


Burns are injuries of skin or other tissue caused by thermal, radiation, chemical, or electrical contact. Burns are classified by depth (superficial and deep partial-thickness, and full-thickness) and percentage of total body surface area (TBSA) involved. Complications and associated problems include hypovolemic shock, inhalation injury, infection, scarring, and contractures. Patients with large burns ( 20% TBSA) require fluid resuscitation. Treatments for burn wounds include topical antibacterials, regular cleansing, elevation, and sometimes skin grafting. Intensive rehabilitation, consisting of range-of-motion exercises and splinting, is often necessary.
Burns cause about 3000 deaths/year in the US and about 2 million physician visits.
(See also Ocular Burns and Caustic Ingestion.)
Etiology of Burns
Thermal burns may result from any external heat source (flame, hot liquids, hot solid objects, or occasionally, steam). Fires may also result in toxic smoke inhalation (see also Carbon Monoxide Poisoning).
Pearls & Pitfalls
|
Radiation burns most commonly result from prolonged exposure to solar ultraviolet radiation (sunburn) but may result from prolonged or intense exposure to other sources of ultraviolet radiation (eg, tanning beds) or from exposure to sources of x-ray or other nonsolar radiation (see Radiation Exposure and Contamination).
Chemical burns may result from strong acids, strong alkalis (eg, lye, cement), phenols, cresols, mustard gas, phosphorus, and certain petroleum products (eg, gasoline, paint thinner). Skin and deeper tissue necrosis caused by these agents may progress over several hours.
Electrical burns result from heat generation and electroporation of cell membranes associated with massive currents of electrons. High voltage (> 1000 volts) electrical burns often cause extensive deep tissue damage to electrically conductive tissues, such as muscles, nerves, and blood vessels, despite minimal apparent cutaneous injury.
Events associated with a burn (eg, jumping from a burning building, being struck by debris, motor vehicle crash) may cause other injuries. Abuse should be considered in young children and older patients with burns (see Child Maltreatment and Elder Abuse).
Pathophysiology of Burns
Heat from burns causes protein denaturation and thus coagulative necrosis. Around the coagulated tissue, platelets aggregate, vessels constrict, and marginally perfused tissue (known as the zone of stasis) can extend around the injury. In the zone of stasis, tissue is hyperemic and inflamed.
Damage to the normal epidermal barrier allows
Bacterial invasion
External fluid loss
Impaired thermoregulation
Damaged tissues often become edematous, further enhancing intravascular volume loss. Heat loss can be significant because thermoregulation of the damaged dermis is absent, particularly in wounds that are exposed.
Burn depth
Superficial (formerly 1st-degree) burns are limited to the epidermis.
Partial-thickness (formerly 2nd-degree) burns involve part of the dermis and can be superficial or deep.
Superficial partial-thickness burns involve the papillary (more superficial) dermis. These burns heal within 1 to 2 weeks, and scarring is usually minimal. Healing occurs from epidermal cells lining sweat gland ducts and hair follicles; these cells grow to the surface, then migrate across the surface to meet cells from neighboring glands and follicles.
Deep partial-thickness burns involve the deeper dermis and take ≥ 2 weeks to heal. Healing occurs only from hair follicles, and scarring is common and may be severe.


© Springer Science+Business Media
Full-thickness (formerly 3rd-degree) burns extend through the entire dermis and into the underlying fat. Healing occurs only from the periphery; these burns, unless small, require excision and skin grafting.
Complications of Burns
Burns cause both systemic and local complications. The major factors contributing to systemic complications are breakdown of skin integrity and fluid loss. Local complications include eschars and contractures and scarring.
Systemic burn complications
The greater the percentage of total body surface area (TBSA) involved, the greater the risk of developing systemic complications. Risk factors for severe systemic complications and mortality include all of the following:
Partial and full-thickness burns of ≥ 40% of TBSA
Age > 60 years or < 2 years
Presence of simultaneous major trauma or smoke inhalation
The most common systemic complications are hypovolemia and infection.
Hypovolemia, causing hypoperfusion of burned tissue and sometimes shock, can result from fluid losses due to burns that are deep or that involve large parts of the body surface; whole-body edema from escape of intravascular volume into the interstitium and cells also develops. Also, insensible fluid losses can be significant. Hypoperfusion of burned tissue also may result from direct damage to blood vessels or from vasoconstriction secondary to hypovolemia.
Infection, even in small burns, is a common cause of sepsis and mortality, as well as local complications. Impaired host defenses and devitalized tissue enhance bacterial invasion and growth. The most common pathogens are streptococci and staphylococci during the first few days and gram-negative bacteria after 5 to 7 days; however, flora are almost always mixed.
Metabolic abnormalities may include hypoalbuminemia that is partly due to hemodilution (secondary to replacement fluids) and partly due to protein loss into the extravascular space through damaged capillaries. Dilutional electrolyte deficiencies can develop; they include hypomagnesemia, hypophosphatemia, and hypokalemia. Metabolic acidosis may result from shock. Rhabdomyolysis or hemolysis can result from deep thermal or electrical burns of muscle or from muscle ischemia due to constricting eschars. Rhabdomyolysis causing myoglobinuria or hemolysis causing hemoglobinuria can lead to acute tubular necrosis and acute kidney injury.
Hypothermia may result from large volumes of cool IV fluids and extensive exposure of body surfaces to a cool emergency department environment, particularly in patients with extensive burns.
Ileus is common after extensive burns.
Local burn complications
Eschar is stiff, dead tissue caused by deep burns. A circumferential eschar, which completely encircles a limb (or sometimes the neck or torso), is potentially constricting. A constricting eschar limits tissue expansion in response to edema; instead, tissue pressure increases, eventually causing local ischemia. The ischemia threatens viability of limbs and digits distal to the eschar, and an eschar around the neck or thorax can compromise ventilation.
Scarring and contractures result from healing of deep burns. Depending on the extent of the scar, contracture deformities can appear at the joints. If the burn is located near joints (particularly in the hands), in the feet, or in the perineum, function can be severely impaired. Infection can increase scarring. Keloids form in some patients with burns, especially in patients with darker skin.
Symptoms and Signs of Burns


Image provided by Steven E. Wolf, MD.


Image provided by Steven E. Wolf, MD.
Wound symptoms and signs depend on burn depth:
Superficial burns: These burns are red, blanch markedly and widely with light pressure, and are painful and tender. Vesicles or bullae do not develop.
Superficial partial-thickness burns: These burns blanch with pressure and are painful and tender. Vesicles or bullae develop within 24 hours. The bases of vesicles and bullae are pink and subsequently develop a fibrinous exudate.
Deep partial-thickness burns: These burns may be white, red, or mottled red and white. They do not blanch and are less painful and tender than more superficial burns. A pinprick is often interpreted as pressure rather than sharp. Vesicles or bullae may develop; these burns are usually dry.
Full-thickness burns: These burns may be white and pliable, black and charred, brown and leathery, or bright red because of fixed hemoglobin in the subdermal region. Pale full-thickness burns may simulate normal skin except the skin does not blanch to pressure. Full-thickness burns are usually anesthetic or hypoesthetic. Hairs can be pulled easily from their follicles. Vesicles and bullae usually do not develop. Sometimes features that differentiate full thickness from deep partial thickness burns take 24 to 48 hours to develop.
Diagnosis of Burns
Clinical assessment of burn extent and depth
Laboratory testing and chest x-ray in admitted patients
Location and depth of burned areas are recorded on a burn diagram. Burns with an appearance compatible with both deep partial-thickness and full-thickness are presumed to be full-thickness.
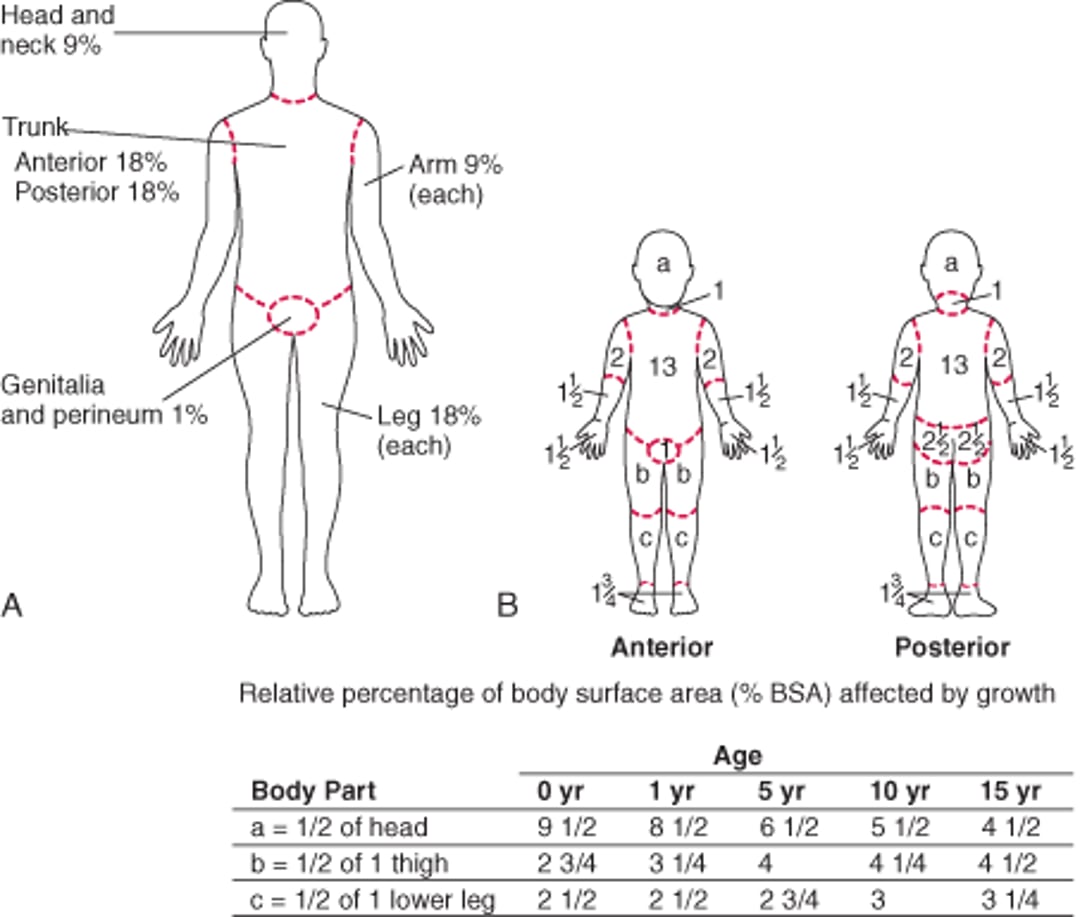
The percentage of TBSA involved is calculated; only partial-thickness and full-thickness burns are included in this calculation (1). For adults, the percentage TBSA for parts of the body is estimated by the rule of nines ([A] Rule of nines (for adults) and [B] Lund-Browder chart (for children) for estimating extent of burns); for smaller scattered burns, estimates can be based on the size of the patient’s entire opened hand (not the palm only), which is about 1% of TBSA. The hand size method is particularly helpful in calculating the burn surface area of a partially burned area. For example, if an arm (which would represent 9% if totally involved) is not completely burned, the patient's hand size can be used as a template to estimate the extent of scattered uninvolved (or involved) areas. The uninvolved area can be subtracted from the 9% area of the arm to more accurately calculate the burned surface area of the arm. Children have proportionally larger heads and smaller lower extremities, so the percentage TBSA is more accurately estimated using the Lund-Browder chart ([A] Rule of nines (for adults) and [B] Lund-Browder chart (for children) for estimating extent of burns).
(A) Rule of nines (for adults) and (B) Lund-Browder chart (for children) for estimating extent of burns
(Redrawn from Artz CP, JA Moncrief: The Treatment of Burns, ed. 2. Philadelphia, WB Saunders Company, 1969; used with permission.) |

Muscle compartments are evaluated in patients with myoglobinuria.
Burn infection is suggested by wound exudate, impaired wound healing, or systemic evidence of infection (eg, feeding intolerance, decrease in platelet count, increase in serum glucose level). Fever and white blood cell count elevation are common in burn patients without infection and therefore are unreliable signs of developing sepsis. If the diagnosis is unclear, infection can be confirmed by biopsy; cultures from the wound surface or exudate are unreliable. Many centers test patients on admission for colonization with methicillin-resistant Staphylococcus aureus (MRSA).
Diagnosis reference
1. Kamolz LP, Parvizi D, Giretzlehner M, et al: Burn surface area calculation: What do we need in future. Burns 40(1):171-172, 2014. doi: 10.1016/j.burns.2013.07.021
Treatment of Burns
IV fluids for partial and full thickness burns > 10% of total body surface area (TBSA)
Wound cleansing, dressing, and serial assessment
Supportive measures
Transfer or referral of selected patients to burn centers
Surgery and physical therapy for deep partial-thickness and full-thickness burns
Initial treatment
Treatment begins in the prehospital setting. The first priorities are the same as for any injured patient: ABC (airway, breathing, and circulation). An airway is provided, ventilation is supported, and possible associated smoke inhalation is treated with 100% oxygen. Ongoing burning is extinguished, and smoldering and hot material is removed. All clothing is removed. Chemicals, except powders, are flushed with water; powders should be brushed off before wetting. Burns caused by acids, alkalis, or organic compounds (eg, phenols, cresols, petrochemicals) are flushed with copious amounts of water continuing for at least 20 min after nothing of the original solution seems to remain.
Intravenous fluids
IV fluids are given to patients in shock or with partial and full thickness burns > 10% TBSA. A 14- to 16-gauge venous cannula is placed in 1 or 2 peripheral veins through unburned skin if possible. Venous cutdown, which has a high risk of infection, is avoided.
Initial fluid volume is guided by treatment of clinically evident shock (1). If shock is absent, fluid administration aims to replace the predicted deficit and supply maintenance fluids. The Parkland formula (4 mL/kg) × % TBSA burned (partial and full thickness burns) is used to estimate fluid volume needs in the first 24 hours after the burn (not after presentation to the hospital) and determines the rate of IV fluid administration. Half the calculated amount is given over the first 8 hours; the remainder is given over the next 16 hours. Fluid is given as lactated Ringer's solution because large amounts of normal saline could result in hyperchloremic acidosis.
For example, in a 100-kg man with a 50% TBSA burn, fluid volume by the Parkland formula would be


Half of the volume, 10 L, is given in the first 8 hours after injury as a constant infusion, and the remaining 10 L is given over the following 16 hours. In practice, this formula is only a starting point, and infusion rates are adjusted based on clinical response. Urine output, typically measured with an indwelling catheter, is the usual indicator of clinical response; the goal is to maintain output of 0.5 mL/kg/hr in adults and 1.0 mL/kg/hour in children (< 30 kg). Additional pediatric maintenance fluid requirements should be calculated and added separately because children are at risk of hypoglycemia in high volume resuscitation. When giving typical large volumes of fluid, it is also important to avoid fluid overload and consequent heart failure and compartment syndrome. Fluid administration can be titrated to achieve only the goal urine output. Clinical parameters, including urine output and signs of shock or heart failure, are recorded at least hourly on a flow chart.
Pearls & Pitfalls
|
2, 3, 4).
For patients with rhabdomyolysis
Initial wound care
After adequate analgesia, the wound is cleansed with soap and water, and all loose debris is removed. Water should be room temperature or warmer to avoid inducing hypothermia. Ruptured blisters, except for small ones on palms, fingers, and soles, are debrided. Unruptured blisters can sometimes be left intact but should be treated by application of a topical antimicrobial. In patients who are to be transferred to a burn center, clean dry dressings can be applied (burn creams may interfere with burn wound assessment at the receiving facility), and patients are kept warm and relatively comfortable with IV opioids.
After the wound is cleansed and is assessed by the final treatment provider, burns can be treated topically. For shallow partial-thickness burns, topical treatment alone is usually adequate. All deep partial-thickness burns and full-thickness burns should ultimately be treated with excision and grafting, but in the interim, topical treatments are appropriate.
Topical treatment may be with
Commercial dressings incorporating silver (eg, sustained-release nanocrystalline silver dressings)
Biosynthetic wound dressings (also called artificial skin products)
Topical salves must be changed daily. Artificial skin products and silver impregnated dressings are not changed routinely but can result in underlying purulence necessitating removal, particularly when wounds are deep. Burned extremities should be elevated. Compression dressings such as elastic wraps should be used to reduce edema and improve wound healing.
A tetanus toxoid boosterPrevention of Tetanus).
Escharotomy (incision of the eschar) of constricting eschars may be necessary to allow adequate expansion of the thorax or perfusion of an extremity. However, constricting eschars rarely threaten extremity viability during the first few hours, so if transfer to a burn center can occur within that time, escharotomy can typically be deferred until then. If timely transfer is not possible, escharotomy should be done with the input of a consulting burn center.
Supportive measures
Nutritional support is indicated for patients with burns > 20% TBSA or preexisting undernutrition. Support with a feeding tube begins as soon as possible if oral nutrition is not feasible or adequate. Parenteral support is rarely necessary.
Hospitalization and referral
After initial treatment and stabilization, the need for transfer and/or hospitalization is assessed. Consultation with a burn center to discuss treatment options is strongly suggested for
Full-thickness burns > 1% TBSA
Partial-thickness burns > 5% TBSA
Burns of the hands, face, feet, or perineum (partial-thickness or deeper)
Because of the many factors involved in burn outcome, early discussion of the specifics of each case with a burn center is probably more helpful than applying rigid criteria without consultation.
In addition, transfer and/or hospitalization may be necessary if
Patients are < 2 years or > 60 years.
Adherence to home care measures is likely to be poor or difficult (eg, if continuous elevation of the hands or feet, usually difficult at home, is required).
Many experts recommend that all burns, except for superficial burns < 1% TBSA, be treated by experienced physicians and that urgent burn center follow-up treatments be strongly considered for all partial or full-thickness burns > 2% TBSA. Maintaining adequate analgesia and exercise can be difficult for many patients and caregivers. Even patients who are not treated as inpatients can benefit from transferral or early referral to a burn center so that wound care, specialized dressings, and early range-of-motion exercises can be initiated.
Infection
Prophylactic systemic antibiotics are not given.
Surgery
Surgery is indicated for burns that are not expected to heal within 2 weeks, including most deep partial-thickness burns and all full-thickness burns. Eschars are removed as soon as possible, ideally within 3 days to prevent sepsis and facilitate early wound grafting, which shortens hospitalization and improves the functional result. If burns are extensive and life threatening, the largest eschars are removed first to close as much burn area as early as possible. (See also How To Do Burn Escharotomy.)
After excision, grafting proceeds ideally using partial-thickness autografts (the patient’s skin), which are permanent (5). Autografts can be transplanted as sheets (solid pieces of skin) or meshed grafts (sheets of donor skin that are stretched to cover a larger area by making multiple, regularly spaced, small incisions). Meshed grafts are used in areas where appearance is less of a concern when burns are > 20% TBSA and donor skin is scarce. Meshed grafts heal with an uneven gridlike appearance, sometimes with excessive hypertrophic scarring.
When burns are > 40% TBSA and the supply of autograft material appears insufficient, an artificial dermal regeneration template can be used as temporary coverage (5). Allografts (viable skin usually from cadaver donors) or xenografts (eg, pig skin) can also be used temporarily; they are rejected, sometimes within 10 to 14 days. Both types of temporary coverage must ultimately be replaced with autografts.
Fasciotomy is done when edema within a muscle compartment elevates compartment pressure > 30 mm Hg. Compartment syndrome is rare in burns other than high voltage electrical burns (6).
Physical and occupational therapy
Physical and occupational therapy are begun at admission to help minimize scarring and contractures, particularly for body surfaces with high skin tension and frequent movement (eg, face, hands), and to optimize function. Active and passive range-of-motion exercises become easier as the initial edema subsides (enhanced by appropriate elevation and compression); they are done once or twice daily. After grafting, exercises are often suspended for 3 days, then resumed, but at some centers are initiated within 24 hours of grafting. Extremities affected by deep partial-thickness burns or full-thickness burns are splinted in functional positions as soon as possible and kept splinted continuously (except during exercise) until the graft has been placed, healing has occurred, or both.
Outpatient burn treatment
Outpatient treatment includes keeping burns clean and, to the extent possible, keeping the affected body part elevated and, for extremities, compressed (eg, by elastic wraps over dressings). Dressings should be changed daily for burns treated with topical salves. The salve is applied and then covered with a dry nonadherent gauze dressing and compression wraps. Silver dressings should be changed every 7 to 10 days, depending on the specific product recommendation. Dressing change simply involves removing the older dressing and replacing it with a new one. Biosynthetic wound dressings should not be changed in the absence of purulence. Biosynthetic dressings should simply be covered with dry gauze, which is changed daily. (See also How To Debride and Dress a Burn.)
Outpatient follow-up visits are scheduled as needed depending on burn severity (eg, for very minor burns, initial visit within 24 hours, then subsequent visits every 7 to 10 days). Visits include debridement if indicated, reassessment of burn depth, and evaluation of the need for physical therapy and grafting. Patients should return earlier if they note signs of infection, such as increasing redness extending from the wound edges, increasing purulence and pain, or a change in the appearance of the wound with development of black or red spots. Should these signs occur, medical evaluation should ensue urgently. Outpatient treatment is acceptable for minor burn-wound cellulitis in healthy patients aged 2 to 60 years; hospitalization is indicated for other infections.
Treatment references
1. Pham TN, Cancio CL, Gibran NS: American Burn Association practice guidelines burn shock resuscitation. J Burn Care Res J 29(1):257-266, 2008. doi: 10.1097/BCR.0b013e31815f3876
2. Eljaiek R, Heylbroeck C, Dubois MJBurns 43(1):17-24, 2017. doi: 10.1016/j.burns.2016.08.001
3. Greenhalgh DG, Cartotto R, Taylor SL: Burn resuscitation practices in North America: Results of the Acute Burn ResUscitation Multicenter Prospective Trial (ABRUPT). Ann Surg 10.1097/SLA.0000000000005166, 2021. doi: 10.1097/SLA.0000000000005166.
4. Navickis RJ, Greenhalgh DG, Wilkes MMJ Burn Care Res 37(3):e268-278, 2016. doi: 10.1097/BCR.0000000000000201
5. Kagan RJ, Peck MD, Ahrenholz DH, et al: Surgical management of the burn wound and use of skin substitutes: An expert panel white paper. J Burn Care Res 34:e60–79, 2013. doi: 10.1097/BCR.0b013e31827039a6
6. International Society for Burn Injury (ISBI) Practice Guidelines Committee: Steering Committee; Advisory Committee. ISBI Practice Guidelines for Burn Care. Burns 42(5):953-1021, 2016. doi: 10.1016/j.burns.2016.05.013
Key Points
Clues to burn depth include presence of vesicles or bullae (suggesting a partial-thickness burn); and decreased sensation, dry leathery eschar, hypoesthesia, and ability to easily pull hairs (suggesting a full-thickness burn).
If partial or full-thickness burns are > 10% TBSA, give IV lactated Ringer's solution at an initial rate guided by the Parkland formula (4 mL/kg × %TBSA burned during the first 24 hours after the burn) and adjusted based on hourly urine output.
For eschars that are circumferential or constricting, consider escharotomy.
Supportive measures include adequate analgesia and, if burns are > 20% TBSA, early nutritional support.
Strongly consider burn center consultation if burns involve the hands, feet, or perineum (partial-thickness or deeper); are> 5% TBSA (partial-thickness or deeper); are > 1% TBSA (full-thickness); or if patients are> 60 years or < 2 years of age or are unlikely to fully adhere to home care measures.
Treat surgically if an eschar is present, compartmental pressure is > 30 mm Hg, or, usually, if burns are full or deep partial-thickness.
For infections, apply topical antimicrobials (for prevention); routinely inspect burns (for early diagnosis of complications); and use systemic antibiotics, change topical treatment as needed, and occasionally excise the infected area (for treatment).
Begin physical and occupational therapy early to minimize scarring and contractures.






