is caused by the gram-negative bacterium Yersinia pestis
Yersinia (formerly Pasteurella) pestis is a short bacillus that often shows bipolar staining (especially with Giemsa stain) and may resemble a safety pin.
Massive human epidemics (eg, the Black Death of the Middle Ages, an epidemic in Manchuria in 1911) have occurred.
More recently, plague has occurred sporadically or in limited outbreaks.
In the US, the last urban outbreak of rat-associated plague occurred in Los Angeles in 1924 to 1925. Since that time, > 90% of human plague in the US has occurred in rural or semirural areas of the Southwest, especially New Mexico, Arizona, California, and Colorado.
Worldwide, most cases since the 1990s have occurred in Africa; the Democratic Republic of Congo and Madagascar are most endemic. Peru is also one of the most endemic countries. In the last 20 years, almost all of the cases occurred among people living in small towns and villages or agricultural areas rather than in larger towns and cities.
Transmission
Plague occurs primarily in wild rodents (eg, rats, mice, squirrels, prairie dogs) and is transmitted from rodent to human by the bite of an infected rat flea vector. Plague may also be spread through contact with fluid or tissue from an infected animal.
Human-to-human transmission occurs by inhaling droplets from patients with pulmonary infection (primary pneumonic plague), which is highly contagious.
In endemic areas in the US, several cases may have been caused by household pets, especially cats (infected by eating infected rodents). Transmission from cats can be by bite of an infected flea or, if the cat has pneumonic plague, by inhalation of infected respiratory droplets.
Pneumonic plague can also be transmitted via exposure in a laboratory or intentional aerosol spread as an act of bioterrorism.
Symptoms and Signs of Plague
Plague has several distinct clinical manifestations:
Bubonic plague (most common)
Pneumonic plague (primary or secondary)
Septicemic plague
Pestis minor
Pharyngeal plague and plague meningitis are less common forms.
Bubonic plague
In bubonic plague, the most common form, the incubation period is usually 2 to 5 days but varies from a few hours to 12 days.
Onset of fever of 39.5 to 41° C is abrupt, often with chills. The pulse may be rapid and thready; hypotension may occur.
Lymph nodes that drain the site of inoculation by the bacteria become enlarged and tender (buboes) and appear shortly after the fever. The femoral or inguinal lymph nodes are most commonly involved, followed by axillary, cervical, or multiple nodes. Typically, the nodes are extremely tender and firm, surrounded by considerable edema. They may suppurate in the 2nd week. The overlying skin is smooth and reddened but often not warm.
A primary cutaneous lesion (papule, pustule, ulcer, or eschar) may form at the site of the flea bite.
The patient may be restless, delirious, confused, and uncoordinated. The liver and spleen may be enlarged.
Because the bacteria can spread through the bloodstream to other parts of the body, bubonic plague may be complicated by hematogenous (secondary) pneumonic plague.
The case fatality rate for untreated patients with bubonic plague is about 60%; most deaths result from septicemia in 3 to 5 days.

Image courtesy of Drs. Margaret Parsons and Karl F. Meyer via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Drs. Margaret Parsons and Karl F. Meyer via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Drs. Margaret Parsons and Karl F. Meyer via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Drs. Margaret Parsons and Karl F. Meyer via the Public Health Image Library of the Centers for Disease Control and Prevention.
Pneumonic plague
Primary pneumonic plague has a 2- to 3-day incubation period, followed by abrupt onset of high fever, chills, tachycardia, chest pain, and headache, often severe. Cough, not prominent initially, develops within 24 hours. Sputum is mucoid at first, rapidly develops blood specks, and then becomes uniformly pink or bright red (resembling raspberry syrup) and foamy. Tachypnea and dyspnea are present, but pleuritic chest pain is not. Signs of consolidation are rare, and rales may be absent.
Secondary pneumonic plague is more common than primary and results from hematogenous dissemination of organisms from a bubo or other foci of infection.
Most untreated patients with pneumonic plague die within 48 hours of symptom onset.
Septicemic plague
Septicemic plague may occur with the bubonic form or without the bubonic form (called primary septicemic plague) as an acute, fulminant illness.
Abdominal pain, presumably due to mesenteric lymphadenopathy, occurs in 40% of patients. Disseminated intravascular coagulopathy, gangrene of the extremities (hence, the name Black Death), and multiorgan failure eventually develop.
Septicemic plague may be fatal before bubonic or pulmonary manifestations predominate.
Pestis minor
Pestis minor, a more benign form of bubonic plague, usually occurs only in endemic areas. Lymphadenitis, fever, headache, and prostration subside within a week.
Diagnosis of Plague
Staining, cultures, and serologic and polymerase chain reaction (PCR) testing
Rapid diagnosis of plague is important because mortality increases significantly the longer treatment is delayed.
Diagnosis is made by stain and culture of the organism, typically by needle aspiration of a bubo (surgical drainage may disseminate the organism); blood and sputum cultures should also be obtained.
Other tests include immunofluorescent staining and serology; a titer of > 1:16 or a 4-fold rise between acute and convalescent titers is positive. PCR testing, if available, is diagnostic.
Prior vaccination does not exclude plague; clinical illness may occur in vaccinated people.

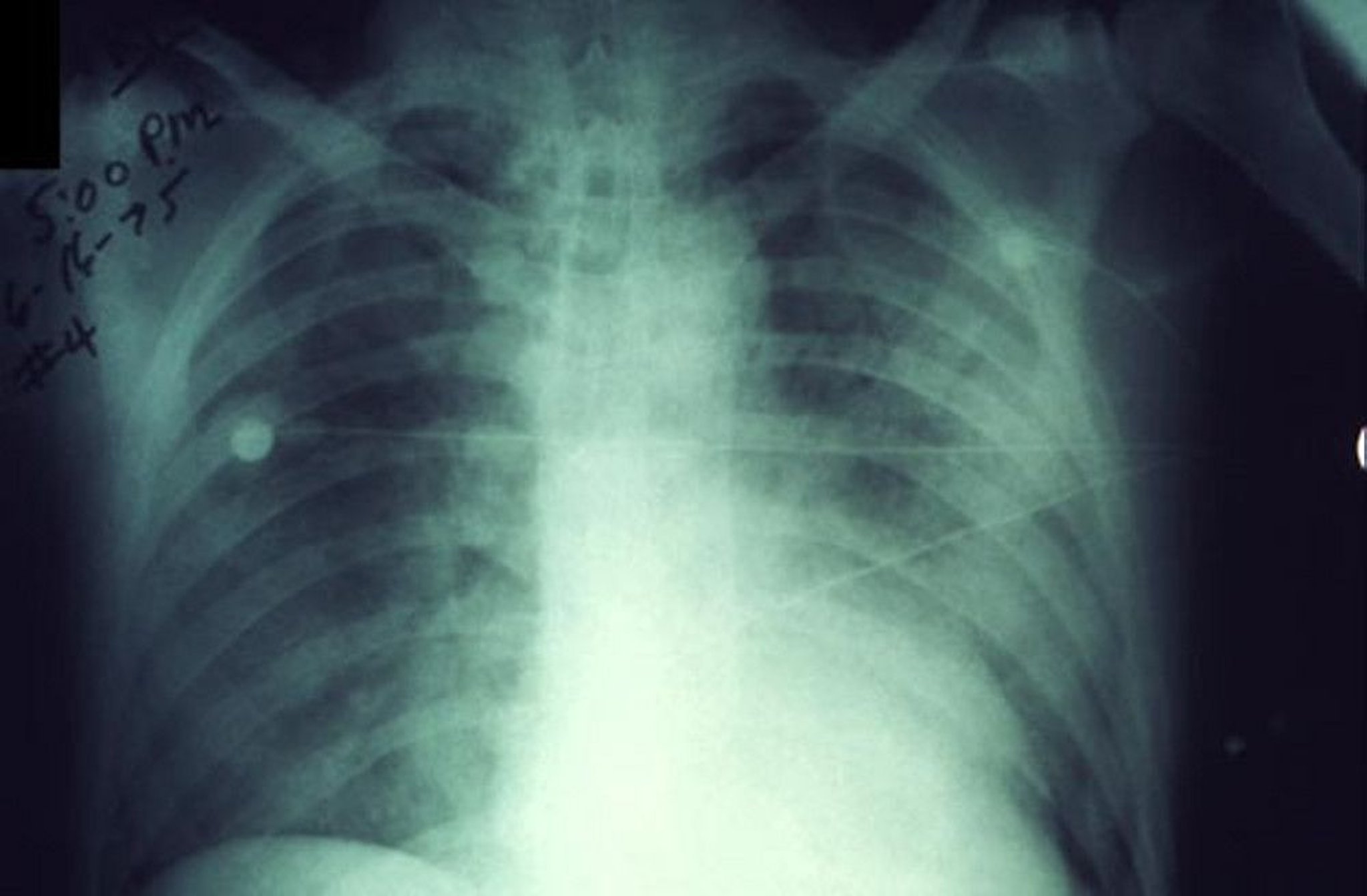
Image courtesy of Dr. Jack Poland via the Public Health Image Library of the Centers for Disease Control and Prevention.
Patients with pulmonary symptoms or signs should have a chest x-ray, which shows a rapidly progressing pneumonia in pneumonic plague. The white blood cell count is usually 10,000 to 20,000/mcL (10 to 20 × 109/L) with numerous immature neutrophils.
Treatment of Plague
Before antibiotics (1900–1941), case fatality among those infected with plague in the US was 66%. By 1990–2010, antibiotic treatment of plague reduced case fatality to 11% (1).
In septicemic or pneumonic plague, treatment must begin within 24 hours with one of the following if renal function is normal (2; see also the Centers for Disease Control and Prevention's [CDC] Resources for Clinicians):
Routine isolation precautions are adequate for patients with bubonic plague. Those with primary or secondary pneumonic plague require strict respiratory isolation and droplet precautions (see the Centers for Disease Control and Prevention's 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings).
Treatment references
1. CDC: What is the death rate of plague? Accessed 03/14/2022.
2. Nelson CA, Meaney-Delman D, Fleck-Derderian S, et al: Antimicrobial treatment and prophylaxis of plague: Recommendations for naturally acquired infections and bioterrorism response. MMWR Recomm Rep 70(3);1–27, 2021. doi: 10.15585/mmwr.rr7003a1
Prevention of Plague
All pneumonic plague contacts should be under medical surveillance. Temperature should be taken every 4 hours for 6 days. They and others in close contact with patients who have plague pneumonia or in direct contact with infected body fluids or tissues should receive oral prophylaxis for 7 days with
Plague vaccines (killed whole-cell and live-attenuated) are no longer available in the US.
Rodents should be controlled and repellents used to minimize flea bites.
Key Points
Plague is a highly contagious, life-threatening infection now present in the US mainly in rural or semirural areas of the Southwest; worldwide, most cases since the 1990s have occurred in Africa.
Plague may cause large, tender, often suppurative lymphadenopathy (buboes), severe pulmonary infection, and/or septicemia.
Rapid diagnosis using stain and culture of the organism is important because mortality increases significantly the longer treatment is delayed.
Place patients with pneumonic plague in strict respiratory isolation; routine isolation is adequate for those with other forms.
More Information
The following are English-language resources that may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Centers for Disease Control and Prevention (CDC):Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings (2007)
Other Yersinia Infections
Yersinia enterocolitica and Y. pseudotuberculosis are zoonoses that occur worldwide and are acquired by ingestion or handling of contaminated food (most commonly raw or undercooked pork products and unpasteurized milk or milk products) or water and occasionally by animal contact.
Y. enterocolitica is a common cause of diarrheal disease and mesenteric adenitis that clinically mimics appendicitis. Y. pseudotuberculosis most commonly causes mesenteric adenitis and has been suspected in cases of interstitial nephritis, hemolytic-uremic syndrome, and a scarlet fever–like illness. Both species can cause pharyngitis, septicemia, focal infections in multiple organs, and postinfectious erythema nodosum and reactive arthritis. In patients with chronic liver disease or iron overload, case fatality from septicemia may be as high as 50%, even with treatment.
The organisms can be identified in standard cultures from normally sterile sites. Selective culture methods are required for nonsterile specimens, such as stool culture for diarrheal disease. It is important to notify the laboratory when Yersinia infection is suspected in stool so that a special culture medium can be used. Serologic assays are available but difficult and not standardized. Diagnosis, particularly of reactive arthritis, requires a high index of suspicion and close communication with the clinical laboratory.
Treatment
Prevention is focused on food handling and preparation, household pets, and epidemiology of suspected outbreaks.






