


Most hip dislocations are posterior and result from severe posteriorly directed force to the knee while the knee and hip are flexed (eg, against a car dashboard).
Complications may include
Sciatic nerve injury
Delayed osteonecrosis of the femoral head
Associated injuries include
In patients with posterior dislocations, the leg is shortened, adducted, and internally rotated. Anterior dislocations are rare and result in the leg being abducted and externally rotated.
(See Overview of Dislocations.)
Diagnosis of Hip Dislocations
X-rays
Routine hip x-rays are diagnostic.

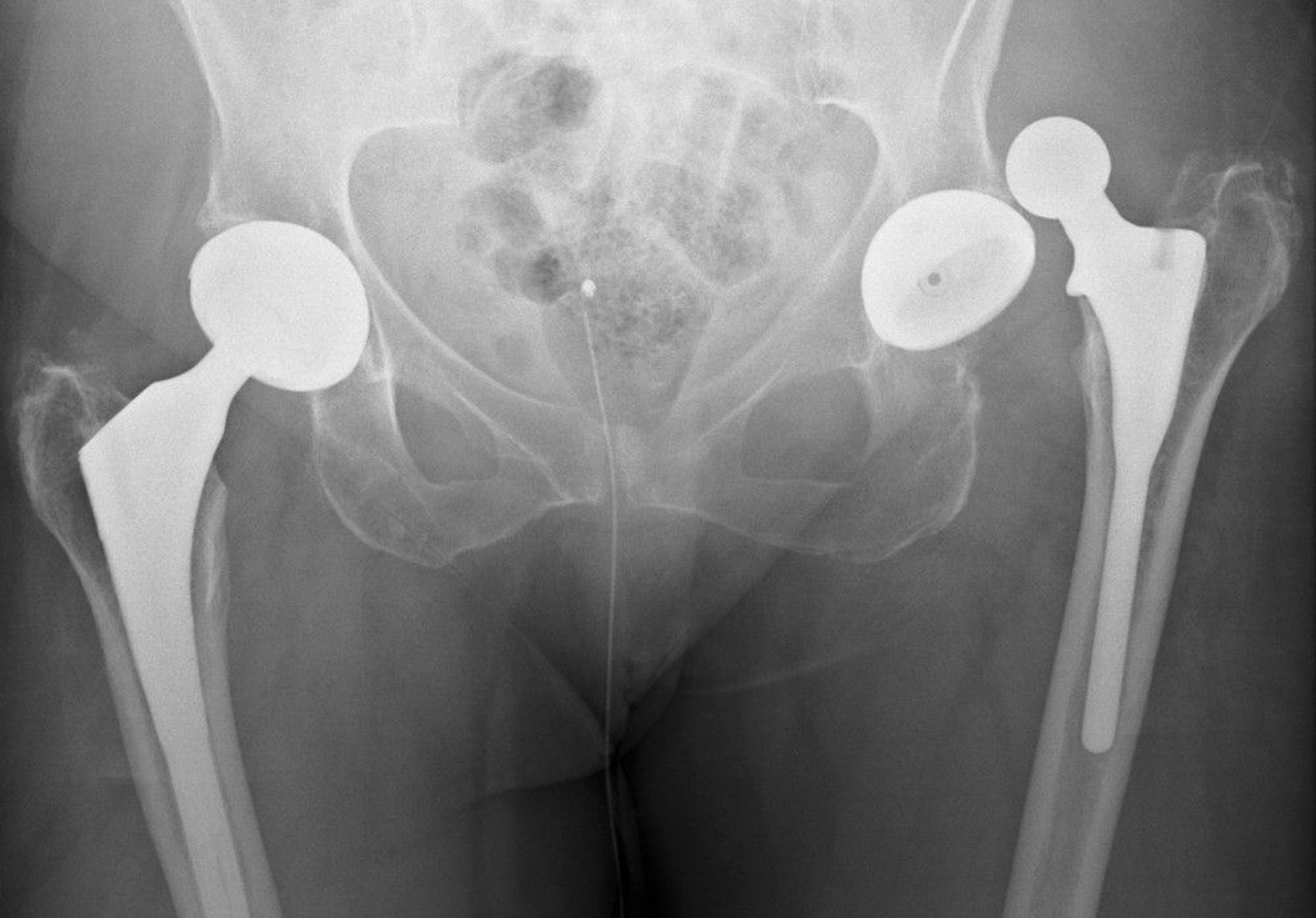
DU CANE MEDICAL IMAGING LTD/SCIENCE PHOTO LIBRARY
Treatment of Hip Dislocations
Closed reduction
Treatment of hip dislocations is closed reduction as soon as possible, preferably in ≤ 6 hours; delay increases the risk of osteonecrosis (1).
The hip can be reduced using one of the following techniques:
Allis technique
Captain Morgan technique
Rocket launcher technique
When any of these techniques is used, the patient requires sedation and muscle relaxation and is in the supine position. (See also How To Reduce a Posterior Hip Dislocation.)
For the Allis technique, the hip is gently flexed to 90°, and vertical traction is applied to the femur; this maneuver may be easiest and safest when the patient is temporarily placed on a rigid backboard that is put on the floor. A strap or brace is used to hold down the patient's hips (providing counterpressure to the vertical traction of the femur).
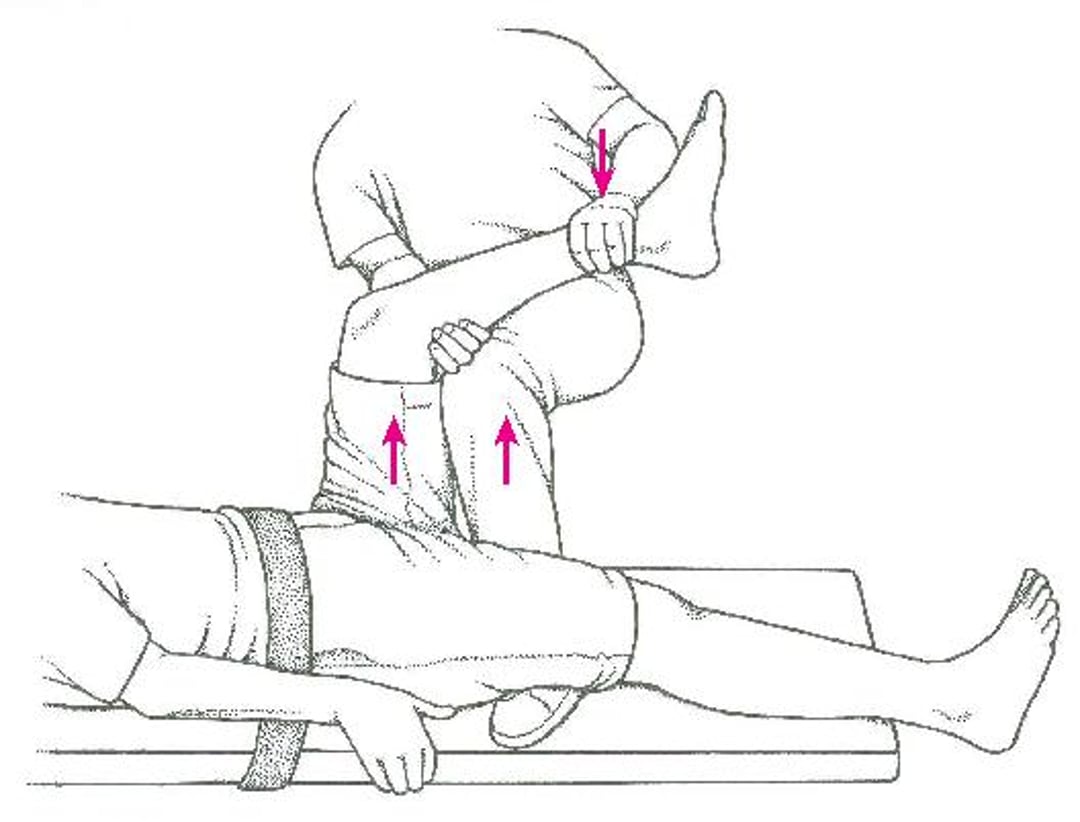
For the Captain Morgan technique, the patient's hips are held down by a sheet or belt, and the dislocated hip is flexed. Practitioners then place their knee under the patient's knee and lift up while applying vertical traction to the femur. The Captain Morgan technique may have a better first-time success rate than the Allis technique (2).
Captain Morgan technique

For the rocket launcher technique (3), the practitioner stands on the side of the affected hip and faces the patient's feet. The dislocated hip and knee are flexed to 90°. The patient's hips are held down by a sheet or by a second practitioner (to provide countertraction to the pelvis). The practitioner squats, and the patient's knee is placed on the practitioner's shoulder; the practitioner essentially holds the leg like a rocket launcher. The patient's hip is adducted by pressing inward on the knee and is internally rotated by turning the foot out; the practitioner then gently applies traction to the femur by standing from the squat and pulling down on the patient's foot, using the practitioner's shoulder as a fulcrum.


Image courtesy of Danielle Campagne, MD.
After reduction, CT is needed in all native hips to identify acetabular and femoral head fractures and intra-articular debris or loose bodies (bone or cartilage fragments). About 70% of patients with posterior dislocation of the hip have a concomitant acetabular fracture (4). If fractures or loose bodies are found, an orthopedist should be consulted about possible surgical intervention. If CT does not show any fractures or loose bodies, patients are sent home with crutches and told that their foot may touch the floor (eg, to maintain balance) but they should not put any weight on it (toe-touch weight bearing), at least until they are given permission to do so after orthopedic follow-up.
Treatment references
1. Kellam P, Ostrum RF: Systematic review and meta-analysis of avascular necrosis and posttraumatic arthritis after traumatic hip dislocation. J Orthop Trauma 30 (1):10–16, 2016. doi: 10.1097/BOT.0000000000000419
2. Hendey GW, Avila A: The Captain Morgan technique for the reduction of the dislocated hip. Ann Emerg Med 58 (6):536–540, 2011. doi: 10.1016/j.annemergmed.2011.07.010
3. Dan M, Phillips A, Simonian M, et al: Rocket launcher: A novel reduction technique for posterior hip dislocations and review of current literature. Emerg Med Australas 27 (3):192–195, 2015. doi: 10.1111/1742-6723.12392
4. Hak DJ, Goulet JA: Severity of injuries associated with traumatic hip dislocation as a result of motor vehicle collisions. J Trauma 47(1):60–63, 1999. doi: 10.1097/00005373-199907000-00014
Dislocated prosthetic hip
After total hip replacement, the prosthetic hip dislocates without trauma in up to 2% of patients. Posterior dislocations are more common.
Closed reduction is often successful, particularly for first-time dislocations, but hip revision surgery is sometimes required.
Key Points
Most hip dislocations are posterior, causing the leg to be shortened, adducted, and internally rotated.
Diagnose using routine x-rays.
Reduce as soon as possible, preferably in ≤ 6 hours, using one of several techniques; delay increases the risk of osteonecrosis.
After reduction, do CT to check for fractures and intra-articular debris or loose bone fragments.






